Pneumoperitoneum without significant bowel perforation in patients with blunt trauma: a systematic review and meta-analysis
Emad Masuadi, Yasir Ahmed Mohammed Elhadi, Osman S. Abdelhamed, Zainab M. Alkharas, Linda Östlundh, Gamila Ahmed, Ashraf F. Hefny

TL;DR
This study finds that about half of trauma patients with CT-detected free intraperitoneal air do not have significant bowel perforation, suggesting that not all cases require surgery.
Contribution
The study quantifies the proportion of blunt trauma patients with CT-detected free intraperitoneal air who do not have significant bowel perforation, challenging traditional surgical guidelines.
Findings
Approximately 51% of patients with CT-detected free intraperitoneal air had no significant bowel perforation.
The pooled analysis showed that 34% of free intraperitoneal air cases did not require surgery.
Benign pneumoperitoneum was often associated with high-energy trauma and managed nonoperatively in some cases.
Abstract
Free intraperitoneal air (FIA) after blunt trauma is traditionally considered a radiological marker of hollow viscus perforation requiring urgent laparotomy. However, emerging reports have described pneumoperitoneum without surgically meaningful bowel injury, raising concerns about unnecessary operations. This systematic review and meta-analysis aimed to quantify the proportion of patients with blunt trauma with computed tomography (CT)-detected FIA who had no significant bowel perforation, defined as either (1) non-therapeutic laparotomy with no identified macroscopic perforation or (2) successful nonoperative management without subsequent clinical deterioration. This review followed the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and was prospectively registered in the International Prospective Register of Systematic Reviews (CRD42020202174).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
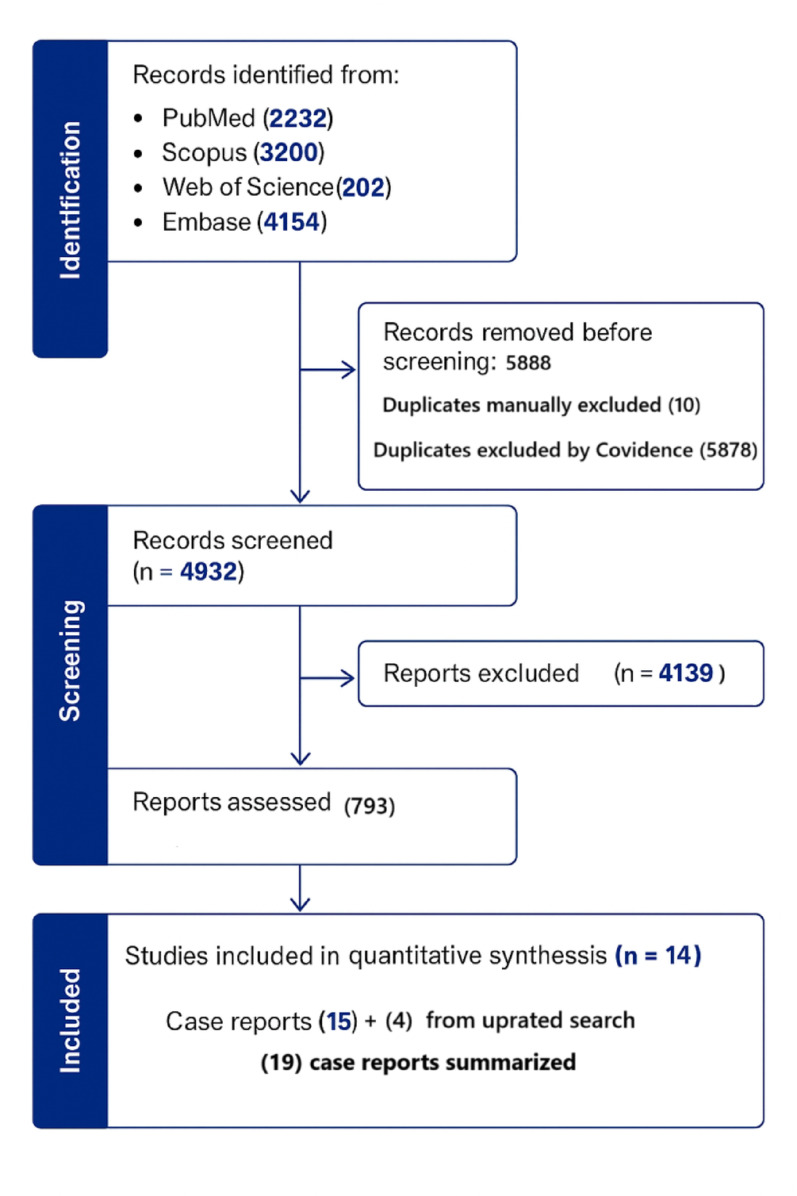 Figure 1
Figure 1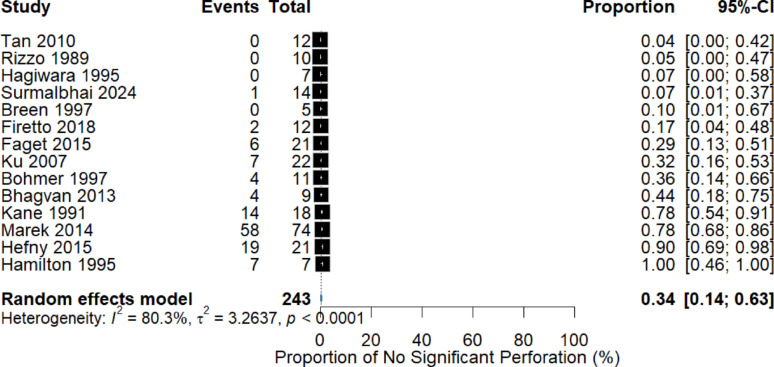 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal Trauma and Injuries · Appendicitis Diagnosis and Management · Abdominal Surgery and Complications
Background
Free intraperitoneal air (FIA) following blunt trauma is traditionally regarded as a critical radiological finding that raises immediate concerns regarding hollow viscus perforation and often prompts urgent laparotomy. Although bowel gas is normally confined to the gastrointestinal lumen, traumatic forces may allow air to escape into the peritoneal cavity. Prompt recognition of clinically significant bowel injuries is essential because delayed intervention is associated with increased morbidity and mortality [1]. However, FIA is not uniformly synonymous with surgically relevant perforations. Air may reach the peritoneal cavity through nonenteric pathways—including dissection of thoracic air, barotrauma related to mechanical ventilation, or gynecologic sources—or may arise from minor, self-limited bowel wall disruptions that do not require operative intervention [2, 3].
Computed tomography (CT) is the diagnostic modality of choice for evaluating blunt abdominal trauma. Several CT features, such as bowel wall thickening, mesenteric hematoma, and unexplained free fluid, are well-established predictors of bowel and mesenteric injuries [4, 5]. FIA, while an important warning sign, has demonstrated limited sensitivity and positive predictive value for diagnosing clinically significant perforation, with isolated pneumoperitoneum sometimes occurring in the absence of bowel injury [6, 7]. Small volumes of air, particularly when unaccompanied by other CT abnormalities, may therefore represent a benign entity rather than a marker of full-thickness perforation. Importantly, evidence from surgical series and case reports shows that some patients with blunt trauma with FIA do not have surgically demonstrable bowel perforation during laparotomy, whereas others remain clinically stable under nonoperative management [8]. While FIA warrants vigilance, treating all cases as perforations may expose patients to nontherapeutic laparotomy, which carries substantial morbidity, increased length of stay, and higher healthcare costs without improving survival [9].
Despite the growing recognition of benign traumatic pneumoperitoneum, the actual proportion of patients with blunt trauma with CT-detected FIA who do not have clinically significant bowel perforations remains unclear. Existing evidence is fragmented across heterogeneous observational studies and isolated case reports, and terminology varies widely, leading to inconsistencies in reporting and interpretation. To our knowledge, no previous systematic review has synthesized this evidence, quantified the pooled proportion of FIA cases without significant perforation, or summarized the potential benign mechanisms underlying FIA in blunt trauma. Therefore, this study aimed to systematically identify and synthesize all available data to (1) estimate the pooled proportion of patients with blunt trauma with CT-confirmed FIA who had no significant bowel perforation, defined as either negative laparotomy findings or successful nonoperative management without clinical deterioration, and (2) narratively summarize the reported benign mechanisms of traumatic pneumoperitoneum.
Materials and methods
Study design and literature search
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines [10] and prospectively registered in International Prospective Register of Systematic Reviews (CRD42020202174) [11]. A comprehensive search of PubMed, Embase, Scopus, and Web of Science was first performed from database inception to November 13, 2024, and subsequently updated during manuscript revision to include all studies published through November 2025, owing to the rarity of traumatic FIA. Search strategies combined Medical Subject Headings and keywords related to blunt trauma, bowel perforation, and FIA, with English-language restrictions applied. The full search strategies are provided in the Supplementary Material. The reference lists of included articles were screened to identify additional eligible studies.
Eligibility criteria
We included peer-reviewed observational studies (prospective or retrospective) reporting the outcomes of adult patients with blunt trauma with CT-detected FIA, in which patients were managed operatively or nonoperatively and the final bowel injury status could be determined. Studies were excluded if they met any of the following criteria:
- Included penetrating trauma, pediatric populations, or nontraumatic pneumoperitoneum.
- Lacked CT confirmation of FIA.
- Did not report whether bowel perforation was confirmed or excluded.
- Were review articles, commentaries, or conference abstracts.
Case reports and small case series were excluded from the meta-analysis but were synthesized narratively because of their relevance in describing benign traumatic pneumoperitoneum.
Screening and study selection
The search results were imported into Covidence (Veritas Health Innovation, Melbourne, Australia) for automated and manual duplicate removal. Two reviewers (YAME and OS), who were blinded to each other’s decisions, screened titles and abstracts according to the predefined eligibility criteria. The full texts of potentially eligible studies were independently assessed. Discrepancies were resolved by discussion or consultation with a third reviewer (AFH).
Data extraction and risk of bias assessment
Two reviewers (YAME and OS) independently extracted data using a standardized extraction sheet. Extracted variables included study design, sample size, mechanisms of injury, number of FIA cases, operative findings, nonoperative outcomes, and presence of bowel perforation. Any disagreements were resolved by consensus.
The risk of bias for observational studies was assessed independently by two reviewers using the Newcastle–Ottawa Scale [12]. Total scores ranged from five to seven of nine, indicating moderate methodological quality. Most studies demonstrated adequate case ascertainment and outcome verification, although comparability scores were consistently low because of limited adjustment for confounders. Full quality assessment results are provided in the Supplementary Material.
Operational definition
Given the variable terminology across studies, we adopted a standardized definition of no significant bowel perforation to ensure consistency. This category included:
- Nontherapeutic laparotomy, defined as the absence of a macroscopic full-thickness perforation despite CT-detected FIA. This definition acknowledges that minor or microscopic injuries may not be visible but are not surgically consequential.
- Successful nonoperative management, defined as hemodynamic and clinical stability during observation, with follow-up clinical assessment and/or imaging showing no deterioration, no delayed perforation, and no need for operative intervention.
This definition aligns with prior trauma literature. Hefny et al. [4] classified conservatively managed FIA as false-positive for perforation, whereas Marek et al. [5] categorized both negative laparotomy and stable nonoperative management outcomes as “benign free air.”
Synthesis and analysis
The primary outcome was the pooled proportion of patients with blunt trauma with CT-detected FIA who had no significant bowel perforation using the operational definition above. A meta-analysis of proportions was performed using a random-effects generalized linear mixed model with a logit link. This approach provides robust estimation of sparse and heterogeneous data and avoids biases associated with traditional transformation methods. Studies reporting zero events were retained using a minimal continuity correction (0.5 added to zero-event studies), consistent with Cochrane guidelines for rare-event meta-analyses. Heterogeneity was quantified using τ^2^ and I-squared statistic (measure of heterogeneity) (I^2^). Potential small-study effects were explored using contour-enhanced funnel plots and Egger regression tests. Case reports were not included in the meta-analysis but were summarized narratively to provide qualitative insight into benign mechanisms of pneumoperitoneum and patterns of conservative versus operative management.
Results
The initial search identified 10,820 studies across the four databases. After removing 5,888 duplicates (5,878 via Covidence and 10 manually), 4,932 studies remained. Of these, 4,139 were excluded based on titles and abstracts, leaving 793 studies for full-text review. Further assessment excluded 779 studies, comprising 15 case reports and 764 irrelevant studies. The updated search yielded no additional original studies; however, four newly published case reports meeting the inclusion criteria were identified. Finally, 14 studies met the inclusion criteria and were included in the quantitative synthesis (Fig. 1).Fig. 1. Preferred reporting items for systematic reviews and meta-analyses flow diagram of included studies
Summary of included studies
Table 1 presents the characteristics of the 14 studies included in the meta-analysis. Most studies were retrospective in design, with only two studies (Ku et al. [13] and Surmalbhai et al. [14]) conducted prospectively. Most cases of blunt trauma resulted from road traffic collisions or falls from heights. The number of patients with CT-confirmed FIA varied widely across studies, ranging from as few as four (Breen et al. [7]) to as many as 76 (Bhagvan et al. [15]). Several studies reported that a high proportion of patients underwent laparotomy; however, the proportion of patients with FIA who had no significant bowel perforation varied considerably. Studies, such as Breen et al. [7], Rizzo et al. [16], Tan et al. [17], and Hagiwara et al. [18], did not report any cases of FIA without significant perforation during laparotomy. Conversely, Hamilton et al. [19], Marek et al. [5], and Hefny et al. [4] documented a substantial proportion of patients with FIA without significant bowel perforation.Table 1. Summary of included studies and patients’ findings (N = 14 studies, 8,972 patients)StudyStudy designN trauma patients with CT scanN CT scan confirmed FIAN FIA and perforation at laparotomyN FIA without detectable perforation at laparotomySuccessful nonoperative managementN FIA and no perforation at laparotomy or successful nonoperative managementN without FIA on CT scan and perforation at laparotomyBohmer and Cowan [20]Retrospective1161171342Breen et al. [7]Retrospective31440005Firetto et al. [21]Retrospective8311210022Rizzo et al. [16]Retrospective51990001Tan et al. [17]Retrospective4111110005Marek et al. [5]Retrospective58777416243458Hagiwara et al. [18]Retrospective430660007Ku et al. [13]Prospective39422157079Bhagvan et al. [15]Retrospective78954048Hamilton et al. [19]Retrospective118702570Kane et al. [22]Retrospective18421214Hefny et al. [4]Retrospective419212019192Faget et al. [23]Retrospective556211560612Surmalbhai et al. [14]Prospective3014131015Total8972239117477512256CT, computed tomography; FIA, free intraperitoneal air
Across all studies, 239 patients (2.7%) had CT-confirmed FIA. Among these patients, 117 (49.0%) had confirmed bowel perforation during laparotomy, whereas 122 (51.0%) had no significant perforation, defined as negative laparotomy (n = 47) or successful nonoperative management without subsequent deterioration (n = 75). By comparison, among patients without FIA on CT, 56 of 8,733 (0.6%) were found to have bowel perforation at surgery. Using a random-effects meta-analysis with maximum likelihood estimation and Hartung–Knapp adjustment, the pooled proportion of patients with FIA who had no significant perforation was 34% (95% CI: 14%–63%) (Fig. 2). Substantial between-study heterogeneity was observed (I^2^ = 80.3%, τ^2^ = 3.2637, p < 0.0001), reflecting methodological and clinical variation across cohorts. Funnel plot inspection revealed an asymmetric distribution, suggesting potential small-study effects (Supplementary Material).Fig. 2. Forest plot showing the pooled proportion of patients with blunt trauma with computed tomography-detected free intraperitoneal air who had no significant bowel perforation, defined as either negative laparotomy or successful nonoperative management
Narrative synthesis of case reports
In addition to the quantitative synthesis, we identified 19 published case reports describing 20 patients with FIA following blunt trauma who had no significant bowel perforation according to our operational definition. These cases provide additional clinical context regarding the spectrum of benign pneumoperitoneum in trauma and highlight important variations in diagnostic pathways and management decisions. Most patients were men (84%) and young to middle-aged, with mechanisms of injury dominated by road traffic collisions, although several cases resulted from falls from heights or assault. Associated thoracic findings, such as pneumothorax or pneumomediastinum, were reported in multiple cases, supporting the hypothesis that extra-abdominal air can dissect into the peritoneal cavity without bowel disruption.
Laparotomy was performed in 15 of 20 patients, most of whom demonstrated no intraoperative evidence of bowel perforation, whereas five patients were successfully managed nonoperatively with clinical observation and, when reported, follow-up imaging demonstrating stability. A detailed summary of individual case characteristics, including patient demographics, mechanism of injury, associated thoracic air, diagnostic pathways, operative versus nonoperative management, and final outcomes, is presented in Table 2.Table 2. Summary of case reports of benign free air in patients with blunt traumaStudyAge/SexBlunt trauma mechanismCasesStudy typeAssociated Px or PmLaparotomyNonoperative managementGardner-T and Maddox [24]34/MRTC1Case report110Nishina et al. [25]60/MFall from height1Case report101Mussack et al. [26]47/MFall from height1Letter to editor110Assenza et al. [27]21/MRTC1Case report110Di Saverio et al. [28]21/M & 20/MAssault and TRC2Case report211Hakim et al. [29]45/MRTC1Case report110Webman et al. [30]56/MRTC1Case report110Curfman et al. [31]82/MFall of stairs1Case report110Carzolio et al. [32]21/MRTC1Case report101Lebby et al. [33]37/MRTC1Case report010Castro et al. [34]78/MRTC1Case report110Ubukata et al. [35]95/MRTC1Case report010Parvez et al. [36]27/MRTC1Case report010Kang and Choi [37]45/FRTC1Case report010Goyal et al. [38]22/MRTC1Case report110Lu et al. [39]16/FFall from height1Case report010Haddar et al. [40]46/MFall from height1Case report001Karoui et al. [41]60/MRTC1Case report010Rai et al. [42]56/MRTC1Case report010Associated Px or Pm**:** associated pneumothorax or pneumomediastinum; RTC: road traffic collision
Discussion
The findings of this systematic review and meta-analysis indicate that an identifiable subgroup of patients with blunt trauma with CT-detected FIA does not have clinically significant bowel perforation. This challenges the long-standing assumption that intraperitoneal air invariably requires surgical exploration. The pooled estimate of 34% (95% CI: 14%–63%) demonstrates considerable uncertainty but confirms that isolated FIA is not uniformly indicative of a hollow viscus injury requiring surgery. The wide confidence intervals and high heterogeneity underscore that these results must be interpreted with caution.
The substantial heterogeneity observed (I^2^ = 80.3%, τ^2^ = 3.26) likely reflects genuine clinical variation across studies, including differences in CT protocols, injury mechanisms, criteria for selecting patients for laparotomy, and definitions of clinically significant perforation. Importantly, modern multidetector CT scanners are highly sensitive for detecting even very small volumes of intraperitoneal air, including air of nonenteric origin. This increased sensitivity, while valuable for injury detection, may also lead to false-positive interpretations for bowel injury, thereby increasing the risk of nontherapeutic laparotomy.
Earlier studies, particularly those conducted before modern CT technology became widespread, frequently regarded FIA as pathognomonic for bowel perforation and therefore recommended mandatory exploratory laparotomy. Marek et al. identified a relatively high proportion of benign or clinically insignificant free air and advocated selective operative decision-making [5]. These more contemporary findings align with our pooled estimate and support selective nonoperative approaches in carefully evaluated patients.
Several nonenteric mechanisms may explain benign FIA in patients with blunt trauma. These include air tracking from pneumothorax or pneumomediastinum via the Macklin effect [43], barotrauma from positive-pressure ventilation, transiently sealed microscopic perforations, pseudopneumoperitoneum, and, more rarely, gynecologic sources. Therefore, FIA alone on CT may be an unreliable indicator of clinically significant bowel injury. However, adjunctive CT findings, such as unexplained free fluid, bowel wall discontinuity, mesenteric hematoma or stranding, or extraluminal contrast, substantially increase diagnostic confidence for clinically significant perforation [44]. Additionally, the number, size, and distribution of air pockets may help clinically differentiate pathologic perforation-related air from benign air patterns [4].
A narrative synthesis of 19 published case reports (20 patients) further reinforces these findings. Most patients were young men who sustained high-energy blunt trauma commonly associated with thoracic injuries, and none had a surgically meaningful bowel perforation. Among these patients, 15 underwent laparotomy with negative findings, whereas five were successfully managed nonoperatively. These reports highlight the risk of unnecessary surgery when FIA is considered in isolation and support a more selective, clinically integrated management strategy. Our analysis also showed that 0.6% of patients had bowel perforation despite no FIA on CT, consistent with the findings of prior literature demonstrating that CT sensitivity, although high, is not absolute. For patients with equivocal or nonspecific CT findings but high clinical suspicion, selective nonoperative management involving close observation, serial abdominal examinations, and, when indicated, repeat imaging remains a safe and evidence-based approach [8, 45]. Large trauma registry studies have further shown that nontherapeutic laparotomies are associated with increased morbidity and postoperative complications [8], reinforcing the need for careful patient selection.
Overall, the present findings support a structured, selective diagnostic algorithm that integrates clinical assessment with radiologic features rather than relying solely on the presence of FIA [5]. Surgical intervention should be reserved for patients with corroborative CT findings, clinical signs of peritonitis, or hemodynamic instability. Further research is needed to develop standardized CT-based scoring systems, define optimal monitoring protocols, and quantify the cost–benefit impact of reducing nontherapeutic laparotomies.
Limitations
This study had several limitations. First, verification bias is inherent, as not all patients with FIA underwent laparotomy. In some cases, “no significant perforation” was inferred from stable nonoperative management, which may underestimate the presence of macroscopic bowel perforation. Definitions of FIA, perforation, and required duration of observation varied across studies, introducing heterogeneity despite the use of a standardized operational definition. The predominance of retrospective, single-center studies further limits control over confounding factors and reduces the comparability of management thresholds. Additionally, FIA is a rare finding, accounting for 2.7% of CT-imaged trauma patients, resulting in small event counts and wide confidence intervals. Assessment of publication bias is also constrained, as funnel plots and related tests are not well calibrated for rare-event proportion meta-analyses. In addition, although the narrative synthesis of case reports provides practical clinical context, such reports are inherently subject to substantial publication bias, including selective reporting of atypical or benign presentations. This limitation may inadvertently over-weight anecdotal benign cases and restrict the generalizability of findings derived from case-level evidence.
Conclusions
A noteworthy subgroup of patients with blunt trauma with CT-detected FIA did not show clinically significant bowel perforation. Although FIA remains an important radiologic warning sign, it is not an independent diagnostic indicator of significant hollow viscus injury. Decision-making should integrate clinical assessment with adjunctive CT findings rather than rely on FIA alone. Owing to the rarity of FIA and limited sample sizes, larger prospective studies are required to refine the diagnostic performance of FIA and optimize selective nonoperative management strategies.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Radhiana H, Azian AA, Siti Kamariah CM. Computed tomography (CT) of bowel and mesenteric injury in blunt abdominal trauma: a pictorial essay.23082464 · pubmed ↗
- 2Hefny ashraf, Ostlundh L, Alkharas Z. Registered Protocol: Free intraperitoneal air without bowel perforation in blunt trauma patients: Systematic review. PROSPERO. https://www.crd.york.ac.uk/PROSPERO/view/CRD 42020202174. Accessed 9 Oct 2025
- 3Stang A. Critical evaluationof the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol; 2010;25:603–5.10.1007/s 10654-010-9491-z 20652370 · doi ↗ · pubmed ↗
- 4Howes N, Walker T, … NA-SA journal, 2012 undefined. Laparotomy for blunt abdominal trauma in a civilian trauma service. scielo.org.za N Howes, T Walker, NL Allorto, GV Oosthuizen, DL Clarke South African J surgery, 2012 scielo.org.za. https://www.scielo.org.za/scielo.php?pid=S 0038-23612012000200002&script=sci_arttext. Accessed 9 Oct 202522622098 · pubmed ↗