Improving diagnosis and management of pediatric ovarian masses: development of a risk stratification model incorporating sonographic and clinical features
Likai Chu, Zhiming Chen, Mingzhi Zhang, Tianna Cai, Min Zhang, Shuangquan Lu

TL;DR
This study creates a model to distinguish between benign and malignant ovarian masses in Chinese children using ultrasound and clinical features to avoid unnecessary surgeries.
Contribution
A pediatric-specific prediction model for ovarian mass malignancy using sonographic and clinical features in Chinese children.
Findings
A combined model of mass size and solid component proportion achieved high diagnostic accuracy (AUC = 0.93) for predicting malignancy.
Solid component proportion > 80% was the strongest predictor of malignancy (OR = 576.5).
Sonographic features like septations and calcifications help differentiate benign follicular cysts from epithelial tumors.
Abstract
To develop and validate a pediatric-specific prediction model for discriminating malignant from benign ovarian masses in Chinese children, aiming to reduce unnecessary surgeries for physiological follicular cysts. This single-center retrospective study analyzed 344 consecutive patients ≤ 18 years undergoing ovarian surgery (2018–2024). Three blinded radiologists assessed sonographic parameters: maximum mass diameter and solid component proportion (Categorized as < 20%, 20–40%, 40–60%, 60–80%, > 80%). Multivariate logistic regression integrated clinical features, tumor markers, and sonographic variables to construct a malignancy prediction model. Diagnostic performance was evaluated by receiver operating characteristic (ROC) analysis. Germ cell tumors (GCTs) predominated (72.7%, 253/348), with malignant lesions comprising 11.5% (40/348). Solid component proportion > 80% was the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
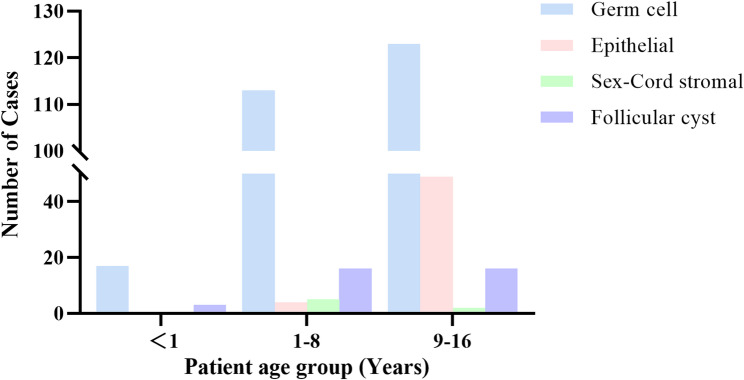 Figure 1
Figure 1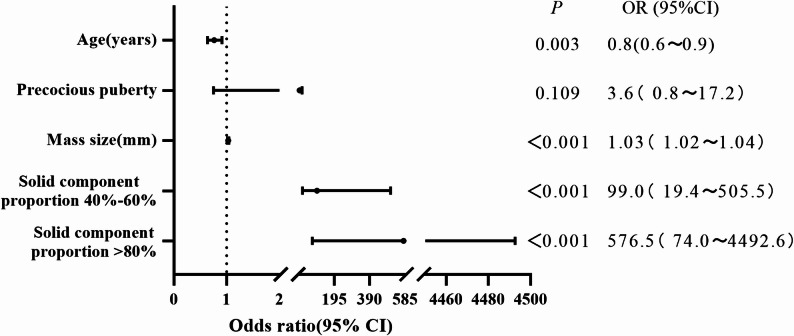 Figure 2
Figure 2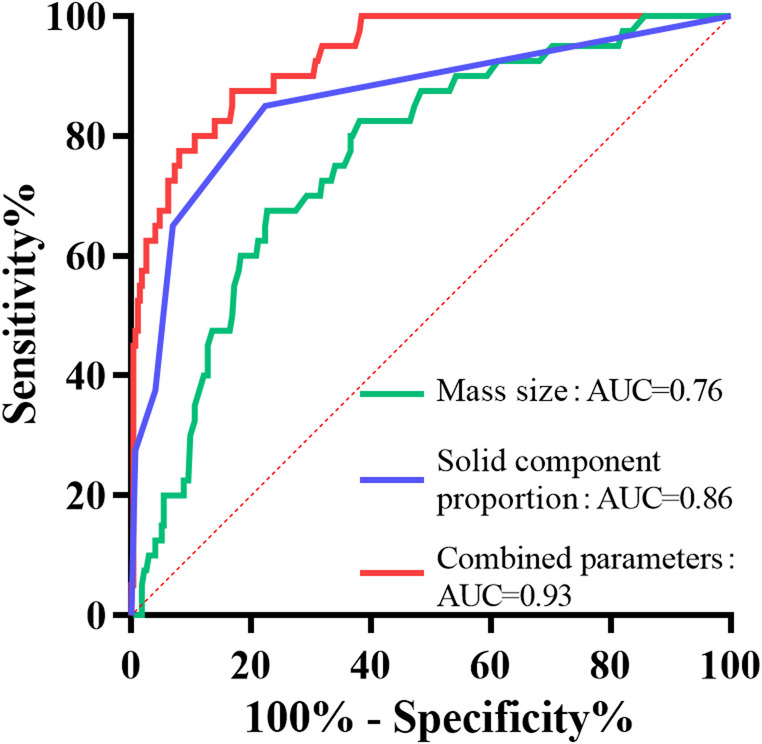 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian cancer diagnosis and treatment · Testicular diseases and treatments · Neuroblastoma Research and Treatments
Introducton
Ovarian masses represent the most prevalent gynecological neoplasms in children and adolescents, accounting for 1–2% of all pediatric malignancies. Strikingly distinct from adults—where epithelial carcinomas predominate—pediatric cases are dominated by GCTs (60–70%), predominantly benign mature teratomas, creating critical opportunities for fertility-preserving management [1, 2].
Early diagnosis of pediatric ovarian malignancies is well-established to significantly improve prognosis, even for advanced-stage tumors [3, 4]. However, progress is hindered by several persistent clinical dilemmas. First, adult prediction tools (e.g., The risk of ovarian malignancy algorithm [ROMA], Assessment of different neoplasias in the adneXa [ADNEX] models) are of limited use in children due to a fundamental mismatch: they target epithelial carcinomas and rely on CA-125 and HE4, whereas pediatric practice is dominated by GCTs, for which AFP and β-HCG are critical biomarkers [5, 6]. Moreover, although pediatric-specific risk models exist, they often rely on dichotomous imaging descriptors (e.g., solid vs. cystic) [7, 8]. However, since benign teratomas frequently contain solid elements like fat or bone [9], this simplistic dichotomization is inherently inaccurate for discriminating malignancy. Second, sonographic similarities between functional follicular cysts and surgically relevant epithelial tumors lead to unnecessary resections of physiological cysts, causing irreversible fertility damage. This clinical dilemma is under-represented in existing pediatric prediction models, which primarily focus on malignancy risk rather than also discriminating between types of benign lesions requiring different management. Third, current studies remain limited by small samples, while large-scale histopathological data from various populations remain scarce despite the potential for ethnic variations in tumor distribution. These gaps perpetuate reliance on subjective clinical judgment, leading to inconsistent surgical decision-making [10, 11].
To address these limitations, we conducted this large, single-center retrospective study of Chinese pediatric patients. The primary aims were: ① Systematically characterize the age-stratified pathological landscape of Chinese pediatric ovarian masses; ② To develop and validate a malignancy prediction model that integrates quantified sonographic parameters—specifically, the maximum diameter and a five-tiered categorical assessment of solid component proportion—with relevant clinical features and pediatric-appropriate tumor markers (AFP, β-HCG); ③ Establish objective clinical features and imaging discriminators for follicular cysts versus epithelial tumors.
This study introduces several key innovations to the field of pediatric ovarian mass management. First, we developed a novel, pediatric-specific predictive model that builds upon and refines existing tools [7]. Unlike adult-centric models or prior pediatric studies that often rely on dichotomous imaging descriptors, our model integrates pediatric-relevant tumor biomarkers (AFP, β-HCG) with quantitatively assessed sonographic parameters, most notably utilizing the solid component proportion as a graded categorical variable. Second, we established explicit and objective discriminators—specifically, the presence of septations or calcifications, alongside patient age and mass size—to differentiate physiological follicular cysts from neoplastic epithelial tumors, a common diagnostic pitfall leading to unnecessary surgery. By incorporating this novel, quantified imaging approach and directly addressing the follicular cyst dilemma, our model provides a significant advance over existing risk stratification tools. It is designed to optimize preoperative decision-making, with the dual goal of preserving fertility in low-risk children by avoiding unwarranted surgery while ensuring timely intervention for high-risk malignancies.
Methods
Participants
This single-center retrospective cohort study was approved by the Ethics Committee of Children’s Hospital of Soochow University (No. 2025CS184), with waiver of informed consent for anonymized retrospective data analysis. We included all consecutive patients ≤ 18 years who underwent ovarian surgery between January 2018 and December 2024. Exclusion criteria: ① Non-ovarian masses (e.g., Metastatic tumors to ovary); ② History of ovarian malignancy; ③ Incomplete clinical-sonographic data; ④ Disorders of sexual development. Finally, 344 patients were enrolled.
Data collection
In this study, we collected various demographic, clinical, and imaging data of pediatric patients with ovarian masses, including age; clinical presentation such as abdominal pain and precocious puberty; laterality of the mass; and tumor markers including AFP, CA125, β-HCG, Carcinoembryonic Antigen(CEA) and estradiol. Sonographic parameters were systematically assessed, including maximum mass diameter and solid component proportion (categorized as < 20%, 20–40%, 40–60%, 60–80%, and > 80%), as well as the presence of septations and calcifications. Additionally, histopathological results were recorded for all surgically resected masses.
Three blinded pediatric radiologists (> 10 years’ experience) assessed maximum diameter (mm) and solid component proportion (5-tiered: < 20%, 20–40%, 40–60%, 60–80%, > 80%). Septations were defined as internal linear echoes ≥ 1 mm; calcifications as hyperechoic foci with acoustic shadowing.
Statistical analysis
Normality of continuous variables was assessed by Shapiro-Wilk test. Normally distributed data are presented as mean ± SD (Independent t-test), non-normal as median Interquartile range [IQR] (Mann-Whitney U test). Categorical variables as frequency (%) (χ² or Fisher’s exact test). Binary logistic regression identified malignancy predictors with variable entry criterion: univariate p < 0.05. ROC analysis evaluated diagnostic performance. Analyses used SPSS 26.0 and Graphpad Prism 9.
Results
Among 348 ovarian masses from 344 pediatric patients undergoing surgery (Including 4 patients with bilateral masses) (Table 1), GCTs constituted the predominant pathology (253 cases, 72.7%), followed by epithelial tumors (53 cases, 15.2%), sex cord-stromal tumors (7 cases, 2.0%), and follicular cysts (35 cases, 10.1%). Mature teratoma was the most common subtype (219/253, 86.6%), with immature teratoma (22/253, 8.7%), yolk sac tumor (4/253, 1.6%), dysgerminoma (4/253, 1.6%), and mixed germ cell tumors (4/253, 1.6%) comprising the remainder. Serous cystadenoma (28/53, 52.8%) and mucinous cystadenoma (25/53, 47.2%) were observed in Epithelial tumors. Sex cord-stromal tumors are included juvenile granulosa cell tumor (4/7, 57.1%), Sertoli-Leydig cell tumor (2/7, 28.6%), and fibroma (1/7, 14.3%). Age distribution analysis (Fig. 1) revealed epithelial tumors predominantly occurred in the 9-16-year age group (49/53, 92.5%), whereas GCTs and follicular cysts showed no significant age-specific predominance across groups.
Table 1. Histopathological classification of 348 pediatric ovarian masses by cell type and age groupHistological diagnosis of tumor<1(y)1–8(y)9–16(y)TotalProportion ^a^Germ cell 17
113
123
253
72.7% Mature teratoma1693110 Immature teratoma1147 Yolk sac013 Dysgerminoma031 Mixed germ cell tumors022Epithelial 0
4
49
53
15.2% Serous cystadenoma0226 Mucinous cystadenoma0223Sex-cord stromal 0
5
2
7
2.0% Juvenile granulosa cell031 Sertoli-Leydig020 Fibroma001Follicular cyst31616 35
10.1% ^a^ Values are n (%) of 348 cases
Fig. 1. Distribution of ovarian mass pathologies across age groups (< 1, 1–8, 9–16 years)
After excluding follicular cysts (n = 35), 313 ovarian masses from 309 patients were classified by malignancy status, comprising 273 benign lesions (Including 4 bilateral cases) and 40 malignant lesions. Comparative analysis of clinical characteristics, laboratory markers, and ultrasound parameters is presented in Table 2. Malignant cases occurred at a significantly younger age than benign cases (7.4 ± 2.9 years vs. 8.8 ± 3.8 years; p = 0.01). No significant difference in laterality was observed (p = 0.07). Abdominal pain was the most common presenting symptom in both groups (Benign: 54.3%, Malignant: 52.5%; p = 0.834), while precocious puberty was significantly more frequent in malignant cases (20.0% vs. 8.6%; p = 0.025). Tumor marker analysis revealed significantly higher rates of elevated AFP, CA-125, and β-HCG in malignant tumors (All p < 0.001). CEA was undetectable in all tested cases, and no significant difference in estradiol levels was found between groups (p = 0.063). Ultrasound measurements demonstrated larger maximum diameters in malignant masses (105.4 ± 43.7 mm vs. 67.7 ± 45.5 mm; p < 0.001). Benign lesions predominantly exhibited < 20% solid component proportion (77.7%), whereas malignant lesions showed progressively higher solid component proportion (p < 0.001 for trend).
Table 2. Comparison of clinical characteristics, tumor markers, and ultrasound features between malignant and benign ovarian massesBenignMalignant P No. of Patients26940No. of Cases27340Age(years), mean ± SD8.8 ± 3.87.4 ± 2.90.01Laterality, Right-sided, n (%)Right: 151 (55.3%)Right: 16(40.0%)0.07Chief complaint, n (%) Pain146 (54.3%)21 (52.5%)0.834 Mass12 (4.5%)4 (10.0%)0.275 Precocious puberty23 (8.6%)8 (20.0%)0.025 Incidental finding88 (32.7%)7 (17.5%)0.052Tumor markers, n/N(%) ^a^ AFP1/124 (0.8%)19/23 (82.6%)<0.001 CEA0/124 (0%)0/23 (0%) CA−12512/102 (11.8%)14/18 (77.8%)<0.001 Estradiol8/43 (18.6%)6/11 (54.6%)0.063* β*-HCG0/85 (0%)6/15 (40.0%)<0.001Mass size by Ultrasound(mm), mean ± SD67.7 ± 45.5105.4 ± 43.7<0.001Solid component proportion (Ultrasound imaging), n (%) <20%212 (77.7%)6 (15.0%)<0.001 20%−40%42 (15.4%)8 (20.0%)0.457 40%−60%8 (2.9%)11 (27.5%)<0.001 60%−80%9 (3.3%)4 (10.0%)0.119 >80%2 (0.7%)11 (27.5%)<0.001Fisher’s exact test was used for groups with expected cell counts < 5Tumor marker elevation was defined as serum levels exceeding institutional reference ranges^a^ N indicates number of patients tested
Binary logistic regression analysis was performed using age(years), precocious puberty, mass size(mm), and solid component proportion (Categorized as 40–60% and > 80% with < 20% as reference, Fig. 2). The results identified age, mass size, solid component proportion 40–60% and > 80% as key predictors of malignancy. Age demonstrated an inverse association with malignancy (OR = 0.8, 95% CI: 0.6–0.9; p = 0.003). Increased mass size was significantly associated with a higher risk of malignancy (OR = 1.03 per mm, 95% CI: 1.02–1.04; p < 0.001). Both solid component proportion 40–60% (OR = 99.0, 95% CI: 19.4-505.5; p < 0.001) and > 80% (OR = 576.5, 95% CI: 74.0-4492.6; p < 0.001) were the strongest predictors of malignant ovarian masses. Although precocious puberty did not reach statistical significance (p = 0.109), it showed an increased risk of malignancy (OR = 3.6, 95% CI: 0.8–17.2).
Fig. 2. Forest plot of multivariate logistic regression analysis for predictors of malignancy
ROC curve analysis was performed to evaluate the diagnostic performance of ultrasound parameters-mass size, solid component proportion, and their combination-in differentiating malignant from benign ovarian masses (Fig. 3; Table 3). The solid component proportion demonstrated significantly higher diagnostic efficacy (AUC = 0.86; p < 0.001) compared to mass size alone (AUC = 0.76; p < 0.001). However, the combined model achieved excellent predictive power (AUC = 0.93; p < 0.001), substantially outperforming either single parameter.
Fig. 3ROC curves for malignancy prediction
Table 3. Diagnostic performance for differentiating malignant from benign pediatric ovarian masses using ROC curve analysisParameterAUC p Cut-off valueSensitivity(%)Specifici(%)Mass size0.76<0.00185.5 (mm)67.577.3Solid component0.86<0.001>30%85.077.7Combined model^a^0.93<0.0010.09787.583.2^a^ The combined model refers to the predicted probability derived from the multivariate logistic regression model including mass size and solid component proportion
To establish reliable discriminators for reducing unnecessary surgery, we analyzed 53 epithelial tumors and 35 follicular cysts (Table 4). Patients with epithelial tumors were significantly older than those with follicular cysts (median age: 12 years [IQR 10–13] vs. 8 years [IQR 1–12]; p < 0.001). Laterality analysis revealed a distinct distribution pattern, with follicular cysts exhibiting a predilection for the right ovary (74.3% vs. 52.8% in epithelial tumors; p = 0.043). Precocious puberty was more prevalent in the follicular cyst group (37.1% vs. 13.2%; p = 0.009). Ultrasound measurements revealed larger maximum diameters in epithelial tumors (78 mm [IQR 54–107] vs. 50 mm [IQR 44–59]; p < 0.001). While both types predominantly presented as purely cystic lesions (Epithelial: 66.0%, Follicular: 100%), septations (28.3% of epithelial cysts) and psammomatous calcifications (5.7%) were exclusively observed in epithelial tumors.
Table 4. Comparison of characteristics between epithelial tumors and follicular cysts in pediatric ovarian massesEpithelialFollicular cyst P No. of Patients5335No. of Cases5335Age(years), IQR12 (10,13)8 (1,12)<0.001Laterality, Right-sided, n (%)Right:28 (52.8%)Right:26 (74.3%)0.043Chief complaint, n (%) Pain28 (52.8%)13 (37.1%)0.149 Mass5 (9.4%)3 (8.6%)1.000 Precocious puberty7 (13.2%)13 (37.1%)0.009 Incidental finding13 (24.5%)6 (17.1%)0.410Mass size(mm), IQR78 (54,107)50 (44,59)<0.001Imaging characteristic(Ultrasound), n(%) Purely cystic35 (66.0%)35 (100%)<0.001 Presence with calcification3 (5.7)0 (0%)0.273 Presence with septations15 (28.3%)0 (0%)<0.001Abbreviation: IQR Interquartile rangeFisher’s exact test was used for groups with expected cell counts < 5
Discussion
This study establishes a malignancy prediction model for pediatric ovarian masses based on a large Chinese cohort (n = 344). Key discoveries include: ① GCTs dominate the pathological spectrum (72.7%), with mature teratoma comprising 86.6%; ② Solid component proportion > 80% emerged as the strongest malignancy predictor (OR = 576.5, p < 0.001); ③ The combined model (Mass size + Solid component proportion) significantly improved diagnostic accuracy (AUC = 0.932 vs. 0.86 for solid component proportion alone); ④ For follicular cyst discrimination, septations (28.3%) and calcifications (5.7%) were specific to epithelial tumors (p < 0.001). These findings address the critical evidence gap in Chinese pediatric ovarian oncology.
This study confirms that GCTs constituted the predominant pathological type of ovarian masses in Chinese children, accounting for 72.7% (253/348) of cases. Within GCTs, mature teratoma was the most prevalent subtype (86.6%, 219/253), aligning closely with epidemiological data from Western populations [12]. Epithelial tumors represented the second most common category (15.2%, 53/348). Notably, epithelial tumors demonstrated a striking age-dependent prevalence, with 92.5% (49/53) occurring in the 9-16-year age group. This pattern may be attributed to gonadal maturation and dynamic hormonal changes characteristic of this developmental stage [13, 14]. The overall malignancy rate in our surgical cohort was 11.5% (40/348). Among malignant lesions, GCTs were again predominant (85.0%, 34/40), with immature teratoma being the most frequent malignant subtype (55.0% of malignant GCTs, 22/40). This distribution underscores the fundamental pathological divergence between pediatric and adult ovarian masses, where epithelial carcinomas predominate [15]. However, pediatric-specific prediction models for ovarian malignancy are relatively scarce, and clinical focus remains primarily oriented towards adult malignancies [5]. Consequently, developing efficient, pediatric-specific prediction models for ovarian malignancy, such as the one validated herein, is of paramount clinical significance.
Although the initial clinical presentations of ovarian masses are diverse, abdominal pain represents the most common symptom in both benign and malignant cases. This is largely attributable to the frequent use of ultrasound as the primary screening modality for pediatric abdominal emergencies, leading to the incidental detection of many masses during abdominal scanning [16]. In our view, consequently, abdominal pain alone cannot serve as a reliable discriminator for tumor malignancy. However, precocious puberty demonstrates a statistically significant difference between benign and malignant tumors. This association is likely attributable to the hormone-secreting properties of specific malignancies, particularly sex cord-stromal tumors such as juvenile granulosa cell tumors [17].
Regarding tumor markers, although CA125 levels demonstrated a statistically significant difference between benign and malignant groups (p < 0.001), its sensitivity for malignancy was merely 53.8% (14/26). Our data demonstrated a weak correlation of CA125 with malignancy in children, consistent with prior criticisms of adult models like ROMA [5]. In the present study, we incorporated AFP and β-HCG, markers highly relevant to pediatric germ cell malignancies. AFP exhibited the highest sensitivity (95.0%, 19/20) for identifying malignant germ cell tumors. This exceptional performance stems from the persistent and excessive production and secretion of AFP by yolk sac tumor elements, a common component within malignant pediatric germ cell tumors [3]. Similarly, elevated β-HCG levels in children and adolescents (Excluding pregnancy) strongly suggest the presence of trophoblastic components, most frequently encountered in mixed germ cell tumors and immature teratomas [18]. By formally integrating AFP and β-HCG with key imaging parameters, our work translates established biomarker knowledge into a practical, multi-parameter risk assessment tool for the pediatric population [8, 10, 19]. Critically, postoperative monitoring reveals that declining AFP and β-HCG levels serve as favorable prognostic indicators, whereas elevated or rising levels may indicate tumor recurrence [20].
The most potent predictor in our model was a solid component proportion exceeding 80% (OR = 576.5). This finding extends beyond prior studies that often used a binary “presence of solid tissue” as a risk factor [21, 22]. By implementing a five-tiered grading system, we demonstrated a dramatic, quantifiable increase in malignancy risk with increasing solidity. Notably, we identified a solid component proportion > 40% as a critical, child-specific risk threshold, with the 40–60% category already conferring a high odds ratio (OR = 99.0). This stands in contrast to the ADNEX model, which uses a > 10% solid component threshold derived from adult epidemiology, a criterion that would likely overestimate malignancy risk in children due to the high prevalence of benign mature teratomas containing solid elements [23]. Our multiparameter model, combining this refined solid component metric with maximum tumor diameter, achieved excellent diagnostic accuracy (AUC = 0.932), which compares favorably with previously reported models in pediatric literature [7, 18].
Although epithelial tumors and follicular cysts share similar sonographic features, their clinical management differs substantially: epithelial tumors typically require surgical resection, whereas follicular cysts are functional entities that often resolve spontaneously [24]. Follicular cysts arise from immature hypothalamic-pituitary-gonadal (HPG) axis development in young children (< 8 years), rendering them susceptible to external stimuli (e.g., Obesity, Stress) that trigger excessive follicular proliferation without ovulation, ultimately leading to cyst formation [25]. In contrast, epithelial tumors originate from heightened proliferative activity of ovarian surface epithelium during gonadal maturation in adolescence, which increases cumulative genetic mutations [26]. Consequently, follicular cysts manifest at significantly younger ages than epithelial tumors. A statistical difference in laterality was observed (p = 0.043). However, we do not consider this to be clinically meaningful. The finding is likely a spurious association attributable to the small sample size in this subset of patients rather than a reflection of true underlying pathophysiology. Unlike epithelial tumors, follicular cysts feature granulosa cells that persistently secrete estradiol, resulting in prominent pseudoprecocious puberty [25]. Due to confinement by the ovarian cortex, follicular cysts undergo spontaneous rupture or absorption upon reaching critical dimensions, whereas epithelial tumors possess inherent proliferative capacity and sustained secretory function—enabling continuous growth unless detected due to acute complications like torsion or rupture [27–29]. Therefore, this fundamental difference in biological behavior explains why epithelial tumors are typically discovered at significantly larger sizes compared to follicular cysts. mucinous cystadenomas, the calcifications might be related to a secretory phenomenon, while true septations form through epithelial cell projections into the lumen supported by fibrovascular cores [30, 31]. Although the aforementioned features are established in the diagnosis of cystadenomas, these characteristics have not been formally incorporated into pediatric-specific risk models as key discriminators for excluding follicular cysts. The mechanistic framework elucidated herein—anchored in developmental endocrinology (HPG axis immaturity) and tumor biology (epithelial mutational accumulation)—validates our discriminative criteria (Age < 8 years, Precocious puberty, Absence of septations/calcifications), enabling a reduction in unnecessary surgeries for physiological cysts while ensuring timely intervention for true neoplasms.
Derived from multivariate analysis, our novel risk stratification framework incorporates an ultrasound-first classification protocol. Purely cystic masses (Type A): For purely cystic masses, discrimination between follicular cysts and neoplastic lesions must integrate age, size, precocious puberty manifestations, and the absence/presence of septations or calcifications—critical to avoid unnecessary resections of physiological entities. Solid-containing masses (Type B): ① Low-risk: Solid component proportion < 20% + Maximum diameter < 85.5 mm + Absence of elevated AFP, CA125, or β-HCG; ② Intermediate-risk: Solid component proportion 20–40% ± Maximum diameter ≥ 85.5 mm + Absence of elevated AFP, CA125, or β-HCG; ③ High-risk: Solid component proportion > 40% + Maximum diameter ≥ 85.5 mm ± Presence of elevated AFP, CA125, or β-HCG. This system synergistically integrates quantitative sonographic parameters (Solid component proportion, Mass size) and serum biomarkers (AFP, β-HCG, CA125), significantly enhancing diagnostic efficacy for pediatric malignancies and providing critical guidance for surgical decision-making.
Several limitations also warrant consideration. First, the potential diagnostic significance of the ovarian crescent sign was not systematically evaluated in our cohort [32]. Second, the absence of borderline epithelial tumors in our series (0/53 epithelial cases) contrasts with reported pediatric incidences of around 15% [22]. This is a notable limitation because borderline tumors may present as large, predominantly cystic masses with negative tumor markers—a profile that would be classified as low-risk by our model, suggesting possible selection bias or center-specific pathological classification practices. Most critically, the extraordinarily wide confidence intervals accompanying high odds ratios (e.g., OR = 576.5, 95% CI: 73.97-4,492.60 for solid proportion > 80%) reflect instability in risk estimation attributable to the limited number of malignant cases (n = 40). Nevertheless, these evidence-based advances address critical gaps and represent a step toward more accurate risk stratification of pediatric ovarian masses.
Conclusion
This study successfully developed and validated a pediatric-specific prediction model for sonographic malignant from benign ovarian masses in Chinese children, integrating sonographic features with clinical and laboratory data. Our findings underscore the predominance of GCTs in this population and establish solid component proportion > 40% as a quantitative imaging marker for malignancy risk stratification. The combined model, incorporating mass size and solid component proportion, demonstrated superior diagnostic accuracy (AUC = 0.932), significantly outperforming individual parameters. Furthermore, in addition to patient age and mass size, the identification of septations and calcifications as features exclusive to epithelial tumors provides a reliable means to differentiate them from physiological follicular cysts, thereby reducing unnecessary surgeries. This model, which provides a practical, evidence-based tool for preoperative decision-making, helps ensure timely intervention for high-risk cases while preserving ovarian function in low-risk patients. Its design is grounded in the distinct pathophysiology of pediatric ovarian masses.