Effects of aqueous aloe vera gel extract on acetaminophen-induced liver damage: a histomorphological, hematological and biochemical study in Albino rats
Yahye Ahmed Abdi, Bot Yakubu Sunday, Charles Idehen, Glory Mbe Nja, Yibala Ibor Oboma, Timothy Neeza, Mustfe Ahmed Awil, Hani Mohamed Mohamud, Maria Ali Mudei, Deko Omar Mohamed

TL;DR
Aloe vera gel extract can protect against liver damage caused by acetaminophen overdose in rats, showing effects similar to a known liver protectant.
Contribution
The study demonstrates the hepatoprotective efficacy of Aloe vera gel extract at a 1000 mg/kg dose comparable to silymarin.
Findings
Aloe vera extract at 1000 mg/kg improved liver function and reduced oxidative stress in acetaminophen-treated rats.
Higher doses of Aloe vera extract restored liver tissue structure and improved hematological parameters.
The extract showed antioxidant and anti-inflammatory effects comparable to silymarin.
Abstract
Acetaminophen overdose is a leading cause of drug-induced acute liver damage, underscoring the urgent need for accessible hepatoprotective therapies. This study evaluated the hepatoprotective effects of Aqueous Aloe vera gel extract on acetaminophen-induced liver damage in adult male Albino Wistar rats. Liver Damage was induced in Albino Wistar rats by oral administration of acetaminophen (750 mg/kg). The rats were divided into six groups: normal control, negative control, positive control (silymarin 50 mg/kg), and three treatment groups receiving Aloe vera gel extract at doses of 250 mg/kg, 500 mg/kg, and 1000 mg/kg. Body and liver weight, hematological, biochemical and oxidative stress parameters and liver histology were assessed after 7 days of treatment. Treatment with Aloe vera gel extract demonstrated dose-dependent hepatoprotective, anti-inflammatory and antioxidant effects…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
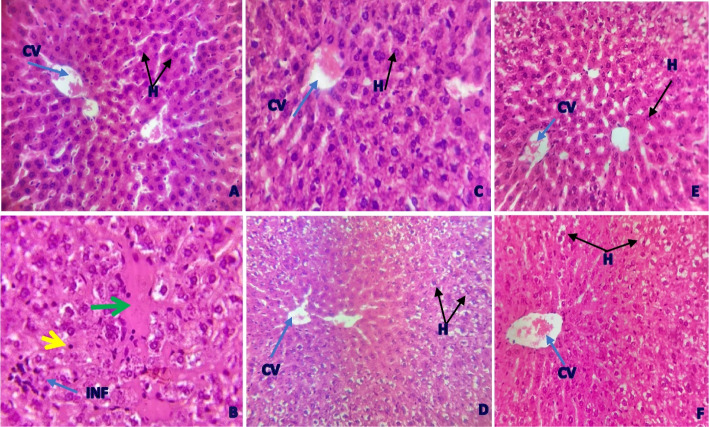 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Hepatotoxicity and Protection · Phytochemistry and biological activity of medicinal plants · Chemotherapy-induced organ toxicity mitigation
Introduction
Acetaminophen (APAP) is a common over-the-counter medication used to reduce fever and relieve pain associated with headaches, mild to moderate discomfort, and other conditions. While safe at recommended doses [1], excessive intake whether from a single overdose or chronic misuse can cause severe liver damage, leading to toxicity that has been fatal in both human cases and animal studies [2].
The hepatotoxicity of acetaminophen involves a complex mechanism. At normal doses, the liver metabolizes APAP mainly via glucuronidation and sulfation. A small fraction is processed by cytochrome P450 enzymes (especially CYP2E1), producing the toxic metabolite N-acetyl-p-benzoquinone imine (NAPQI). Under typical conditions, glutathione (GSH) neutralizes NAPQI. However, during an overdose, metabolic pathways become overwhelmed, increasing NAPQI production. This depletes GSH reserves, allowing NAPQI to damage cellular proteins, disrupt mitochondria, and induce oxidative stress, ultimately causing cell death [3].
The FDA sets a maximum daily dose of 4000 mg for adults, with toxicity typically occurring at 7.5–10 g/day or 140 mg/kg [4]. Acetaminophen overdose is a major public health issue, causing 56,000–80,000 emergency visits, 26,000–34,000 hospitalizations, and around 500 deaths annually in the U.S [5]. In Africa, it accounts for nearly 48% of acute liver failure cases, with a 28% mortality rate among transplant candidates in low- and middle-income countries [6].
The liver plays a crucial role in detoxification and maintaining biochemical balance. Liver injury, often linked to oxidative stress from free radicals, is a growing global concern due to rising hepatic disease mortality. Contributing factors include exposure to toxins, certain drugs, and pathogens. Current treatments such as medications, surgery, and transplants have limited efficacy and notable side effects [7].
Given these challenges, natural hepatoprotective agents like Aloe vera have gained attention. Traditionally used in African medicine, Aloe vera exhibits anti-inflammatory, antioxidant, and regenerative properties. Its bioactive compounds including anthraquinones, vitamins, and phytochemicals—may support liver health [8].
In Uganda, A. vera leaf decoctions treat malaria, stomach pain, fever, infections, and skin conditions [9]. Similarly, Indonesians apply its gel to burns and hair ailments [10]. Research highlights A. vera's broad pharmacological potential, including antibacterial, antidiabetic, and wound-healing effects [11].
Evidence for Aloe vera's Hepatoprotective Potential from In Vitro and Animal Studies: Pre-clinical research has provided substantial evidence supporting the potential hepatoprotective effects of Aloe vera against various liver insults, including acetaminophen-induced liver damage. These studies have elucidated several mechanisms by which Aloe vera exerts its beneficial effects. Oxidative stress is a critical component of acetaminophen-induced liver Damage. Aloe vera gel extract and its components have demonstrated potent antioxidant activities in vitro by scavenging free radicals, reducing lipid peroxidation, and enhancing endogenous antioxidant enzyme systems such as superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GSH-Px) [12, 13]. For instance, in vitro studies using HepG2 cells have shown that Aloe vera gel can reduce reactive oxygen species (ROS) production and exhibit radical scavenging activity [14, 15]. This direct and indirect antioxidant action is crucial in preventing cellular damage caused by NAPQI. Anti-inflammatory Effects: Inflammation plays a significant role in the progression of Acetamnophen hepatotoxicity. Aloe vera has been shown to possess anti-inflammatory properties by inhibiting the production of pro-inflammatory cytokines such as interleukin-1 beta (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), and tumor necrosis factor-alpha^1^ (TNF-α) [16, 17]. Studies on immortalized human keratinocytes (HaCaT cells) subjected to inflammatory stress have demonstrated that Aloe vera extract can inhibit IL-8 secretion, highlighting its anti-inflammatory potential [18]. Components like aloesin, aloin, and emodin within Aloe vera have been implicated in modulating immune responses and limiting excessive inflammation [19]. Acetaminophen overdose triggers hepatocyte apoptosis and necrosis. Some components of Aloe vera, such as aloe-emodin, have been shown to influence cell viability and apoptosis in liver cancer cell lines (in vitro HepG2 cells), suggesting a potential role in modulating cell death pathways in liver damage [20]. Replenishing GSH stores is a primary strategy for treating Acetaminophen liver damage. Animal studies have consistently shown that Aloe vera administration can significantly restore hepatic GSH levels depleted by acetaminophen overdose [21]. This is critical for the detoxification of NAPQI and the prevention of its deleterious effects. Histopathological Improvement in Animal Models: Numerous in vivo studies in rodents have provided compelling evidence of Aloe vera's hepatoprotective effects against Acetaminophen-induced liver damage [22]. A study in mice demonstrated that Aloe vera attenuated Acetaminophen-induced hepatitis by improving liver histopathology, reducing oxidative stress (decreased malondialdehyde, MDA), and restoring hepatic GSH levels. Similar protective effects, characterized by reduced liver enzyme levels (ALT, AST), decreased inflammatory markers, and improved liver architecture, have been observed in various animal models of chemically induced liver injury, including those induced by carbon tetrachloride.
This study is novel in its comprehensive evaluation of aqueous Aloe vera gel extract’s dose-dependent hepatoprotective effects against acetaminophen-induced liver damage in male Albino Wistar rats, integrating histomorphological, hematological, biochemical, and oxidative stress parameters to demonstrate efficacy comparable to silymarin.
Although studies suggest Aloe vera protects against liver damage, its specific impact on acetaminophen-induced damage particularly on liver histology, blood parameters, and biochemistry remains unclear. Further research is needed to explore its therapeutic, reparative, or preventive role in Acetaminophen-related hepatotoxicity.
Materials and methods
Study aim, design and setting
The study was an in vivo experiment to determine the histomorphological, hematological and biochemical effects of an aqueous Aloe vera gel extract on acetaminophen induced liver damage in Albino rats. The study was carried out at Kampala International University – Western Campus (KIU-WC) located in Bushenyi district, Southwestern Uganda. Plant extraction was done at the KIU-WC Pharmacognosy Laboratory, and in vivo studies were done at the KIU-WC Animal Research Laboratory. Blood and liver tissue for hematological, biochemical and histopathological analysis respectively was taken for processing immediately at KIU-Teaching Hospital. All the chemicals and reagents used in the study were of analytical grade and were purchased from authorized distributors.
Plant material collection, identification, and extract preparation
Mature fresh Aloe vera leaves were collected in January 2025 from private land within Bushenyi-Ishaka Municipality, in Bushenyi district, Western Uganda, with verbal permission from the landowner. The Aloe vera samples were collected from private property, and appropriate permission was obtained from the landowner prior to collection. No additional permits or licenses were required for collecting this non-protected plant species. The collected leaves were taxonomically identified by Dr. Eunice A. Olet at Mbarara University; the identified material was assigned the identification number YAA-2025–001.
The Aloe vera gel extract was prepared using a modified method adapted from Werawatganon et.al. [23]. Freshly collected mature Aloe vera leaves were washed clean, allowed to shade dry and sliced open to extract the gel. Aloe vera gel extraction was done by cold maceration where 1978 g of the gel was blended and soaked in an equal volume of distilled water (1978 mL). The mixture was then left to sit on a rotary shaker for 24 h, after which it was strained with cotton wool, was sieved with a double muslin cloth and filtered using Whatman filter paper No.1. The extract was then oven dried at 40 °C, weighed and kept in a properly labelled sample bottles and stored at −4 °C. The percentage yield of the dried extract was calculated based on the oven-dried weight of the initial plant material using the formula; percentage yield = [(weight of dry gel extract/weight of the fresh gel) × 100] and found to be 2.02%.
The aqueous Aloe vera gel extract was qualitatively screened for phytochemical constituents such as alkaloids, flavonoids, tannins, saponins, anthraquinones and amino acids using the methods described by Khan et al. [7].
Experimental animals, housing and feeding
Thirty adult Albino rats; 30—male and 6 – female at 8 weeks old, weighing between 150—180 g were used in the present study. The animals were obtained from the Animal House Facility of the Kampala International University, Western Campus. They were left to acclimatize for 14 days in the laboratory conditions before the experiment.
The animals were housed according to their dose groups in cages with softwood shavings as bedding, fed on standard pellet meal (Engaano Millers Limited, Kampala), given clean water ad libitum, and maintained under suitable laboratory conditions (temperature 22 °C ± 3 °C; relative humidity 60% ± 5% & half-day light–dark cycle). The research was conducted following the nationally and internationally acceptable animal use principles, safety, and handling.
Induction of liver injury and treatment
Liver injury was induced in twenty-five male Albino Wistar rats by administering them with a single oral dose of 750 mg/kg of acetaminophen following a study by Boyd and Hogan [24]. After 72 h, the rats were checked for an elevation (> 65 U/L) in the liver enzymes AST and ALT to confirm liver damage.
Prior to treatment, the median lethal dose (LD50) of the aqueous Aloe vera gel extract was evaluated using the Up and Down method described in OECD guideline 425 in 6 female rats and found to exceed 5000 mg/kg, indicative of low acute toxicity. The experimental animals were then randomly divided into six groups of five rats each that is; the normal control group, negative control group (distilled water 10 mg/kg), positive control group (silymarin 50 mg/kg), low (250 mg/kg), medium (500 mg/kg) and high (1000 mg/kg) dose of the aqueous Aloe vera gel extract. To identify the rats, a unique number was marked on the tail of each rat using a permanent marker. Except for group one, all the other groups contained acetaminophen-induced liver-damaged animals and were treated according to their respective groupings. Administration of both silymarin and Aloe vera gel extract was done once daily as an oral bolus by oral gavage after measurement of the rats’ body weight for 7 days. The body weights of each rat were measured at the start of the study, on day 3 and at the end of the study.
Collection of samples and measurement of study parameters
At the end of the experiment and after an overnight fast, all animals were humanely euthanized by placing them in an enclosed chamber containing cotton soaked with Halothane. This method aimed to deliver a concentration sufficient to induce rapid unconsciousness and respiratory arrest. For reference, Halothane is typically administered via vaporizer at concentrations up to 5–7% for euthanasia in small animals. Blood samples were collected through cardiac puncture from all of the rats while the liver was removed for histological analysis. The liver was examined for gross morphological changes and weighed before it was fixed in 10% neutral formaldehyde buffer for 5 days for histopathological studies.
Approximately 2 mL of the blood collected was placed into EDTA-containing tubes for hematological analysis using an automated hematology analyzer. Hematological evaluation included the following parameters: red blood cell (RBC) count, white blood cell (WBC) count, hematocrit (HCT), hemoglobin (HGB) concentration, differential white cell count, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), and platelet count. The other portion of the blood (3 mL) was put into non-heparinized vacutainers for biochemical analysis using an automated biochemistry analyzer, to determine the liver function tests such as serum concentrations of alanine transaminase, alkaline phosphatase, and aspartate transaminase.
The liver was removed, weighed, and examined for gross morphological changes. The excised livers from the rats were cleaned, and a portion was homogenized in 10% freshly prepared sodium phosphate-buffered saline for malondialdehyde (MDA), superoxide dismutase (SOD) and catalase (CAT) analysis. Additionally, another portion of the liver was fixed in 10% neutral formaldehyde buffer for 5 days pending histological processing. Sections of 5 µm thickness were cut, stained with hematoxylin and eosin (H&E), and mounted using synthetic resin. The prepared slides were then examined under a light microscope for histological evaluation and photomicrographs of selected slides were taken using a light microscope (Olympus BH2) mounted with a Nikon Digital Sight DS-L1 (Nikon Corporation, Japan).
Oxidative stress parameters (MDA, SOD and CAT) were determined as outlined by Khan et al. [7]. Liver tissue homogenates (10%) were centrifuged at 3,000 rpm for 10 min at 4 °C to obtain the supernatant for the determination of lipid peroxidation, CAT and SOD concentrations. Lipid peroxidation levels were analyzed using a commercial kit based on the formation of thiobarbituric acid reactive substances in conjugation with MDA. The activities of antioxidant enzymes (SOD and CAT) were determined using commercially available assay kits following the instructions provided by the manufacturer.
Data management and analysis
Data obtained from this study were statistically analyzed using Graph Pad Prism (Version 9.5.1). Statistical significance between groups was determined by one-way ANOVA followed by Turkey's Honest Post-hoc test. Results are presented as mean ± standard error of the mean (SEM), and values at p ≤ 0.05 were considered statistically significant.
Results
Phytochemical composition of the aqueous aloe vera gel extract
Qualitative phytochemical analysis confirmed the presence of tannins, flavonoids, saponins, anthraquinones, amino acids and alkaloids (Table 1).Table 1. Phytochemical profile of the aqueous Aloe Vera gel extractPhytochemicalTest usedQualitative Test ResultTanninsFerric chloride test + FlavonoidsShinoda test + SaponinsFoam test + AnthraquinonesBontrager’s test + Amino acidsNinhydrin test + AlkaloidsDragendorff’s test + + indicates presence
Effect of the aqueous Aloe vera gel extract on the body and liver weight following acetaminophen-induced liver Damage in male Albino Wistar rats
The study's findings showed no significant differences in the body weights of the animals at the start of the study after induction of liver Damage with acetaminophen. However, by the end of the study, animals that received 1000 mg\kg of the aqueous Aloe vera gel extract had a significantly Higher body weight (p = 0.0265) compared to those given 250 mg/kg (Table 5). Similarly, there was a marked increase in liver weight (p = 0.0061) in the group treated with 1000 mg/kg of the extract relative to the 250 mg/kg group (Table 2).Table 2. Effect of the aqueous Aloe vera gel extract on the body and liver weightStudy variablesTreatment groupsNormal controlNegative controlSilymarin 50 mg/kg250 mg/kg of Aloe vera500 mg/kg of Aloe vera1000 mg/kg of Aloe veraInitial body weight (g)163.2 ± 2.9168 ± 4.5166.9 ± 2.3169.4 ± 4.1156.5 ± 2.1158.6 ± 2.6Final body weight (g)182.3 ± 3.1175.6 ± 4.8180.2 ± 3.5178.9 ± 2.9181.1 ± 3.2183.5 ± 3^b^Liver weight (g)7.5 ± 0.36.8 ± 0.47.2 ± 0.37 ± 0.37.3 ± 0.27.4 ± 0.3^b^Data are expressed as Mean ± SEM, n = 5^*^p^#^p^a^p^b^p < 0.05 vs 250 mg/kg group^c^p
Histological analysis of the liver in acetaminophen-induced liver Damage in male Albino Wistar rats
Microscopic analysis of the liver, as illustrated in Fig. 1, showed that the liver tissue from the normal control group of adult Albino rats had a healthy structure. The liver cells appeared normal, with clearly defined nuclei and cell borders (Fig. 1A). However, in the group that received Acetaminophen, showing apoptotic hepatocytes with pyknotic nuclei and deep eosinophilic cytoplasm (yellow arrow) surrounding a central vein (green arrow), and inflammation (blue arrow) (Fig. 1B).Fig. 1. Photomicrograph showing a section of the liver from the different treatment groups (H&E; × 400)
Conversely, rats administered with silymarin along with medium or high doses of the aqueous Aloe vera gel extract (500 and 1000 mg/kg) showed no signs of liver tissue damage, and their physical condition was similar to that of the healthy control group (Fig. 1C, 1E, and 1 F). In contrast, rats that were given a lower dose of the extract (250 mg/kg) still showed liver damage similar to what was seen in the Acetaminophen group (Fig. 1D).
(A) In the normal control group treated with distilled water, hepatocytes appeared normal, featuring intact nuclei and distinct cellular outlines; and (B) negative control group (750 mg/kg of Acetaminophen) showing apoptotic hepatocytes with pyknotic nuclei and deep eosinophilic cytoplasm (yellow arrow) surrounding a central vein (green arrow), and inflammation (blue arrow) (C) positive control (50 mg/kg of silymarin), and (D, E and F) 250, 500 and 1000 mg\kg of the aqueous Aloe vera gel extract treated groups respectively presenting a comparatively normal liver histoarchitecture.
Effect of the aqueous Aloe vera gel extract on hematological parameters in male Albino Wistar rats following acetaminophen-induced liver Damage
White blood cell levels were much higher in the negative control group (13.8 ± 0.65 × 10⁹/L, p = 0.0051) than in the normal control group (8.9 ± 1.2 × 10⁹/L). However, treatment with Aloe vera gel extract at 500 mg/kg (9.1 ± 0.48 × 10⁹/L, p = 0.0076) and 1000 mg/kg (8.7 ± 0.51 × 10⁹/L, p = 0.0034) significantly reduced WBC levels compared to the negative control (Table 3).Table 3. White blood cell counts profile of rats following acetaminophen-induced liver damageHaematological parametersTreatment groupsNormal controlNegative controlSilymarin 50 mg/kg250 mg/kg of Aloe vera500 mg/kg of Aloe vera1000 mg/kg of Aloe veraWBC (10⁹/L)8.9 ± 1.213.8 ± 0.65^^9.8 ± 0.53^#^10.3 ± 1.39.1 ± 0.48^#^8.7 ± 0.51^#^Neutrophil (10⁹/L)1.84 ± 0.185.25 ± 0.42^^2.89 ± 0.26^#^4.46 ± 0.38^, a^3.25 ± 0.31^, #^2.92 ± 0.29^#, b^Lymphocyte (10⁹/L)7.1 ± 0.97.9 ± 1.17.2 ± 0.86.8 ± 0.76.5 ± 0.66.9 ± 0.7Monocyte (10⁹/L)0.1 ± 0.020.5 ± 0.1^^0.3 ± 0.050.4 ± 0.06^^0.2 ± 0.03^#^0.2 ± 0.08^#^Neutrophil %20 ± 1.838 ± 2.5^^27.5 ± 2.1 ^#^36 ± 2.4^^29 ± 2.2^, #^27 ± 2^#^Lymphocyte %74.9 ± 2.357 ± 2.7^^67 ± 2.5^#^59.3 ± 2.6^^66.3 ± 2.4^#^68.3 ± 2.3^#^Monocyte %5.1 ± 0.75 ± 0.85.5 ± 0.64.7 ± 0.74.7 ± 0.64.7 ± 0.7Data are expressed as Mean ± SEM; n = 5^^p < 0.05 vs normal control group^#^p < 0.05 vs negative control group^a^p < 0.05 vs positive control/silymarin 50 mg/kg group^b^p < 0.05 vs 250 mg/kg group
Neutrophil counts were elevated in the negative control group (p < 0.0001) and in the Aloe vera (250 and 500 mg/kg) groups (p < 0.0001 and p = 0.0441) when compared to the normal control group. There was a decrease in the neutrophil count of animals treated with the aqueous Aloe vera gel extract (500 and 1000 mg/kg) (p = 0.0020 and p = 0.0003) when compared to those in the negative control group. There was also a decrease in neutrophil counts of animals in the groups that received silymarin (50 mg/kg, p = 0.0198) and Aloe vera gel extract (1000 mg/kg, p = 0.0231) compared to those treated with Aloe vera gel extract at 250 mg/kg (Table 3).
Monocyte levels were much higher in the negative control (p = 0.0019) and in the 250 mg/kg Aloe vera gel extract group (p = 0.0272) when compared to the negative control. However, Aloe vera gel extract doses of 500 mg/kg and 1000 mg/kg significantly brought these levels down compared to the negative control group (p = 0.0272) (Table 3).
Red blood cell counts dropped significantly among animals in the negative control group (7.1 ± 0.06 × 10^12^/L, p = 0.0031) compared to the normal group (8.19 ± 0.13 × 10^12^/L). Treatment with silymarin (50 mg/kg) and Aloe vera gel extract at 500 mg/kg, and 1000 mg/kg increased RBC levels significantly compared to the negative control group (p = 0.0002, p = 0.0241 and p = 0.0184) (Table 4).Table 4. Erythropoietic profile of rats following acetaminophen-induced liver DamageErythropoietic parametersTreatment groupsNormal controlNegative controlSilymarin 50 mg/kg250 mg/kg of Aloe vera500 mg/kg of Aloe vera1000 mg/kg of Aloe veraRBC (10^12^/L)8.19 ± 0.137.1 ± 0.06 ^^7.9 ± 0.21 ^#^7.68 ± 0.067.97 ± 0.13 ^#^8 ± 0.33 ^#^HGB (g/dL)15.85 ± 0.2512.5 ± 0.6 ^^14.3 ± 0.2613.6 ± 0.5 ^^14.5 ± 0.4 ^#^15 ± 0.5 ^#^HCT (%)49.8 ± 0.241.2 ± 0.74 ^^46.8 ± 1.11 ^#^44.3 ± 0.92 ^^47.1 ± 0.63 ^#^48.5 ± 1.53 ^#, b^MCV (fL)60.83 ± 0.9849.88 ± 3.362.3 ± 0.7661.18 ± 1.0163 ± 0.4460.65 ± 0.82MCH (pg)19.33 ± 0.4317.6 ± 0.718.8 ± 0.618.1 ± 0.618.9 ± 0.519.1 ± 0.5MCHC (g/dL)31.8 ± 0.3730.2 ± 0.531.5 ± 0.430.8 ± 0.4 ^^31.4 ± 0.331.7 ± 0.3 ^b^PLT (/uL)639.3 ± 49.9400 ± 35 ^^580 ± 44.7520 ± 35.8590.3 ± 50.2620 ± 50.8 ^#^MPV (fL)7.4 ± 0.18.1 ± 0.26 ^^7.8 ± 0.128.3 ± 0.17 ^^7.7 ± 0.17.4 ± 0.13 ^#, b^PDW (%)15.9 ± 0.0718.2 ± 0.12 ^^16.5 ± 0.06 ^, #^17.3 ± 0.06 ^, #, a^16 ± 0.04 ^#, a, b^15.9 ± 0.11 ^#, a, b^PCT (%)0.47 ± 0.030.54 ± 0.020.54 ± 0.040.55 ± 0.020.51 ± 0.030.5 ± 0.04Data are expressed as Mean ± SEM; n = 5^*^p < 0.05 vs normal control group^#^p < 0.05 vs negative control group^a^p < 0.05 vs positive control/silymarin 50 mg/kg group^b^p < 0.05 vs 250 mg/kg group
Hemoglobin levels were also lower in the negative control (12.5 ± 0.6 g/dL, p = 0.0002) and the 250 mg/kg Aloe vera gel extract group (13.6 ± 0.5 g/dL, p = 0.0148) when compared to the normal control group (15.85 ± 0.25 g/dL). Aloe vera gel extract doses of 500 mg/kg (14.5 ± 0.4 g/dL) and 1000 mg/kg (15 ± 0.5 g/dL) significantly improved hemoglobin levels (p = 0.037 and p = 0.0057) respectively when compared to those in the negative control (Table 4).
Regarding the hematocrit (HCT) concentration, there was a decreased concentration among animals in the negative control group (p < 0.0001) and the 250 mg/kg Aloe vera group (p = 0.0049) compared to the normal control. Rats treated with silymarin or Aloe vera at 500 mg/kg and 1000 mg/kg had significantly higher HCT than those in the negative control group (p = 0.0041, p = 0.0024, and p = 0.0002). Also, HCT levels in rats treated with 1000 mg/kg Aloe vera were significantly higher than in those that received 250 mg/kg (p = 0.0461) (Table 4).
Mean corpuscular hemoglobin concentration was significantly lower in the 250 mg/kg Aloe vera gel extract group compared to both the normal control group (p = 0.0081) and the 1000 mg/kg Aloe vera group (p = 0.0117) (Table 4). The study also showed that platelet levels dropped significantly in the negative control group compared to both the normal control (p = 0.0108) and the 1000 mg/kg Aloe vera gel extract group (p = 0.0218) (Table 4).
There was a significant rise in mean corpuscular volume (MCV) in the negative control (p = 0.0437) and 250 mg/kg Aloe vera group (p = 0.0054) compared to the normal control. However, animals treated with 1000 mg/kg Aloe vera had significantly lower MCV levels than those in the negative control (p = 0.0437) and 250 mg/kg Aloe vera group (p = 0.0054) (Table 4).
Platelet distribution width was significantly higher in the negative control group, the positive control (silymarin 50 mg/kg), and Aloe vera250 mg/kg group (p < 0.0001, p = 0.0003, and p < 0.0001) respectively when compared to the negative control. However, silymarin and all Aloe vera gel extract doses (250, 500, and 1000 mg/kg) significantly lowered the platelet distribution width compared to the negative control group (p < 0.0001). The platelet distribution width values in the silymarin group were lower than in the Aloe vera 250 mg/kg group (p < 0.0001), but higher than in the 500 mg/kg (p = 0.0029) and 1000 mg/kg (p = 0.0003) Aloe vera groups (Table 4).
Effect of the aqueous Aloe vera gel extract on liver function biomarkers in male Albino Wistar rats following acetaminophen-induced liver Damage
The study noted that there was a statistically significant increase in the serum aspartate transferase concentration of animals in the toxic control group and those treated with Aloe vera (250 mg/kg and 500 mg/kg) aqueous gel extract (p < 0.0001, p = 0.0006 and p = 0.0008) when compared with those in the negative control group. The study also indicated that there was a statistically significant decrease in the serum aspartate transferase concentration of animals treated with the Aloe vera (250 and 500 and 1000 mg/kg) gel extract (p = 0.0129, p = 0.0102 and p < 0.0001) as compared to the negative control group. There was a statistically significant increase in the serum aspartate transferase concentration of animals treated with the Aloe vera (250 and 500 mg/kg) gel extract (p = 0.0127 and p = 0.0162) as opposed to those in the positive control group. Furthermore, the study indicated a significant increase in the serum aspartate transferase concentration of animals treated with the Aloe vera (250 and 500 mg/kg) gel extract (p = 0.0127 and p = 0.0162) as opposed to those treated with Aloe vera 1000 mg/kg gel extract (Table 5).Table 5. Effect of the aqueous Aloe vera gel extract on serum biochemical markers following acetaminophen-induced liver DamageAntioxidant parameters Treatment groupsNormal controlNegative controlSilymarin 50 mg/kg250 mg/kg of Aloe vera500 mg/kg of Aloe vera1000 mg/kg of Aloe veraAST (U/L)29.6 ± 4.192.8 ± 4.8 ^^45.2 ± 5.1 ^#^70.3 ± 6.1 ^, #, a^55.1 ± 5.5 ^, #, a^38.9 ± 4.7 ^#, b, c^ALT (U/L)49 ± 4.9116.3 ± 7.3 ^^69.9 ± 6.3 ^#^89.6 ± 7.4 ^^72.5 ± 6.8 ^^53.4 ± 9.2 ^#^Albumin (g/dL)6.34 ± 0.33.12 ± 0.2 ^^4.87 ± 0.2 ^, #^4.03 ± 0.1 ^^4.48 ± 0.5 ^, #^5.93 ± 0.3 ^#, b, c^Data are expressed as Mean ± SEM, n = 5^*^p < 0.05 vs normal control group^#^p < 0.05 vs negative control group^a^p < 0.05 vs positive control/silymarin 50 mg/kg group^b^p < 0.05 vs 250 mg/kg group^c^p < 0.05 vs 500 mg/kg group
The study indicated that there was a significant increase in the serum alanine transferase concentration of animals in the negative control group and those treated with the Aloe vera (250 and 500 mg/kg) gel extract (p = 0.0002, p = 0.0307 and p = 0.0271) when compared to those in the normal control group. The study also noted a significant decrease in the serum alanine transferase concentration of animals treated with the Aloe vera (1000 mg/kg) gel extract (p = 0.0004) when compared to those in the negative control group (Table 5).
Regarding the serum albumin concentration, the study indicated that it was significantly decreased among animals in the negative and positive control groups (p < 0.0001 and p = 0.0125) and those treated with the aqueous Aloe vera gel extract (250 and 500 mg/kg) (p < 0.0001 and p = 0.0012) when compared to those in the normal control group. The study also indicated a significant increase in the serum albumin concentration of animals treated with the aqueous Aloe vera gel extract (500 and 1000 mg/kg) (p = 0.0227 and p < 0.0001) when compared to those in the negative control group. Furthermore, the study indicated a significant increase in the serum albumin concentration of animals treated with the Aloe vera (250 and 500 mg/kg) gel extract (p = 0.0009 and p = 0.0142) as opposed to those treated with the Aloe vera1000 mg/kg gel extract (Table 5).
Antioxidant effects following acetaminophen-induced liver damage
Administration of acetaminophen led to a marked increase in liver malondialdehyde concentrations in the negative control group compared to the normal control (p < 0.0001). Treatment with Aloe vera gel extract significantly lowered MDA levels at doses of 250 mg/kg (p = 0.0012), 500 mg/kg (p < 0.0001), and 1000 mg/kg (p < 0.0001) relative to the negative control group. Additionally, animals receiving the 1000 mg/kg dose of aqueous Aloe vera gel extract exhibited a significant reduction in liver tissue MDA levels compared to those treated with 250 mg/kg (p = 0.0383) (Table 6).Table 6. Effect of the aqueous Aloe vera gel extract on the antioxidant parameters of male Albino Wistar rats following acetaminophen-induced liver DamageAntioxidant parametersTreatment groupsNormal controlNegative controlSilymarin 50 mg/kg250 mg/kg of Aloe vera500 mg/kg of Aloe vera1000 mg/kg of Aloe veraMDA (nmol/mg protein1.63 ± 0.174.9 ± 0.3 ^^1.65 ± 0.16 ^#^2.9 ± 0.5 ^#^1.8 ± 0.3 ^#^1.5 ± 0.2 ^#, b^SOD (U/mg protein)78 ± 4.940 ± 3.2 ^^64.4 ± 2.7 ^#^48 ± 3.7 ^^56 ± 5.1 ^^76 ± 2.4 ^#, b, c^CAT (U/mg of protein)122.6 ± 2.2100 ± 2.7 ^^111 ± 4.5100.1 ± 2.5 ^^107.7 ± 3.7 ^^114.1 ± 3.6Data are expressed as Mean ± SEM, n = 5^^p < 0.05 vs normal control group^#^p < 0.05 vs negative control group^b^p < 0.05 vs 250 mg/kg group^c^p < 0.05 vs 500 mg/kg group
Superoxide dismutase activity was significantly reduced in the negative control group (p < 0.0001) and in the groups treated with Aloe vera gel extract at 250 mg/kg and 500 mg/kg (p = 0.0001 and p = 0.0051, respectively) when compared to the normal control. Treatment with the 1000 mg/kg Aloe vera gel extract significantly boosted SOD levels (p < 0.0001) compared to the negative control. furthermore, treatment with 1000 mg/kg of Aloe vera resulted in enhanced SOD activity when compared to the 250 mg/kg (p = 0.0003) and 500 mg/kg (p = 0.0125) treatment groups (Table 6).
The study also indicated a significant decline in catalase enzyme concentration within liver tissues of the negative control animals (p = 0.0007) and those treated with Aloe vera at 250 mg/kg and 500 mg/kg (p = 0.0008 and p = 0.039, respectively) compared to the normal control group (Table 6).
Discussion
The aqueous extraction of Aloe vera gel yielded 2.02%. This aligns with previous findings where Aloe vera gel extracts have demonstrated moderate yields depending on solvent type and processing method [1]. The phytochemical analysis confirmed the presence of tannins, flavonoids, saponins, anthraquinones, amino acids, and alkaloids. These bioactive compounds have been widely reported to possess hepatoprotective, antioxidant, and anti-inflammatory properties, which may explain Aloe vera’s potential role in mitigating acetaminophen-induced liver Damage [2].
Recent studies have confirmed that Aloe vera gel contains bioactive compounds such as flavonoids, tannins, saponins, anthraquinones, and polysaccharides, which contribute to its medicinal properties. A study by Manye et al*.* demonstrated that aqueous Aloe vera gel extract possesses flavonoids and anthraquinones which have strong antioxidant properties, that help to inhibit lipid peroxidation [21]. Another study by Raad et al*.* found that Aloe vera’s phytochemicals play a significant role in reducing oxidative stress in hepatocytes, and also support tissue repair and collagen synthesis [22].
Acetaminophen overdose is known to cause hepatocellular necrosis primarily through the excessive generation of reactive oxygen species and subsequent oxidative stress [3]. Regarding the morphological effects on the organs, the study findings suggest that the aqueous extract of Aloe vera gel, particularly at 500 and 1000 mg/kg dose, was able to ameliorate the liver Damage attributable to acetaminophen. The absence of visible changes in the 1000 mg/kg group indicates that the higher dose of the extract did not exacerbate or cause any additional liver damage. Histopathological findings indicated that the aqueous Aloe vera gel extract, particularly at higher doses (500 mg/kg and 1000 mg/kg), effectively ameliorated the acetaminophen-induced liver Damage. This ameliorative effect is attributed to the presence of bioactive compounds that counteract oxidative stress and inflammation, aligning with studies on Aloe vera’s restorative effects[4]. The study recorded a significant recovery in liver weight at 1000 mg/kg toward normal levels, suggesting protection against the hepatic changes associated with acetaminophen-induced damage. This normalization aligns with Aloe vera’s ability to stimulate hepatocyte proliferation via polysaccharide-mediated activation of growth factors [5]. Flavonoids and saponins enhance liver tissue repair and regeneration. Histological studies demonstrated that aqueous Aloe vera gel extract reduces hepatic necrosis, inflammation, and fibrosis [6]. Hossain et al. found that Aloe vera gel reduced liver necrosis and improved tissue structure in Albino rats [13]. Khan et al. showed Aloe vera restores hepatocyte integrity by reducing fibrosis and cellular damage in drug-induced liver toxicity [7].
The haematological findings revealed significant alterations in white blood cell, red blood cell, haemoglobin, and haematocrit levels following acetaminophen-induced liver damage. Increased WBC and neutrophil counts in the toxic control group align with existing literature on acetaminophen-induced systemic inflammation [7]. Aloe vera gel extract (500 and 1000 mg/kg) reduced WBC and neutrophil counts, suggesting an anti-inflammatory role via modulation of cytokine release and inhibition of pro-inflammatory cytokines and neutrophil infiltration [6]. Aloe vera has been found to improve haematological parameters, particularly RBC count, haemoglobin levels, and WBC modulation. Bala et al. showed that Aloe vera reduced leucocytosis and neutrophilia caused by acetaminophen-induced inflammation [8].
RBC, HGB, and HCT levels were reduced in the negative control but improved in Aloe vera-treated groups, suggesting protection against acetaminophen-induced hematotoxicity, likely due to antioxidant properties counteracting oxidative damage to erythrocyte membranes and enhanced iron utilization [9]. Platelet counts, reduced in the negative control, improved with Aloe vera treatment, indicating benefits in preventing thrombocytopenia due to impaired thrombopoietin synthesis. Kishore et al. showed Aloe vera maintains platelet homeostasis [10].
Serum aspartate aminotransferase and alanine aminotransferase levels, elevated in acetaminophen-induced liver damage, indicate hepatocyte necrosis [11]. Aloe vera treatment, particularly at 1000 mg/kg, reduced AST and ALT levels, suggesting hepatoprotective effects. Biochemical studies confirm Aloe vera’s role in normalizing liver enzyme levels through membrane stabilization by polysaccharides, preventing NAPQI-induced mitochondrial permeability transition and preserving ATP synthesis [6].
Flavonoids block APAP bioactivation, reducing oxidative stress [12]. Abaekwume and Kagbo demonstrated that Aloe vera reduced AST and ALT levels in acetaminophen-treated rats [13]. Treatment with aqueous Aloe vera gel extract increased serum albumin concentrations, with notable improvements at higher doses, indicating dose-dependent restoration of liver synthetic function. Ebenyi et al*.* reported similar dose-dependent albumin elevation with Aloe vera extracts in paracetamol-induced hepatotoxicity [14–16].
Oxidative stress is a key mechanism in acetaminophen-induced liver damage. Aqueous Aloe vera gel extract reduced MDA levels, a marker of lipid peroxidation, while enhancing SOD and CAT activities, corroborating research that Aloe vera enhances endogenous antioxidant defenses [17]. Aloe vera has Aloe vera upregulates SOD, catalase, and reduces malondialdehyde via Nrf2-mediated upregulation of antioxidant enzymes [17, 18]. Klaikeaw et al*.* reported that Aloe vera significantly reduced oxidative stress markers in the liver [19].
The therapeutic potential of aqueous Aloe vera gel extract depends on its antioxidant mechanisms, with bioactive compounds inhibiting acetaminophen-induced tissue damage. These results are consistent with studies on Aloe vera’s hepatoprotective properties [20–22].
This study was limited by the relatively short duration of treatment, preventing the assessment of long-term efficacy and safety. Extended treatment studies would be valuable to determine the optimal treatment duration and potential for adverse effects with prolonged administration. The study utilized a therapeutic treatment protocol, administering Aloe vera extract after acetaminophen challenge. Future studies should explore preventive protocols, administering the extract before established liver injury, to assess its potential for preventing, rather than treating acetaminophen hepatotoxicity.
Future studies should include additional antioxidant enzymes, such as glutathione peroxidase (GSH-Px), to further elucidate the antioxidant mechanisms of Aloe vera gel extract.
Conclusion
This study demonstrates that aqueous Aloe vera gel extract mitigates acetaminophen-induced liver damage through antioxidant, anti-inflammatory, and regenerative mechanisms. At 1000 mg/kg, it restored hepatic histoarchitecture, hematological homeostasis, normalized liver function biomarkers, and suppressed oxidative stress, with efficacy comparable to silymarin. These effects are driven by bioactive constituents like flavonoids, anthraquinones, and polysaccharides, which counteract NAPQI-induced damage and promote tissue repair. Future studies should explore preventive protocols, long-term safety, and clinical translation to validate Aloe vera’s therapeutic potential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nalimu F, Oloro J, Peter EL, Ogwang PE. Acute and sub-acute oral toxicity of aqueous whole leaf and green rind extracts of Aloe vera in Wistar rats. BMC Complementary Medicine and Therapies. 2022;22(1):16. 10.1186/s 12906-021-03470-4PMC 876073135031035 · doi ↗ · pubmed ↗
- 2Prescott LF. Paracetamol (acetaminophen) poisoning: The early years. British journal of clinical pharmacology. 2024;90(1):127–34.10.1111/bcp.1590337683599 · doi ↗ · pubmed ↗
- 3Panda S, Sharma R, Khan A, Kar A. Ameliorative effect of Aloe gel against L-T 4-induced hyperthyroidism via suppression of thyrotropin receptors, inflammation and oxidative stress. Molecular biology reports. 2020;47(4):2801–10. 10.1007/s 11033-020-05405-732242301 · doi ↗ · pubmed ↗
- 4Farooq S, Shaheen G, Asif HM, Aslam MR, Zahid R, Rajpoot SR, et al. Preliminary phytochemical analysis: In-Vitro comparative evaluation of anti-arthritic and anti-inflammatory potential of some traditionally used medicinal plants. Dose-Response. 2022;20(1):15593258211069720.10.1177/15593258211069720 PMC 875308035069052 · doi ↗ · pubmed ↗
- 5Bala S, Chugh NA, Bansal SC, Koul A. Aloe vera modulates X-ray induced hematological and splenic tissue damage in mice. Human & experimental toxicology. 2019 Oct;38(10):1195 -211.10.1177/096032711986017431256688 · doi ↗ · pubmed ↗
- 6Orrico F, Laurance S, Lopez AC, Lefevre SD, Thomson L, Möller MN, Ostuni MA. Oxidative stress in healthy and pathological red blood cells. Biomolecules. 2023 Aug 18;13(8):1262.10.3390/biom 13081262 PMC 1045211437627327 · doi ↗ · pubmed ↗
- 7Ishida Y, Zhang S, Kuninaka Y, Ishigami A, Nosaka M, Harie I, Kimura A, Mukaida N, Kondo T. Essential involvement of neutrophil elastase in acute acetaminophen hepatotoxicity using BALB/c mice. International Journal of Molecular Sciences. 2023 Apr 25;24(9):7845. 10.3390/ijms 24097845 PMC 1017787337175553 · doi ↗ · pubmed ↗
- 8Abdel-Daim M, Abushouk AI, Reggi R, Yarla NS, Palmery M, Peluso I. Association of antioxidant nutraceuticals and acetaminophen (paracetamol): Friend or foe?. journal of food and drug analysis. 2018 Apr 1;26(2):S 78-87. 10.1016/j.jfda.2017.11.004PMC 932688229703389 · doi ↗ · pubmed ↗