Improving 13C-urea breath test performance metrics for diagnosis of Helicobacter pylori infection
Paula Mantero, Germán Rodolfo Flekenstein, Mariana Andrea Janjetic, Julián Andrés Fuda, Horacio Emilio Torti, Gustavo Cernadas, Marcela Beatriz Zubillaga, Cinthia Gabriela Goldman

TL;DR
This study shows that the 13C-urea breath test is highly accurate for diagnosing and monitoring Helicobacter pylori infection in adults.
Contribution
The study evaluates and optimizes the 13C-urea breath test's cut-off value for improved diagnostic accuracy in a specific population.
Findings
The 13C-UBT showed high sensitivity (93.0%) and specificity (95.6%) for initial diagnosis of H. pylori.
When compared to histology and PCR, the test achieved 98.8% sensitivity and 98.3% specificity.
The test was also highly effective (94.4% sensitivity, 100% specificity) for confirming H. pylori eradication post-treatment.
Abstract
The 13C-Urea Breath Test (13C-UBT) is a popular, non-invasive method used for the diagnosis of Helicobacter pylori infection. This work evaluates its performance for the initial diagnosis and post-treatment follow-up in dyspeptic adults from Buenos Aires, Argentina. We retrospectively analyzed data from two earlier studies, which evaluated H. pylori infection using 13C-UBT and histology of gastric biopsies. Additionally, we assessed the 13C-UBT performance against the concordant results of both histology and PCR in a subsample with available data. The 13C-UBT was performed using a commercial kit, with isotope-ratio-mass-spectrometry (IRMS) as the measurement technique. Results from 154 volunteers were evaluated to assess the performance of 13C-UBT for the initial diagnosis of H. pylori infection, with histological evaluation as the reference method. For a cut-off value set at 3.5‰,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
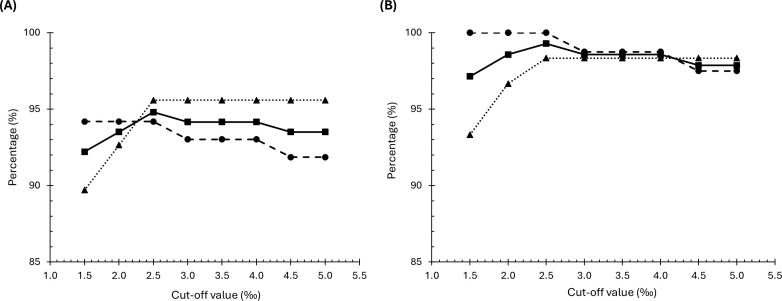 Figure 1
Figure 1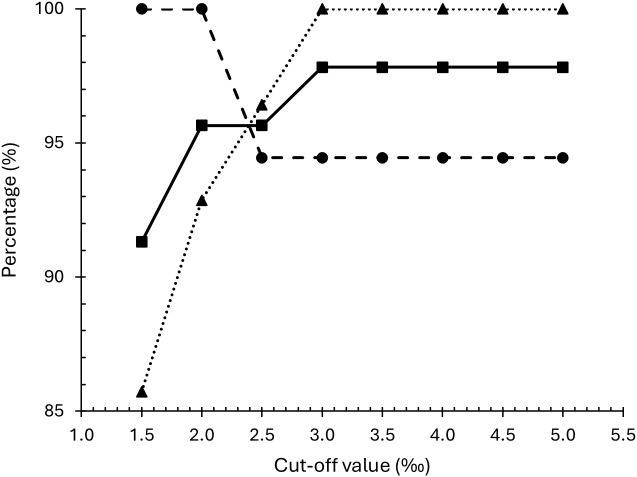 Figure 2
Figure 2| Cut-off DOB (‰) | True positive ( | True negative ( | False positive ( | False negative ( | Sensitivity (%) | Specificity (%) | Accuracy (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1.5 | 81 | 61 | 7 | 5 | 94.2 | 89.7 | 92.2 | 92.0 | 92.4 |
| 2.0 | 81 | 63 | 5 | 5 | 94.2 | 92.6 | 93.5 | 94.2 | 92.6 |
| 2.5 | 81 | 65 | 3 | 5 | 94.2 | 95.6 | 94.8 | 96.4 | 92.9 |
| 3.0 | 80 | 65 | 3 | 6 | 93.0 | 95.6 | 94.2 | 96.4 | 91.5 |
| 3.5 | 80 | 65 | 3 | 6 | 93.0 | 95.6 | 94.2 | 96.4 | 91.5 |
| 4.0 | 80 | 65 | 3 | 6 | 93.0 | 95.6 | 94.2 | 96.4 | 91.5 |
| 4.5 | 79 | 65 | 3 | 7 | 91.9 | 95.6 | 93.5 | 96.3 | 90.3 |
| 5.0 | 79 | 65 | 3 | 7 | 91.9 | 95.6 | 93.5 | 96.3 | 90.3 |
| Cut-off DOB (‰) | True positive ( | True negative ( | False positive ( | False negative ( | Sensitivity (%) | Specificity (%) | Accuracy (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1.5 | 80 | 56 | 4 | 0 | 100.0 | 93.3 | 97.1 | 95.2 | 100.0 |
| 2.0 | 80 | 58 | 2 | 0 | 100.0 | 96.7 | 98.6 | 97.6 | 100.0 |
| 2.5 | 80 | 59 | 1 | 0 | 100.0 | 98.3 | 99.3 | 98.8 | 100.0 |
| 3.0 | 79 | 59 | 1 | 1 | 98.8 | 98.3 | 98.6 | 98.8 | 98.3 |
| 3.5 | 79 | 59 | 1 | 1 | 98.8 | 98.3 | 98.6 | 98.8 | 98.3 |
| 4.0 | 79 | 59 | 1 | 1 | 98.8 | 98.3 | 98.6 | 98.8 | 98.3 |
| 4.5 | 78 | 59 | 1 | 2 | 97.5 | 98.3 | 97.9 | 98.7 | 96.7 |
| 5.0 | 78 | 59 | 1 | 2 | 97.5 | 98.3 | 97.9 | 98.7 | 96.7 |
| Cut-off DOB (‰) | True positive ( | True negative ( | False positive ( | False negative ( | Sensitivity (%) | Specificity (%) | Accuracy (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1.5 | 18 | 24 | 4 | 0 | 100.0 | 85.7 | 91.3 | 81.8 | 100.0 |
| 2.0 | 18 | 26 | 2 | 0 | 100.0 | 92.9 | 95.7 | 90.0 | 100.0 |
| 2.5 | 17 | 27 | 1 | 1 | 94.4 | 96.4 | 95.7 | 94.4 | 96.4 |
| 3.0 | 17 | 28 | 0 | 1 | 94.4 | 100.0 | 97.8 | 100.0 | 96.6 |
| 3.5 | 17 | 28 | 0 | 1 | 94.4 | 100.0 | 97.8 | 100.0 | 96.6 |
| 4.0 | 17 | 28 | 0 | 1 | 94.4 | 100.0 | 97.8 | 100.0 | 96.6 |
| 4.5 | 17 | 28 | 0 | 1 | 94.4 | 100.0 | 97.8 | 100.0 | 96.6 |
| 5.0 | 17 | 28 | 0 | 1 | 94.4 | 100.0 | 97.8 | 100.0 | 96.6 |
- —Universidad de Buenos Aires 10.13039/501100005363
- —Agencia Nacional de Promoción de la Investigación, el Desarrollo Tecnológico y la Innovación 10.13039/501100021778
- —International Atomic Energy Agency 10.13039/501100004493
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Gastroesophageal reflux and treatments · Gastric Cancer Management and Outcomes
Introduction
1
Helicobacter pylori is a Gram-negative, microaerophilic bacterium that affects, on average, about half of the world’s population (1, 2). This spiral-shaped microorganism colonizes the human gastric mucosa, causing chronic gastritis. Although most infected subjects are asymptomatic, approximately 10-15% may develop more severe pathologies such as dyspepsia, peptic ulcer disease, gastric cancer and mucosa-associated lymphoid tissue lymphoma (3).
Successful colonization and persistence in the hostile gastric environment are possible through different mechanisms. Flagellar motility, chemotaxis, adhesin expression, and immunomodulation allow H. pylori to migrate across the mucus layer from the stomach lumen to the gastric epithelium (4). Another crucial factor for H. pylori survival is the production of urease, an enzyme that hydrolyzes urea to carbon dioxide and ammonia, neutralizing gastric acidity. This change in pH both alters the mucus viscosity, which facilitates motility, and creates a gradient that helps H. pylori orient away from the lumen (3, 5).
The ^13^C-Urea Breath Test (^13^C-UBT) is a popular non-invasive method used for the initial diagnosis of H. pylori infection as well as for post-treatment eradication control (2, 6, 7). It is based on the urease activity of this microbe and involves the administration of ^13^C-labeled urea and the subsequent measurement of Carbon Isotope Ratio (CIR; ^13^CO_2_/^12^CO_2_ or Δ^13^CO_2_ per mil) in an exhaled breath sample, where ^13^CO_2_ enrichment over a cut-off value reflects the presence of H. pylori. Our research group has used this methodology in research projects (8–14) and technology transfer services in various clinical settings, assessing CIR by mass spectrometry.
Given the critical importance of local validation for diagnostic tests (7, 15), the aim of this study was to evaluate the performance of the ^13^C-UBT compared to histopathological diagnosis of H. pylori in adult patients with dyspepsia, both for initial diagnosis and post-treatment control in a population from Buenos Aires city, Argentina.
Method
2
We retrospectively analyzed data from a cross-sectional study and a longitudinal research project conducted by our laboratory (13, 14). Both protocols included dyspeptic adults (18–70 years) who were fasting overnight and had an indication for upper gastrointestinal (GI) endoscopy. Exclusion criteria included: active GI bleeding, prior GI surgery, neoplastic disease, diabetes, celiac disease, thyroid, renal, or hepatic pathologies, drug abuse, coagulopathies, pregnancy, previous H. pylori treatment, and use of antimicrobials or acid suppressants 4 weeks before enrollment. All volunteers signed a written informed consent. These protocols were approved by the Ethics Committee of the participating institutions and were performed in accordance with the principles of the Declaration of Helsinki and the Guidelines for Good Clinical Practice.
H. pylori status was evaluated by ^13^C-UBT and histological examination of gastric biopsies. The ^13^C-UBT was performed using a commercial kit (TAU-KIT, Isomed Pharma S.L., Madrid, Spain), as previously described (14). Basal breath samples were collected 10 minutes after ingestion of 100 mL citric acid solution (17.2 g/L). Then, 50 mL of an aqueous solution containing 100 mg ^13^C-labeled urea was administered and post-^13^C-urea breath samples were obtained after 30 minutes, according to the manufacturer’s specifications. CIR was measured in our laboratory using an isotope-ratio mass spectrometer (IRMS) coupled with a gas chromatograph (Finnigan-MAT GmbH, ThermoQuest Corp., Bremen, Germany) and subsequently compared to an international standard for carbon isotopic composition (VPDB) to calculate the delta 13 PDB (Del 13 PDB). The parameter used to assess ^13^CO_2_ enrichment was the Delta Over Baseline (DOB), calculated as the algebraic difference between the Del 13 PDB in the post-^13^C-urea samples and the basal samples, with a cut-off value set at 3.5‰ for H. pylori infection diagnosis (6, 16).
The endoscopic procedure was performed 1 to 2 hours after the ^13^C-UBT. A total of four gastric biopsies were obtained, with two samples collected from the antrum and two from the body. One biopsy from each site was used for histological examination. Briefly, “biopsies were processed by formalin immersion for 2 h, dehydration in 96% ethanol for 6 h, 100% ethanol for 4 h and xylene for 3 h, with immersion in paraffin at 56-58°C for 3 h and at 62°C for 3 h. Consecutive 4 μm sections were obtained using a spin tissue processor (MicromSTP120, ThermoScientific Corp., Walldorf, Germany) for hematoxylin-eosin and Giemsa histologic staining” (14). Microscopic assessment diagnosed H. pylori infection if curved rods were identified in one or both samples. The two remaining biopsies were reserved for molecular analysis by polymerase chain reaction (PCR). Bacterial DNA was isolated from the biopsies using the QIAamp Mini Kit (QIAGEN, INC., CA, United States). H. pylori infection was evaluated by amplification of the s-region of the vacA gene, which is present in all H. pylori strains. Primers va1F (5’-ATGGAAATACAACAAACACAC-3’) and va1XR (5’-CCTGAGACCGTTCCTACAGC-3’) were used, yielding a product of 176 bp for vacA s1 allele and 203 bp for type s2 variants (17). The PCR mixture contained 1X Taq polymerase buffer, 1.5 mM MgCl_2_, 0.2 mM each deoxynucleotide, 1.0 U of Platinum^®^ Taq DNA Polymerase (Invitrogen Argentina, Buenos Aires, Argentina), 0.1 μg each oligonucleotide primer, and 5 μL of DNA template in a total volume of 50 μL. PCR incubation was performed in an automatic thermocycler (MyCycler, BioRad, CA, United States) with an initial denaturation for 3 min at 94°C, followed by 35 cycles of 30 s at 94°C, 45 s at 50°C, and 45 s at 72°C, and a final extension at 72°C for 5 min. A 10 μL aliquot was analyzed by electrophoresis on a 1.5% agarose gel stained with ethidium bromide, and the PCR products were visualized under UV light, as previously described (13, 14).
The sensitivity, specificity, accuracy, positive predictive value (PPV) and negative predictive value (NPV) of the ^13^C-UBT for initial diagnosis were calculated from the cross-sectional study data using Giemsa staining histology as a reference method and concordant histology and PCR results in a sub-sample set. Meanwhile, the results from the longitudinal protocol allowed us to estimate these same parameters for the ^13^C-UBT as a post-treatment control diagnostic method. We further evaluated these performance metrics by setting different cut-off points ranging from 1.5‰ to 5.0‰ to include the gray zone associated with inconclusive ^13^C-UBT results (6, 16, 18). We used the GraphPad Prism (Version 8.0.1, December 2018, Boston, Massachusetts, United States) to compute the 95% confidence interval (CI95%) of the proportions through the hybrid Wilson/Brown method (19, 20).
Results
3
Data from 163 volunteers enrolled between 2012 and 2015 (13) were processed to evaluate the ^13^C-UBT for the initial diagnosis of H. pylori infection. We excluded 9 patients lacking the histology report. The median age of the included participants was 40.0 years (IQR, 27.8-51.0 y), 58.4% (CI95%, 50.5%-65.9%) were female, and the prevalence of H. pylori infection, as estimated by histopathology, was 55.8% (CI95%, 48.0%-63.5%). The test performance characteristics were calculated for a cut-off value of 3.5‰, as is usually set in our laboratory. The results were as follows: sensitivity 93.0% (CI95%, 85.6%-96.8%), specificity 95.6% (CI95%, 87.8%-98.8%), accuracy 94.2% (CI95%, 89.3%-96.9%), PPV 96.4% (CI95%, 89.9%-99.0%) and NPV 91.5% (CI95%, 82.8%-96.1%).
The DOB results allowed us to assess the test performance for different cut-off values, ranging from 1.5‰ to 5.0‰. Table 1 summarizes the sensitivity, specificity, accuracy, PPV, and NPV calculated for each cut-off. A cut-off of 2.5‰ maximized all these parameters, resulting in the best performance for the test, as shown in Figure 1A.
Sensitivity (•), specificity (▴) and accuracy (▪) of 13C-UBT at different cut-off values for initial diagnosis of H. pylori infection compared to histology (A) and concordant histology and PCR (B).
Given the limitations of histology as an exclusive diagnostic method for H. pylori infection, we analyzed the performance of the ^13^C-UBT by comparing it to concordant histology and PCR results in our cross-sectional study. One of the patients lacked PCR results, and 13 had non-concordant results between histology and PCR: specifically, 8 individuals had a negative H. pylori diagnosis by histology but a positive PCR result, while 5 were considered positive by histology with no amplification by PCR. This population of 140 adults had a median age of 41.0 years (IQR, 27.0-51.0 y), 57.1% (95% CI, 48.9%-65.0%) were female and H. pylori infection had a prevalence of 57.1% (95% CI, 48.9%-65.0%).
The test performance metrics of ^13^C-UBT against the combined histology and PCR reference were improved compared to the metrics when compared against histology alone. The calculated sensitivity was 98.8% (95% CI, 93.3%-99.9%), specificity was 98.3% (95% CI, 91.1%-99.9%), accuracy was 98.6% (95% CI, 94.9%-99.7%), PPV was 98.8% (95% CI, 93.3%-99.9%) and NPV was 98.3% (95% CI, 91.1%-99.9%). These parameters were also higher when calculated at different cut-off values, as shown in Table 2. Consistent with the previous analysis, the best accuracy was observed at a cut-off value of 2.5‰ (Figure 1B).
We also evaluated the performance of the ^13^C-UBT for the post-treatment control of H. pylori after eradication treatment. This analysis was based on data from a longitudinal study conducted between 2015 and 2017 (14), which included 46 subjects who were initially diagnosed with the infection, underwent antimicrobial therapy, and subsequently returned for follow-up. The median age of this group was 47.5 (IQR, 35.8-55.3) years, and 63.0% (95% CI, 48.6%-75.5%) were female. Based on histopathology, the prevalence of H. pylori infection was 39.1% (95% CI, 26.4%-53.5%).
In this context, the ^13^C-UBT showed a sensitivity of 94.4% (95% CI, 74.2%-99.7%), a specificity of 100.0% (95% CI, 87.9%-100.0%), an accuracy of 97.8% (95% CI, 88.7%-99.9%), a PPV of 100.0% (95% CI, 81.6%-100.0%) and a NPV of 96.6% (95% CI, 82.8%-99.8%). These parameters were also calculated at different cut-off values, as detailed in Table 3. Under these circumstances, a value of 3.0‰ was the lowest cut-off to achieve 100% specificity and PPV, with sensitivity, accuracy and NPV all exceeding 94%. At a cut-off of 2.5‰, both specificity and accuracy decreased without improving sensitivity. Further reductions in the cut-off resulted in a sensitivity of 100%, but a sharp decline in specificity (Figure 2).
Sensitivity (•), specificity (▴) and accuracy (▪) of 13C-UBT at different cut-off values for H. pylori infection control after-treatment compared to histology.
Discussion
4
The ^13^C-UBT is a safe, non-invasive and widely used diagnostic method with high sensitivity and specificity for the initial diagnosis of H. pylori infection as well as for the control after eradication treatment (2). Local validation is recommended as demographic characteristics may vary across populations, and several test parameters can affect its outcome, including the ^13^C-urea dose, the chosen cut-off value, the sampling time after ^13^C-urea administration, the type of test meal and the measuring equipment (7). Based on results from two previous studies conducted by our research group, we evaluated the performance of ^13^C-UBT in patients from Buenos Aires city using a commercial kit (TAU-KIT).
The test demonstrated a robust performance, both for the initial diagnosis of H. pylori infection and for confirming eradication after treatment, under the conditions used in our study. These conditions included initial citric acid intake, a 100 mg ^13^C-urea dose in an aqueous solution, 30 minutes sampling time after urea ingestion, assessment using IRMS, and 3.5‰ cut-off value. However, our analysis of sensitivity, specificity and accuracy at different cut-off values -when evaluating ^13^C-UBT against histology alone and the combined concordant results of histology and PCR- revealed that for initial diagnosis of H. pylori infection the cut-off could be lowered to 2.5‰. This adjustment increased the sensitivity without compromising the specificity, thus improving accuracy. Further reducing the cut-off value, however, did not result in any additional increase in sensitivity but caused a drop in the specificity. In contrast, for post-treatment control, a 3.0‰ cut-off provided the best accuracy; lowering it to 2.5‰ maintained sensitivity but led to a decrease in specificity, thereby reducing accuracy. These outcomes led us to select 3.0‰ as the most appropriate cut-off value for use in our experimental setup.
It is important to highlight that, in this study, these test performance metrics were initially estimated using histology as the gold standard, even though it is widely known that it has both advantages and disadvantages, as any other reference method. In this case, histology limitations may be related to the patchy distribution of H. pylori and the varying bacterial density within the gastric mucosa. This can result in a sampling error, as well as interobserver variability due to differences in the pathologists’ expertise in identifying the microorganism (21). Despite these limitations, ^13^C-UBT performance values for initial diagnosis of H. pylori infection observed in this study are consistent with those reported in systematic reviews and meta-analyses of this technique (22). Furthermore, performance metrics of the ^13^C-UBT improved even more when we used two coincident diagnostic methods, histology and PCR, as a gold standard (7, 23).
A key strength of our study was that it also evaluated the ^13^C-UBT for post-treatment assessment, which yielded enhanced performance metrics. In this analysis, the reference method was restricted to histology due to a lack of PCR results for many participants in this cohort, which we acknowledge as a potential limitation.
Our investigation enrolled adult dyspeptic patients from the urban region of Buenos Aires. The prevalence of H. pylori infection within this study population aligns with rates reported for symptomatic individuals in urban areas of other Argentine provinces (24–29), thus supporting the broader applicability of our optimized cut-off to these demographically similar groups. Nevertheless, the optimized ^13^C-UBT cut-off may not be universally applicable. Its utility could be limited in other Latin American populations exhibiting higher H. pylori prevalences (30, 31), or in the diagnosis of infection in pediatric cases, where variables such as a reduced ^13^C-urea dose could impact DOB values.
The relevance of improving the performance metrics of the ^13^C-UBT lies in its ability to avoid both missed infections and unnecessary antibiotic exposure. Reducing false negative results may prevent the progression of gastrointestinal pathologies associated with H. pylori infection that could lead to the development of gastric cancer, with the resulting decrease in healthcare costs related to severe outcomes. Conversely, lowering false-positive results may reduce antibiotic misprescription, thereby mitigating the emergence of antimicrobial resistance (2).
This study shows that the ^13^C-UBT is highly sensitive and specific for both the initial diagnosis and for the post-treatment assessment of H. pylori infection, with its only drawback being the economic cost. The high accuracy of this non-invasive test, together with its simplicity and its capacity to detect active infection by evaluating the entire gastric mucosa, makes it a method of choice whenever the technology is available.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zamani M Ebrahimtabar F Zamani V Miller WH Alizadeh-Navaei R Shokri-Shirvani J. Systematic review with meta-analysis: the worldwide prevalence of Helicobacter pylori infection. Aliment Pharmacol Ther. (2018) 47:868–76. doi: 10.1111/apt.14561, PMID: 29430669 · doi ↗ · pubmed ↗
- 2Malfertheiner P Megraud F Rokkas T Gisbert JP Liou JM Schulz C. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. (2022) 71:1724–62. doi: 10.1136/gutjnl-2022-327745, PMID: 35944925 · doi ↗ · pubmed ↗
- 3Robinson K Letley DP Kaneko K. The human stomach in health and disease: Infection strategies by Helicobacter pylori . Curr Top Microbiol Immunol. (2017) 400:1–26. doi: 10.1007/978-3-319-50520-6_1, PMID: 28124147 · doi ↗ · pubmed ↗
- 4De Brito BB Da Silva FAF Soares AS Pereira VA Cordeiro Santos ML Sampaio MM. Pathogenesis and clinical management of Helicobacter pylori gastric infection. World J Gastroenterol. (2019) 25:5578–89. doi: 10.3748/wjg.v 25.i 37.5578, PMID: 31602159 PMC 6785516 · doi ↗ · pubmed ↗
- 5Salama NR Hartung MLMüller A. Life in the human stomach: Persistence strategies of the bacterial pathogen Helicobacter pylori . Nat Rev Microbiol. (2013) 11:385–99. doi: 10.1038/nrmicro 3016, PMID: 23652324 PMC 3733401 · doi ↗ · pubmed ↗
- 6Gisbert JP Pajares JM. Review article 13C-urea breath test in the diagnosis of Helicobacter pylori - a critical review. Aliment Pharmacol Ther. (2004) 20:1001–17. doi: 10.1111/j.1365-2036.2004.02203.x, PMID: 15569102 · doi ↗ · pubmed ↗
- 7Miftahussurur M Yamaoka Y. Diagnostic methods of Helicobacter pylori infection for epidemiological studies: critical importance of indirect test validation. Bio Med Res Int. (2016) 2016:1–14. doi: 10.1155/2016/4819423, PMID: 26904678 PMC 4745376 · doi ↗ · pubmed ↗
- 8Goldman C Barrado A Janjetic M Balcarce N Rua EC Oshiro M. Factors associated with H pylori epidemiology in symptomatic children in Buenos Aires, Argentina. World J Gastroenterol. (2006) 12:5384–8. doi: 10.3748/wjg.v 12.i 33.5384, PMID: 16981273 PMC 4088210 · doi ↗ · pubmed ↗