Case Report: A novel approach to pseudoportomesenteric hypertension with refractory chylothorax and ascites
Ahmet Sakiri, Annalise De Marco, Shreekar Patel, Naser Khan, Thayer Hamoudah, Altaf Dawood, Rajesh Kakarla

TL;DR
This case report describes a rare condition called pseudoportomesenteric hypertension caused by a pancreatic tumor, and how stent placement helped reduce severe symptoms.
Contribution
The paper presents a novel case of pseudoportomesenteric hypertension caused by a pancreatic neuroendocrine tumor and its successful palliative endovascular treatment.
Findings
Stent placement in the superior mesenteric vein reduced pressure gradient and resolved varices.
The patient had a well-differentiated grade 2 pancreatic neuroendocrine tumor confirmed by biopsy.
Palliative endovascular intervention improved antegrade hepatopetal flow in a patient with refractory chylothorax and ascites.
Abstract
Pseudoportomesenteric hypertension (PPMH) is a rare form of non-cirrhotic portal hypertension caused by increased pressure in the portal and mesenteric venous systems. Unlike traditional portal hypertension, which arises from liver cirrhosis, PPMH stems from conditions that are extrahepatic in etiology, such as venous thrombosis, external compression by intra-abdominal masses, or congenital anomalies. Treatment is aimed at addressing the underlying cause of obstruction. We report a case of PPMH secondary to a pancreatic neuroendocrine tumor (PNET). A female in her 60s presented with a six-month history of diarrhea, 30-pound weight loss, and dyspnea. Initial evaluation revealed massive right pleural effusion with subtotal lung collapse, cardio-mediastinal shift, and sub-segmental pulmonary emboli. Additionally, she had extensive four-quadrant ascites and a heterogeneous mass at the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
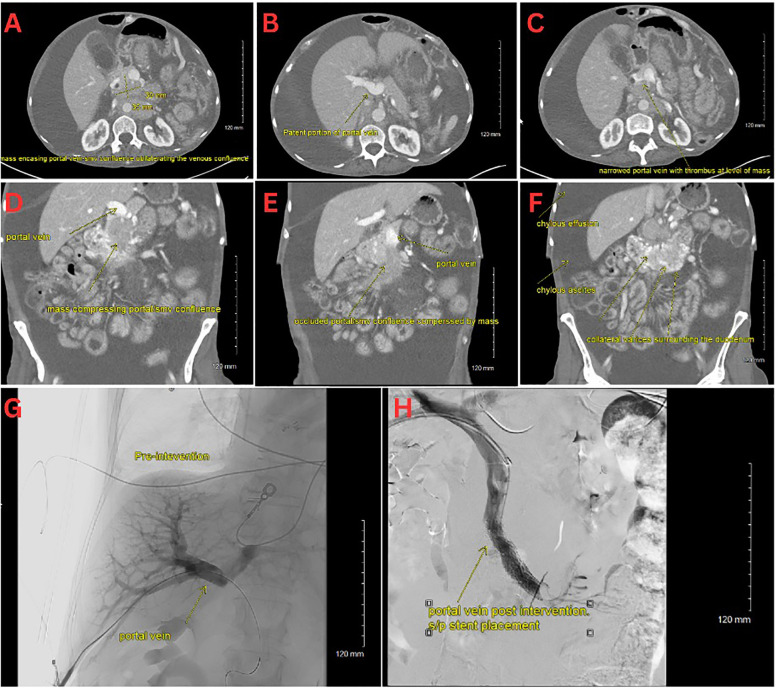 Figure 1
Figure 1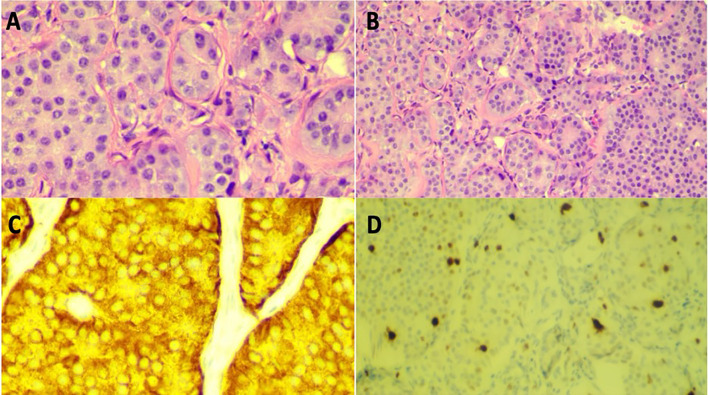 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Lymphatic Disorders and Treatments · Intestinal Malrotation and Obstruction Disorders
Introduction
Pseudoportomesenteric hypertension (PPMH) is a rare form of non-cirrhotic portal hypertension caused by extrahepatic compression or obstruction of the mesenteric or portal venous system. When the superior mesenteric vein (SMV) or portal vein is compressed by tumor or lymphadenopathy, patients can develop refractory ascites, variceal formation, and chylous effusions. Pancreatic masses, including pancreatic neuroendocrine tumors (pNETs), can lead to compression and significantly elevate portal pressures (1). We present a case of unresectable pNET causing SMV obstruction and subsequent pseudoportomesenteric hypertension, resulting in massive ascites and chylothorax. We highlight the successful use of an SMV stent to palliate refractory fluid collections and improve the patient’s quality of life.
Case report
A woman in her 60s, with a known carrier status for cystic fibrosis and newly diagnosed exocrine pancreatic insufficiency, presented to the emergency department with a six-month history of loose frothy bowel movements, progressive fatigue, exertional dyspnea, and a 30-pound unintentional weight loss. She reported frequent small-volume bowel movements with associated urgency, tenesmus, hypogastric cramping, and occasional streaks of blood on wiping. Additionally, she noted early satiety, post-prandial bloating, and abdominal distension.
On initial evaluation, she appeared cachectic, tachycardic (110 bpm), tachypneic, and had an oxygen saturation of 87% on room air. She had conjunctival pallor, severely diminished breath sounds on the right side, massive abdominal distension with diffuse dullness to percussion, and bilateral pitting edema extending to the thighs. Notable laboratory results included mild thrombocytosis (platelets 471 x 10^3/µL), hypokalemia (K 2.7 mmol/L), hypoalbuminemia (3.2 g/dL), and hypomagnesemia (0.9 mg/dL), and an elevated troponin levels (28, 27, 24 ng/L). A chest CT showed a massive right pleural effusion with leftward cardio-mediastinal shift and near-complete right lung collapse. Additionally, segmental pulmonary emboli were found in the left lower lobe (Figures 1A–F). Abdominal CT revealed a heterogeneous pancreatic head/uncinate mass with encasement of the superior mesenteric artery (SMA) and mass effect on the SMV, retroperitoneal lymphadenopathy, and sclerotic bone lesions.
Due to marked ascites, a paracentesis was performed that demonstrated a serum-ascites albumin gradient (SAAG) of 2.3, suggesting portal hypertension. Cytology was negative for malignant cells. After chest tube placement, the pleural fluid eventually became milky, with triglyceride levels of 343 mg/dL, confirming chylothorax. She required frequent large-volume paracenteses and chest tube drainage for refractory ascites and chylothorax.
Biopsy options for the pancreatic mass were limited by large duodenal varices. Thus, a CT-guided retroperitoneal lymph node biopsy was performed, confirming a well-differentiated grade 2 pancreatic neuroendocrine tumor (Figure 2). Ultrasound duplex of the abdomen and pelvis was conducted to assess mesenteric vessel flow. This revealed significant hemodynamic stenosis exceeding 70% at the distal superior mesenteric artery, consistent with prior cross-sectional imaging demonstrating narrowing and encasement by a mass in the pancreatic head and uncinate process. Additionally, marked splanchnic hypertension was noted, with evidence of hemodynamically significant obstruction at the portal-mesenteric confluence.
Interventional radiology performed a transhepatic portal venogram, demonstrating a 20 cm H2O gradient across the SMV obstruction, along with extensive varices. A 12 mm x 60 mm self-expanding stent was deployed, reducing the gradient from 20 to 10 cm H2O and restoring antegrade hepatopetal flow (Figures 1G–H). Post-procedure, her abdominal distension, and chylothorax gradually improved, and large-volume paracenteses were no longer required. She was started on total parenteral nutrition (TPN) and long-acting octreotide for symptom management.
(A–C) CT scan with an axial view of the pNET mass. (D–F) CT scan with a coronal view of the pNET mass. (G) Venogram showing portal vein prior to stent deployment with no distal contrast visualized. (H) Venogram post SMV stent deployment with subsequent patency.
A Ga68-DOTATATE PET/CT confirmed SSTR2-positive pancreatic head mass, with hepatic and osseous metastases. She was started on capecitabine and temozolomide chemotherapy, but tolerability issues led to early discontinuation. She continued octreotide with plans for routine imaging follow-up.
(A) High power (20x) view of H&E stain of retroperitoneal lymph node biopsy. (B) Low power (10x) view of H&E stain of retroperitoneal lymph node biopsy. (C) High power (20x) view Synaptophysin stain of lymph node biopsy in high power (20x) view. (D) Ki-67 positive stain (~4% positive), indicating well-differentiated grade 2 neuroendocrine tumor in low power (10x) view.
Discussion
Unlike cirrhosis, where increased intrahepatic resistance drives portal hypertension, pseudoportomesenteric hypertension constitutes a non-cirrhotic, prehepatic phenomenon arising from external compression of the portal or mesenteric venous system (2). Recognizing this distinction is crucial, as correcting the anatomical obstruction can alleviate symptoms and improve clinical outcomes. The superior mesenteric vein (SMV) is a critical component of the portal venous system, responsible for draining blood from the small intestine, cecum, and ascending colon and delivering nutrient-rich blood to the liver via its confluence with the splenic vein to form the portal vein. Any pathology that significantly narrows or occludes the SMV—such as tumor encasement—can precipitate a severe increase in splanchnic venous pressures.
In the presented case, a pancreatic neuroendocrine tumor encased the SMV, leading to significant luminal narrowing and obstruction of blood flow. This obstruction resulted in elevated splanchnic venous pressures, manifesting as refractory ascites and chylothorax due to increased hydrostatic pressure and subsequent fluid transudation into the peritoneal and pleural cavities. Symptoms can be refractory to medical therapy alone and require interventional relief of the obstruction.
Endovascular stenting offers a key palliative strategy for malignant SMV obstruction. By deploying a stent across the stenotic segment of the SMV, normal antegrade hepatopetal flow is reestablished, effectively reducing splanchnic hypertension. Maintaining SMV patency lowers the portomesenteric gradient, thereby diminishing fluid extravasation into the peritoneal and pleural spaces, allowing for the resolution of ascites and chylothorax. Additionally, restoring normal hemodynamics improved the patient’s quality of life by reducing abdominal distension, facilitating better oral intake, and decreasing reliance on paracentesis and total parenteral nutrition.
The successful outcome aligns with existing literature, which reports high technical success rates and significant symptom palliation in patients undergoing portal vein stenting for malignant obstructions. For instance, a single‐center, retrospective study by Shah et al. evaluated percutaneous transhepatic portal vein stenting (PVS) in 38 patients with pancreaticobiliary cancer and extrahepatic portomesenteric venous stenosis leading to refractory ascites or variceal bleeding (3). In the 28 patients treated primarily for these complications, PVS achieved a 93% technical success rate and sustained symptomatic relief for an average of 87% of the remaining patients. Stent patency correlated strongly with decreased ascites and stable liver volume, while no major or minor complications were observed (3). These findings underscore the potential of PVS to significantly improve the quality of life in this challenging clinical setting.
While surgical resection is ideal in localized disease, metastatic and vascularly encased tumors often preclude curative resection (4). Portal-SMV stenting is a low-risk procedure with a high clinical success rate that can provide a bridge to systemic therapies (e.g., octreotide, chemotherapy) and enhance quality of life (3). Somatostatin analogs like octreotide can slow tumor progression and reduce secretory outputs, while capecitabine–temozolomide may offer antiproliferative effects in well-differentiated pNETs (5). However, therapy must be individualized based on tolerance and patient goals.
This case underscores the importance of understanding the anatomical and physiological underpinnings of the portal venous system. It highlights the efficacy of SMV stenting as a therapeutic option for managing complications arising from malignant portal vein obstructions. Multidisciplinary care, incorporating interventional radiology, oncology, and gastroenterology, is essential in managing such cases to balance endovascular, medical, and oncological therapies. SMV stenting serves as a viable and effective intervention for patients with pseudoportomesenteric hypertension secondary to malignant obstruction, especially when surgical resection is not feasible, offering substantial improvements in clinical symptoms and overall quality of life. Future research should focus on identifying criteria for patient selection and timing of stent placement, as well as factors that may affect stent patency.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ro C Chai W Yu VE Yu R. Pancreatic neuroendocrine tumors: biology, diagnosis, and treatment. Chin J Cancer. (2013) 32:312–24. doi: 10.5732/cjc.012.10295, PMID: 23237225 PMC 3845620 · doi ↗ · pubmed ↗
- 2Gioia S Nardelli S Ridola L Riggio O. Causes and management of non-cirrhotic portal hypertension. Curr Gastroenterol Rep. (2020) 22:56. doi: 10.1007/s 11894-020-00792-0, PMID: 32940785 PMC 7498444 · doi ↗ · pubmed ↗
- 3Sheth RA Sabir SH Parmet P Amin R Kuban JD Huang SY. Portomesenteric venous stenting for palliation of ascites and variceal bleeding caused by prehepatic portal hypertension. Oncologist. (2018) 23:712–8. doi: 10.1634/theoncologist.2017-0337, PMID: 29284759 PMC 6067944 · doi ↗ · pubmed ↗
- 4Sulciner ML Clancy TE. Surgical management of pancreatic neuroendocrine tumors. Cancers (Basel). (2023) 15:2006. doi: 10.3390/cancers 15072006, PMID: 37046665 PMC 10093271 · doi ↗ · pubmed ↗
- 5Strosberg JR Fine RL Choi J Nasir A Coppola D Chen DT. First-line chemotherapy with capecitabine and temozolomide in patients with metastatic pancreatic endocrine carcinomas. Cancer. (2011) 117:268–75. doi: 10.1002/cncr.25425, PMID: 20824724 PMC 4665634 · doi ↗ · pubmed ↗