Successful treatment of low-flow-low-gradient aortic stenosis and complex coronary artery disease in a patient with severely depressed left-ventricular function by protected percutaneous coronary intervention and transfemoral transcatheter aortic valve replacement via Y-graft vascular prosthesis: a case report
Yusuf Nejahsie, Samer Hakmi, Stephan Willems, Wolfgang Tigges, Eike Tigges

TL;DR
A high-risk patient with severe heart conditions was successfully treated using a staged approach involving PCI and TAVR via a Y-graft, leading to symptom relief and improved heart function.
Contribution
Demonstrates the feasibility and safety of Impella®-supported PCI followed by TAVR via a Y-graft in a complex clinical scenario.
Findings
The patient experienced immediate symptom relief and improved ejection fraction after treatment.
Follow-up showed improved aortic valve function and sustained clinical benefits at 3 months.
The staged interventional approach was feasible and safe despite challenging transfemoral access.
Abstract
Low-flow, low-gradient aortic stenosis (LFLG AS) is a subset of aortic stenosis associated with a poor prognosis and high operative risk, particularly in the presence of concomitant coronary artery disease (CAD) requiring intervention. In patients considered inoperable, minimally invasive approaches often remain the only alternative. However, there are limited data on treatment strategies and outcomes in patients with LFLG AS and severe ischaemic cardiomyopathy undergoing percutaneous coronary intervention (PCI) and transcatheter aortic valve replacement (TAVR), especially in cases with challenging transfemoral access. An 87-year-old male presented with progressive dyspnoea and angina. Diagnostics revealed a non-ST-segment elevation myocardial infarction, acute heart failure, acute-on-chronic renal failure, LFLG AS (aortic valve area of 0.7 cm²), and a left ventricular ejection…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
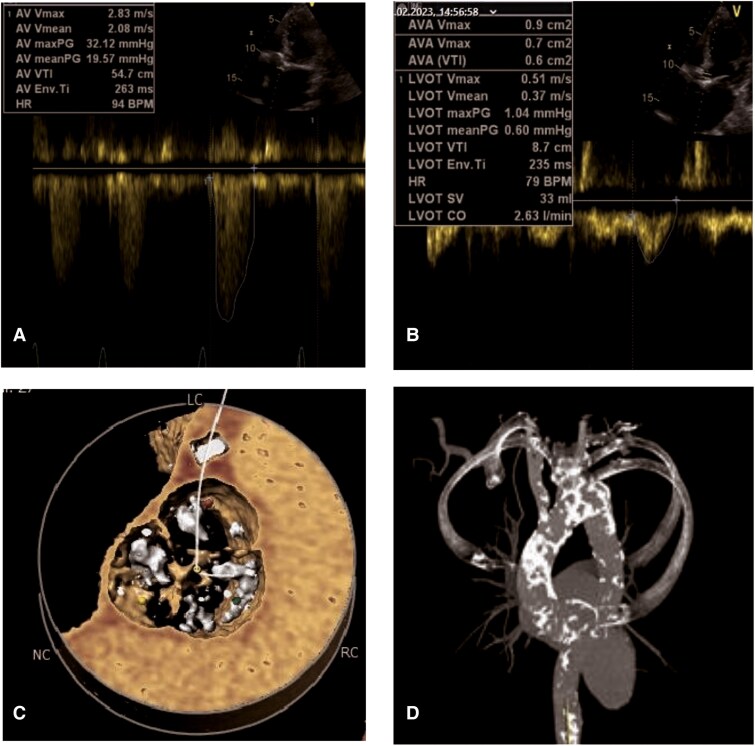 Figure 1
Figure 1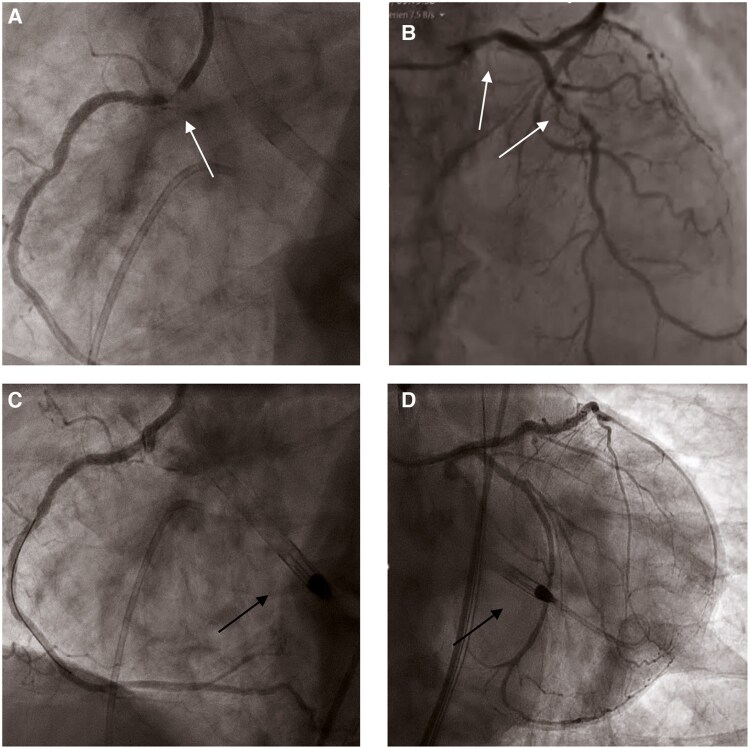 Figure 2
Figure 2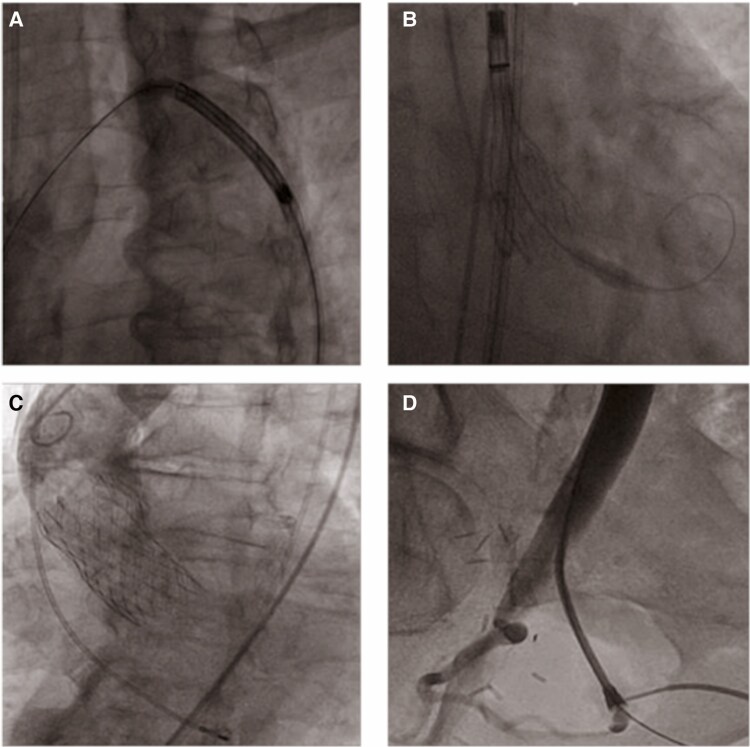 Figure 3
Figure 3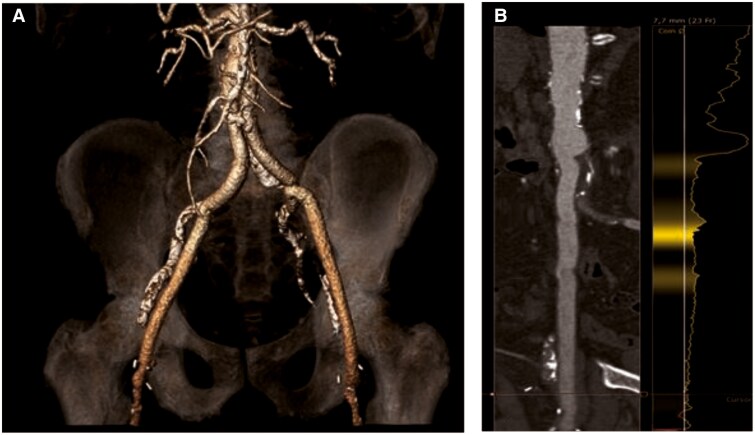 Figure 4
Figure 4| CLINICAL CASE OVERVIEW: |
Patient Profile: 87-year-old male with LFLG AS and severe ischaemic cardiomyopathy. Initial Presentation: Progressive dyspnoea and angina, diagnosed with NSTEMI, acute heart failure, and acute-on-chronic renal failure. Diagnostic Findings: Valve area 0.7 cm², mean aortic valve gradient of 20 mmHg, LVEF 10%. Severe stenoses in left main, left anterior descending, and right coronary arteries. Surgical Risk: High operative risk (EuroSCORE 14.9%, STS 9.7%) and porcelain aorta; deemed unsuitable for surgery. |
| Treatment Strategy: |
Day 1: Protected PCI High-risk PCI using Impella CP® via aortoiliac bypass graft. Successful revascularization with drug-eluting stents. Day 2: Transfemoral TAVR TAVR with 29-mm EVOLUT™ Pro Plus bioprosthesis. Transfemoral access via Y-graft; unilateral secondary access (≥2 cm distal to the delivery sheath); valve deployment under fast pacing. |
| Post-procedure Outcome: |
Immediate symptom relief; improved LV function (20%). Discharged on Day 6 with optimal medical therapy. Follow-up after 3 month with further improvement of LV function (35%); NYHA II and CCS 0 |
| Discussion Points: |
Feasibility of staged Impella-supported PCI and TAVR in LFLG AS. Challenges and considerations in PCI for patients with severe AS and LV dysfunction. Safety access in TAVR via femoral Y-graft Valve-type selection. |
| Conclusion: |
This case illustrates the feasibility and safety of a staged Impella-supported PCI before addressing the AS via transfemoral TAVR in spite of the presence of a femoral Y-graft in a patient with |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Cardiac and Coronary Surgery Techniques
Introduction
Low-flow, low-gradient aortic stenosis (LFLG AS) is a subset of aortic stenosis (AS) associated with a poor prognosis and high operative risk.^1^ This condition occurs when left ventricular (LV) systolic dysfunction coexists with severe AS, resulting in a reduced stroke volume index (SVI). Transcatheter aortic valve replacement (TAVR) is a well-established alternative to surgical aortic valve replacement, especially in patients considered inoperable or at high surgical risk. However, TAVR alone may not be sufficient to improve outcomes in patients with LFLG AS and concomitant coronary artery disease (CAD), as residual myocardial ischaemia may limit the recovery of LV function and increase the mortality risk.^1^
Percutaneous coronary intervention (PCI) in patients with AS and severely reduced LV ejection fraction (LVEF) is challenging. In this context, the use of mechanical circulatory support devices such as the Impella® has been shown to be safe and effective in cases of cardiogenic shock, high-risk PCI, and acute myocardial infarction.^2^ However, evidence supporting its use in patients with LFLG AS and severe ischaemic cardiomyopathy undergoing PCI and TAVR remains limited.^3^
Transfemoral access is the most commonly utilized approach for TAVR with a favorable safety profile.^4^ However, data on large-bore access in Y-graft bioprostheses remain limited.^5^
Here, we present a case of successful treatment of a patient with LFLG AS and severe ischaemic cardiomyopathy by staged Impella®-supported PCI and transfemoral TAVR via an aortofemoral bypass graft.
Summary figure
Educational Overview
**: **
Case presentation
An 87-year-old man with a history of hypertension, chronic kidney disease, atrial fibrillation, and peripheral arterial disease with bilateral aortoiliac bypass grafting (since 2012) was admitted due to progressive dyspnoea and angina. Upon admission, elevated serum levels of high-sensitive troponin (hsTnI) were identified, with a value of 548 ng/L (<34 ng/L),^6^ decreasing to 299 ng/L within a 3-h span. NT-proBNP was elevated to 12 803 ng/L (<450 ng/L),^6^ and creatinine to 2.6 mg/dL (0.7–1.2 mg/dL),^7^ with a baseline of 1.4 mg/dL due to chronic kidney disease. The ECG showed atrial fibrillation with a normal ventricular rate and absence of ST-segment elevations. Chest X-ray indicated pulmonary venous congestion. These findings were consistent with a non-ST-segment elevation myocardial infarction (NSTEMI) with heart failure and acute-on-chronic renal failure.
Further diagnostics demonstrated a mean aortic valve gradient of 20 mmHg, and a LVEF of 10%, resulting in an aortic valve area (AVA) of 0.7 cm² (Figure 1; Supplementary material online, Video S1–S3). Coronary angiography showed severe stenoses in the left main (LM), left anterior descending (LAD), and an ostial stenosis of the right coronary artery (RCA; Figure 2A and B; Supplementary material online, Video S4 and S5).
(A+B) Transthoracic echocardiography shows gradient measurements with a peak velocity of 2.83 m/s, a mean gradient of 19.57 mmHg, aortic valve area (measured by velocity time integral [VTI]) 0.6 cm2, and stroke volume (SV) 33 mL. (C) Hockey puck (VR)—Preprocedural CT scan showing severe aortic valve calcification. (D) Electrocardiography-gated cardiac computed tomography demonstrates severe calcification of the aorta ascendens–porcelain aorta.
(A and B) Coronary angiography shows severe stenosis of the left main, left anterior descending, and the right coronary artery. White arrows show the stenosis. (C and D) Final angiographic results after implantation of drug-eluting stents in the left main, left anterior descending artery, and the right coronary artery. Black arrows show the correctly positioned Impella CPR device (Abiomed, Danvers, MA, USA) in the left ventricular.
Given the patient’s clinical status and operative mortality risks (EuroSCORE 14.9%, STS 9.7%), the Heart Team recommended staged PCI followed by transfemoral TAVR. The patient provided informed consent after detailed discussion of risks and alternatives. On the first day, protected PCI of the LM, LAD and the RCA was performed via a 6-Fr sheath through the right radial artery. The Impella CP® was inserted via the vascular graft under fluoroscopic guidance, advanced across the calcified aortic valve, and maintained at 3.6 L/min throughout the procedure. Complete revascularization with drug-eluting stents was achieved (Figure 2C and D; Supplementary material online, Video S7 and S8). The patient remained stable without inotropic support, and the Impella CP® was removed immediately after the procedure.
The following day, TAVR was performed via the right femoral Y-graft using a self-expandable 29-mm EVOLUT™ Pro+ bioprosthesis under local anaesthesia and sedation. Haemostasis was achieved with a suture-based vascular closure system, and final angiography confirmed a patent Y-graft and a well-functioning valve without significant leak or gradient (Figure 3; Supplementary material online, Video S10 and S11).
(A) Fluoroscopic image of crossing the aortic arch with the EVOLUT™ delivery system. (B) Deployment of the EVOLUT™ Pro+ in the cusp overlap view. (C) Final aortogram after successful implantation of EVOLUT™ Pro+ bioprosthesis without periprosthetic leaks. (D) Final peripheral angiogram confirming a patent Y-graft with preserved blood flow without any stenosis.
Post-procedural monitoring was uneventful, without bleeding, renal impairment, or arrhythmias, including atrioventricular conduction disturbances. The patient was discharged on the sixth post-operative day with an improved LV function of 20% (see Supplementary material online, Video S12–S14).
An optimal heart failure medication regimen according to guidelines was initiated. At admission, the patient received a low-dose beta-blocker and a mineralocorticoid antagonist. Angiotensin receptor-neprilysin inhibitor and SGLT-2 inhibitor were added and titrated to maximum tolerated doses over 3 months. By then, LVEF improved from initially 10% to 35% (see Supplementary material online, Video S15–S17), symptoms improved to NYHA II/CCS 0, and NT-proBNP decreased from 12 803 to 5716 ng/L. Further follow-up could not be obtained, as the patient lives remotely and declined additional follow-ups.
Discussion
The diagnosis of LFLG AS relies on the AVA, transvalvular gradient, SVI, and contractile reserve assessed by dobutamine-stress echocardiography.^8^ Due to ongoing unstable angina with heart failure, dobutamine stress echocardiography was not performed. However, the patient`s clinical presentation, severe aortic valve calcification (3360 Agatston units; Figure 1C), and planimetry of AVA supported the diagnosis of severe AS.
PCI in patients with LFLG AS and severe LV dysfunction poses challenges such as contrast-induced nephropathy, haemodynamic instability during balloon inflation, and stent deployment.^9^ An Impella CP® device was employed for mechanical circulatory support; although data remain limited in this population, smaller studies demonstrate its feasibility and safety.^10^ Regarding valve choice, balloon-expandable bioprostheses may facilitate coronary re-access. However, a self-expandable valve was chosen in this case to reduce the risks associated with rapid ventricular pacing due to the patient’s compromised haemodynamics and to better accommodate annular calcification with lower radial force, thereby minimizing rupture risk.
PCI was prioritized to address the urgency of NSTEMI management, avoid crossing the Impella CP® through a newly implanted valve, and mitigate risks of bioprosthetic valve damage or migration.
Complete revascularization was pursued, given the patient’s balanced coronary supply pattern in the setting of multivessel disease. The presenting symptom of angina was attributed to complex CAD, necessitating a comprehensive treatment strategy. Despite the patient’s advanced age and comorbidities, he had maintained an independent lifestyle until admission, when progressive angina and functional decline developed. Partial revascularization was unlikely to sufficiently reduce ischaemic burden, potentially impairing LV recovery and limiting TAVR benefits. Complete revascularization aimed to stabilize haemodynamics and reduce future coronary risks, especially due to challenging coronary access after TAVR with a supra-annular bioprosthesis. Overall, this strategy was chosen—taking into account the patient’s preference—to optimize both immediate and long-term clinical outcomes in this high-risk patient.
Limited evidence exists regarding transfemoral TAVR via prosthetic grafts. However, in our case, the decision to proceed transfemorally was supported by CT angiography, which confirmed a sufficient Y-graft diameter to safely accommodate a 14 Fr sheath (Figure 4). The presence of the Y-graft complicates contralateral safety access by rendering cross-over manoeuvres infeasible in case of vascular complications. Although alternative access routes such as apical, transaxillary, and transcaval approaches were discussed, these remain reserved for patients in whom transfemoral access is not feasible.^11^ To avoid cross-over manoeuvres, we used unilateral distal puncture (≥2 cm distal to the delivery sheath). Similar complex cases have been reported, with different management strategies. Soriano et al. presented a case series with TAVR followed by PCI without mechanical circulatory support,^12^ in contrast to our approach of Impella®-supported PCI prior to TAVR, which aimed to reduce ischaemic burden and avoid manipulating a freshly implanted valve with the Impella CP®. Naganuma et al. described transfemoral implantation of a balloon-expandable valve via surgical exposure of an aortofemoral graft.^13^ In contrast, we used a minimally invasive percutaneous graft puncture. To ensure vascular safety, ultrasound-guided puncture and pre-closure with ProGlide™ devices were performed. Our case also differed in valve type, use of circulatory support, and the complexity of complete revascularization. In summary, this case demonstrates the feasibility and safety of a staged approach with mechanical support, complete revascularization, and TAVR via complex access in high-risk patients.
(A) Multislice CT (three-dimensional reconstruction) shows the bilateral aortoiliac graft and the femoral arteries. (B) Sufficient luminal diameter of the (right) Y-graft.
Lead author biography
Dr Mohammad Yusuf Nejahsie graduated in 2018 from the Faculty of Medicine of the University of Hamburg, Germany. He is currently a Cardiology resident at the Department of Cardiology and Internal Intensive Care, Asklepios Klinik St. Georg in Hamburg-Germany. His main areas of interest are valvular and structural interventions.
Supplementary Material
ytag035_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pibarot P, Dumesnil JG. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J Am Coll Cardiol 2012;60:1845–1853.23062546 10.1016/j.jacc.2012.06.051 · doi ↗ · pubmed ↗
- 2Glazier JJ, Kaki A. The Impella device: historical background, clinical applications and future directions. Int J Angiol 2019;28:118–123.31384109 10.1055/s-0038-1676369 PMC 6679960 · doi ↗ · pubmed ↗
- 3Yeo I, Wong SC, Mack CA, Ko W, Kim LK, Feldman DN, et al Feasibility and safety of Impella-assisted high-risk CI before TAVR in patients with severe aortic stenosis. J Soc Cardiovasc Angiogr Interv 2023;2:101061.39132408 10.1016/j.jscai.2023.101061 PMC 11307818 · doi ↗ · pubmed ↗
- 4Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632.Erratum in: Eur Heart J. 2022 Jun 1;43(21):2022. doi: 10.1093/eurheartj/ehac 051.34453165 · doi ↗ · pubmed ↗
- 5Gul M, Akgul O, Erturk M, Eksik A, Yildirim A. Transcatheter aortic valve implantation through a left aortoiliac graft. Tex Heart Inst J 2012;39:898–900.23304050 PMC 3528219 · pubmed ↗
- 6Carlsson AC, Bandstein N, Roos A, Hammarsten O, Holzmann MJ . High sensitivity cardiac troponin T levels in the emergency department in patients with chest pain but no myocardial infarction. Int J Cardiol 2017;228:253–259.27865194 10.1016/j.ijcard.2016.11.087 · doi ↗ · pubmed ↗
- 7Junge W, Wilke B, Halabi A, Klein G . Determination of reference intervals for serum creatinine, creatinine excretion and creatinine clearance with an enzymatic and a modified Jaffé method. Clin Chim Acta 2004;344:137–148.15149882 10.1016/j.cccn.2004.02.007 · doi ↗ · pubmed ↗
- 8Clavel MA, Magne J, Pibarot P. Low-gradient aortic stenosis. Eur Heart J 2016;37:2645–2657.27190103 10.1093/eurheartj/ehw 096PMC 5030681 · doi ↗ · pubmed ↗