The Association of Periodontitis and Stroke History: Exploring the Role of Hypertension in a Cross‐Sectional NHANES Analysis
Shi-Yin Jin, Qing Liu, Xiao-Qing Cao, Dian-Wei Wu, Yun-Fan Cai, Li-Na Niu, Wen Qin, Tao Ye

TL;DR
This study explores how periodontitis and stroke are linked, finding that hypertension plays a key role in their relationship.
Contribution
The study identifies hypertension as a significant mediator in the association between periodontitis and stroke using NHANES data.
Findings
Periodontitis was initially strongly associated with stroke, but this link disappeared after adjusting for other factors.
Hypertension was found to mediate 31.3% of the association between periodontitis and stroke.
The direct effect of periodontitis on stroke was not significant after accounting for hypertension.
Abstract
Periodontitis, a chronic inflammatory disease, and stroke, a leading cause of death and disability, share common risk factors and inflammatory pathways. However, the role of key mediators such as hypertension in this relationship remains to be fully elucidated. This cross‐sectional analysis was conducted using data from the NHANES 2009–2014. Participants aged 30 years and older with complete periodontal and stroke data were included (n = 2,783). Periodontitis was classified according to standard NHANES protocols. Stroke history was self‐reported. Survey‐weighted multivariable logistic regression was used to assess the periodontitis‐stroke association. Mediation analysis was performed to quantify the indirect association mediated through hypertension. In unadjusted models, periodontitis was significantly associated with stroke (OR: 5.69; 95% CI: 2.24–20.61). After full adjustment, this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
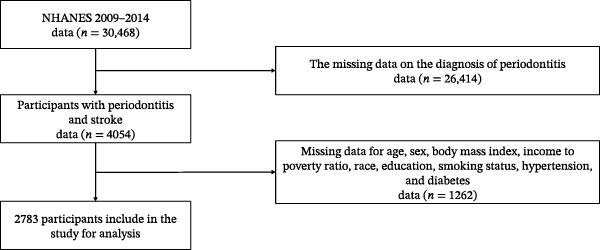 Figure 1
Figure 1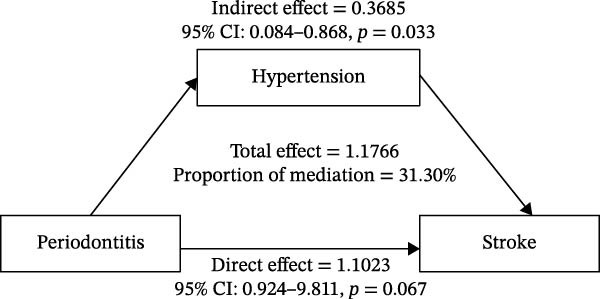 Figure 2
Figure 2| Characteristic | Total ( | No Periodontitis ( | Periodontitis ( |
|
|---|---|---|---|---|
| Stroke | <0.001 | |||
| No | 2707 (97.27%) | 577 (99.48%) | 2130 (96.69%) | |
| Yes | 76 (2.73%) | 3 (0.52%) | 73 (3.31%) | |
| Age | 50.87 ± 13.60 | 44.93 ± 11.14 | 53.06 ± 13.77 | <0.001 |
| Gender | 0.6 | |||
| Male | 1243 (44.66%) | 256 (44.14%) | 987 (44.80%) | |
| Female | 1540 (55.34%) | 324 (55.86%) | 1216 (55.20%) | |
| Race | <0.001 | |||
| Non‐Hispanic White | 592 (21.27%) | 92 (15.86%) | 500 (22.70%) | |
| Non‐Hispanic Black | 1179 (42.36%) | 294 (50.69%) | 885 (40.17%) | |
| Hispanic | 609 (21.88%) | 93 (16.03%) | 516 (23.42%) | |
| Other/Multirace | 403 (14.48%) | 101 (17.41%) | 302 (13.71%) | |
| Hypertension | 1608 (57.78%) | 242 (41.72%) | 1366 (62.01%) | <0.001 |
| Diabetes status | 359 (12.90%) | 35 (6.03%) | 324 (14.71%) | 0.001 |
| Smoking status | <0.001 | |||
| Never | 2042 (73.37%) | 507 (87.41%) | 1535 (69.68%) | |
| Ever | 741 (26.63%) | 73 (12.59%) | 668 (30.32%) | |
| Education | <0.001 | |||
| High school or less | 589 (21.16%) | 39 (6.72%) | 550 (24.97%) | |
| High school graduate | 594 (21.34%) | 74 (12.76%) | 520 (23.60%) | |
| Some college or more | 1600 (57.49%) | 467 (80.52%) | 1133 (51.43%) | |
| Alcohol | 1872 (67.27%) | 417 (71.90%) | 1455 (66.05%) | 0.4 |
| BMI | 29.32 ± 6.92 | 28.80 ± 6.66 | 29.51 ± 7.01 | 0.046 |
| Family poverty income ratio | 3.10 (1.47, 5.00) | 3.83 ± 1.44 | 2.73 ± 1.64 | <0.001 |
| eGFR | 92.09 ± 19.04 | 95.48 ± 17.00 | 90.82 ± 19.61 | <0.001 |
| WBC | 7.32 ± 2.28 | 7.05 ± 2.13 | 7.42 ± 2.33 | 0.042 |
| TG | 1.79 ± 1.76 | 1.67 ± 1.39 | 1.84 ± 1.88 | <0.001 |
| Glu | 103.33 ± 37.24 | 98.08 ± 31.46 | 105.29 ± 39.01 | <0.001 |
| Variable | Number of subjects | Number of stroke | Unadjusted model | Age, sex‐adjusted model | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
| |||
| No periodontitis | 580 | 3 | 1.00 (ref) | <0.001 | 1.00 (ref) | 0.034 | 1.00 (ref) | 0.175 | 1.00 (ref) | 0.486 |
| Periodontitis | 2203 | 73 | 5.69 (2.24, 20.61) | 2.81 (1.07, 10.35) | 2.06 (0.75, 7.79) | 1.48 (0.53, 5.67) | ||||
| Variable | Subgroup | Number of stroke /total | Unadjusted | Age, sex‐adjusted | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
| OR (95% CI) |
| |||
| Age | <45 years | 4/1024 | 4.52 (0.48–600.04)a | 0.220 | 4.40 (0.46–588.00)a | 0.235 | 5.57 (0.49–776.38)a | 0.190 | 3.45 (0.32–468.81)a | 0.351 |
| 45–64 years | 29/1165 | 2.85 (0.85–17.76) | 0.155 | 2.50 (0.73–15.73) | 0.217 | 1.94 (0.53–12.55) | 0.390 | 1.54 (0.40–10.12) | 0.581 | |
| ≥65 years | 43/594 | 3.11 (0.65–55.90) | 0.268 | 2.81 (0.57–50.69) | 0.317 | 2.66 (0.51–48.90) | 0.351 | 2.54 (0.49–46.73) | 0.373 | |
| Gender | Male | 30/1243 | 3.71 (1.11–23.06) | 0.075 | 1.65 (0.45–10.61) | 0.513 | 1.06 (0.26–7.22) | 0.942 | 0.69 (0.15–4.86) | 0.657 |
| Female | 46/1540 | 12.41 (2.70–220.35) | 0.013 | 6.44 (1.36–115.39) | 0.068 | 6.48 (1.33–117.18) | 0.070 | 4.75 (0.95–86.33) | 0.133 | |
| Hypertension | No | 8/1175 | 6.94 (0.86–897.91)a | 0.075 | 4.47 (0.51–587.44)a | 0.212 | 5.64 (0.60–754.20)a | 0.152 | 3.69 (0.37–496.65)a | 0.312 |
| Yes | 68/1608 | 3.98 (1.46–16.37) | 0.020 | 2.34 (0.83–9.76) | 0.161 | 1.99 (0.68–8.49) | 0.268 | 1.56 (0.52–6.71) | 0.482 | |
| Diabetes | No | 53/2424 | 4.94 (1.81–20.36) | 0.007 | 2.41 (0.85–10.15) | 0.149 | 2.15 (0.72–9.26) | 0.225 | 3.44 (1.21–14.51) | 0.044 |
| Yes | 23/359 | 5.53 (0.74–708.16)a | 0.114 | 4.02 (0.51–518.54)a | 0.235 | 3.89 (0.48–504.62)a | 0.253 | 4.35 (0.54–563.49)a | 0.206 | |
| BMI | Underweight (<18.5) | 1/38 | — | — | — | 0.619 | — | — | — | — |
| Normal (18.5–24.9) | 22/741 | 6.45 (1.34–116.10) | 0.069 | 2.95 (0.57–54.20) | 0.304 | 2.15 (0.36–41.52) | 0.485 | 1.57 (0.24–30.99) | 0.685 | |
| Overweight (25.0–29.9) | 30/922 | 7.74 (1.64–138.44) | 0.045 | 3.75 (0.74–68.44) | 0.204 | 2.90 (0.55–53.67) | 0.313 | 2.18 (0.40–40.83) | 0.465 | |
| Obese (≥30.0) | 23/1082 | 5.67 (1.18–101.82) | 0.091 | 2.93 (0.58–53.53) | 0.303 | 3.42 (0.64–63.42) | 0.245 | 2.30 (0.41–43.26) | 0.437 | |
| Smoking | Never | 45/2042 | 4.73 (1.71–19.57) | 0.010 | 1.66 (0.56–7.12) | 0.417 | 1.37 (0.44–6.01) | 0.624 | 3.01 (1.05–12.74) | 0.073 |
| Ever/former | 31/741 | 7.26 (1.01–923.30)a | 0.049 | 3.53 (0.46–455.09)a | 0.287 | 4.50 (0.55–584.91)a | 0.198 | 6.33 (0.82–814.76)a | 0.086 | |
| Alcohol | Nondrinker | 32/911 | 14.83 (2.08–1881.41)a | 0.002 | 5.63 (0.74–722.90)a | 0.113 | 5.63 (0.72–726.57)a | 0.119 | 3.92 (0.49–508.84)a | 0.249 |
| Drinker | 44/1872 | 4.00 (1.45–16.59) | 0.021 | 2.30 (0.80–9.70) | 0.176 | 1.79 (0.58–7.80) | 0.365 | 1.34 (0.42–5.93) | 0.655 | |
- —National Natural Science Foundation of China10.13039/501100001809
- —Project of State Key Laboratory of Oral & Maxillofacial Reconstruction and Regeneration
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Dental Radiography and Imaging · Forensic Anthropology and Bioarchaeology Studies
1. Introduction
Periodontitis is a chronic inflammatory disease characterized by the progressive destruction of tooth‐supporting structures, including the periodontal ligament and alveolar bone. The condition manifests through gingival inflammation, clinical attachment loss (AL), increased probing depths (PDs), and alveolar bone resorption [1]. As one of the most prevalent chronic diseases worldwide, periodontitis affects ~11.2% of the global population and represents a significant public health burden [2]. The disease’s impact extends beyond oral health, with mounting evidence suggesting associations with various systemic conditions [3].
Stroke, the second‐leading cause of death globally, affects ~795,000 Americans annually with substantial healthcare costs and disability burden [4, 5]. The potential association between periodontitis and stroke has gained scientific interest due to shared biological pathways involving chronic inflammation, bacterial translocation, and common risk factors [6, 7].
Several mechanisms may link periodontitis to stroke. Chronic periodontal inflammation elevates systemic inflammatory markers, contributing to endothelial dysfunction and atherosclerosis [8]. Periodontal pathogens like P. gingivalis can enter systemic circulation, potentially triggering vascular inflammation and plaque instability [9]. Additionally, both conditions share multiple risk factors, including age, smoking, diabetes, socioeconomic status, and notably, hypertension [7, 10]. Among these shared risk factors, the relationship with hypertension deserves particular attention due to its dual role as both a consequence of periodontal inflammation and the most potent modifiable risk factor for stroke.
Hypertension represents a critical mediator in the periodontitis‐stroke pathway. Beyond being a shared risk factor, chronic periodontal inflammation may actively contribute to blood pressure elevation through endothelial dysfunction, increased arterial stiffness, and activation of the renin–angiotensin system [11]. Meta‐analytic evidence demonstrates that individuals with periodontitis have significantly higher blood pressure and increased hypertension prevalence compared to periodontally healthy individuals [12]. Given that hypertension accounts for ~50% of stroke risk, understanding how periodontitis may both share and potentially exacerbate this crucial risk factor has profound implications for stroke prevention strategies [13].
Previous studies have been limited by inadequate confounder control and lack of standardized periodontal assessments. The National Health and Nutrition Examination Survey (NHANES) addresses these limitations through comprehensive periodontal examinations, detailed health assessments, and a nationally representative sampling design.
Therefore, this study investigates the association between periodontitis and stroke using NHANES 2009–2014 data. We aimed to: (1) examine the relationship between periodontitis and stroke in US adults after adjusting for potential confounding factors and (2) investigate which factors mediate the periodontitis‐stroke association, with particular focus on hypertension.
2. Materials and Methods
2.1. Study Population
We conducted a cross‐sectional analysis using data from the NHANES 2009–2014 cycles. All data and materials are publicly available on the National Center for Health Statistics website (https://www.cdc.gov/nchs/nhanes/index.htm). For this analysis, we included participants aged 30 years and older with complete periodontal examinations and at least one remaining tooth. Participants with missing data on key variables (periodontal status, stroke history, and essential covariates) were excluded from the analysis.
2.2. Assessment of Periodontal Disease
Periodontal examinations were conducted by trained dental examiners following standardized NHANES protocols [14]. The classification of periodontal disease is divided into two categories: presence of periodontitis, which includes participants who meet the criteria for any degree of periodontitis; and no periodontitis, which refers to participants not meeting the criteria for any degree [15]. For those classified as having periodontitis, the severity is further graded as follows: mild periodontitis is defined as having ≥2 teeth with clinical AL ≥3 mm and ≥2 teeth with PD ≥4 mm, or any site with PD ≥5 mm; moderate periodontitis is indicated by ≥2 teeth with AL ≥4 mm or ≥2 teeth with PD ≥ 5mm; and severe periodontitis is characterized by ≥2 teeth with AL ≥6 mm and ≥1 tooth with PD ≥5 mm [16].
2.3. Assessment of Stroke
Stroke history was ascertained through self‐reported physician diagnosis during the NHANES interview, a method that has been validated in previous epidemiological studies [17]. Participants were classified as having a stroke history if they answered “yes” to the question about whether a doctor had ever told them they had a stroke.
2.4. Covariates and Potential Mediators
Demographic variables included age, sex, race/ethnicity, education level, and family income‐to‐poverty ratio. Lifestyle factors included smoking status (never, former, and current) and body mass index (BMI). Clinical covariates included diabetes status (based on self‐report, medication use, or laboratory values), estimated glomerular filtration rate (eGFR, calculated using the 2021 CKD‐EPI equation without race coefficient), fasting glucose, and triglycerides [18]. Hypertension was defined according to the 2017 American Heart Association/American College of Cardiology guidelines as having systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥80 mmHg (based on the average of available measurements), or currently taking antihypertensive medication, or self‐reported physician diagnosis of hypertension [19]. Blood pressure measurements were obtained following standardized NHANES protocols during the examination. White blood cell count (WBC) was considered as a potential inflammatory mediator in the periodontitis‐stroke pathway, as systemic inflammation represents a key mechanistic link between periodontal infection and cardiovascular outcomes [7]. WBC values were standardized (z‐scores) for analysis. Other potential mediators examined included hypertension, diabetes, and metabolic factors that may lie on the causal pathway from periodontitis to stroke.
2.5. Statistical Analysis
All analyses accounted for the complex NHANES sampling design using appropriate survey weights (WTMEC2YR), stratification variables (SDMVSTRA), and primary sampling units (SDMVPSU) [20]. For pooled cycles, weights were divided by the number of cycles included to obtain proper population estimates. Population characteristics were presented as means with standard errors for continuous variables and as percentages with standard errors for categorical variables. Group differences were evaluated using the Wilcoxon rank‐sum test for continuous data and the Rao–Scott chi‐squared test tailored for complex survey samples when examining categorical data. The relationship between periodontal disease and stroke was examined using weighted multivariable logistic regression to calculate odds ratios (OR), adjusting for potential confounding factors [21]. Additionally, we used Firth regression to address potential issues with sparse data and better estimate the relationships involving low‐frequency outcomes. The NHANES protocol was approved by the Institutional Review Board of the National Center for Health Statistics, Centers for Disease Control and Prevention, and all participants provided informed consent. A total of 30,468 participants aged 30 years or older were included in this study, 26,414 participants were excluded from the study due to incomplete data on periodontitis and stroke, and an additional 1262 participants were excluded due to missing data on other covariates. Ultimately, 2783 participants were included in the study (Figure 1).
The flowchart of this study.
For mediation analysis, we used regression‐based mediation analysis methods implemented in the CMAverse R package to decompose the total association of periodontal disease on stroke into direct and indirect association through potential mediators [22]. The analysis employed loglinear models for the binary outcome and linear models for continuous mediators, with bootstrap confidence intervals (1000 iterations) for statistical inference. We examined multiple potential mediators, including hypertension, diabetes, inflammatory markers, and other risk factors, to identify the key pathways linking periodontal disease to stroke. All statistical analyses were performed in R (version 4.5.1), and statistical significance was defined as p < 0.05.
3. Results
3.1. Demographic, Clinical Characteristics of the Study Population
From NHANES 2009–2014, a total of 2783 participants were included in the analysis, all of whom completed periodontal assessments and relevant health questionnaires. Table 1 summarizes baseline demographic and health‐related characteristics, including the distribution of periodontitis within the study population. The overall age was 50 years (IQR 40–60). The median Family Poverty Income Ratio was 3.10 (IQR 1.47–5.00). Males accounted for 44.66% of the cohort. Overall, 26.63% were ever smokers, and 67.27% were current alcohol consumers. The prevalence of hypertension, diabetes mellitus, and stroke was 57.78%, 12.90%, and 2.73%, respectively. Periodontitis was present in 2203 participants (79.2%), while 580 (20.8%) had no periodontitis.
Hypertension and stroke. Hypertension was more frequent in participants with periodontitis than in those without (62.01% vs. 41.72%; p < 0.001; Rao–Scott χ ^2^). Stroke was also more common in the periodontitis group (3.31% vs. 0.52%; p < 0.001; Rao–Scott χ ^2^).
Significant between‐group differences (p < 0.05; Rao–Scott χ ^2^ for categorical variables; survey‐weighted Wilcoxon rank‐sum test for continuous variables) were observed for age, family Poverty Income Ratio, race/ethnicity, education, BMI, smoking status, hypertension, diabetes mellitus, stroke, eGFR, WBC, triglycerides, and glucose.
3.2. Association Between Periodontitis and Stroke
In survey‐weighted logistic regression, stroke events occurred in 73 of 2203 participants with periodontitis and in 3 of 580 without periodontitis (Table 2). Compared with no periodontitis, periodontitis was associated with higher odds of stroke in the unadjusted model (OR: 5.69; 95% CI: 2.24–20.61; p < 0.001; survey‐weighted logistic regression), which attenuated after adjusting for age and sex (OR: 2.81; 95% CI: 1.07–10.35; p = 0.034; survey‐weighted logistic regression). After further adjustment for race, education, and income (Model 1), the association was no longer statistically significant (OR: 2.06; 95% CI: 0.75–7.79; p = 0.175; survey‐weighted logistic regression). In the fully adjusted model additionally controlling for smoking status, alcohol use, hypertension, and diabetes (Model 2), the association remained nonsignificant (OR: 1.48; 95% CI: 0.53–5.67; p = 0.486; survey‐weighted logistic regression), indicating no independent association between periodontitis and stroke after adjusting for age, sex, race, education, income, smoking status, alcohol use, hypertension, and diabetes.
3.3. Subgroup Analyses of the Association Between Periodontitis and Stroke
In survey‐weighted subgroup analyses (Table 3), findings were broadly consistent with the main results. In the fully adjusted model (Model 2, controlling for age, sex, race/ethnicity, education, income, smoking, alcohol use, hypertension, and diabetes), no age stratum showed a statistically significant association between periodontitis and stroke, and no clear age gradient was evident. By sex, the association appeared stronger among females, whereas estimates for males were more modest and imprecise; however, wide confidence intervals across both strata limit definitive inference. Stratification by hypertension suggested a higher odds of stroke among participants with hypertension, but neither the hypertensive nor the nonhypertensive groups reached statistical significance. Similarly, the association was detectable among participants without diabetes, while estimates among those with diabetes were highly imprecise; neither subgroup met conventional significance thresholds. It is worth noting that certain subgroups, particularly those aged <45 years, exhibited wide confidence intervals due to limited sample size, warranting cautious interpretation of these estimates.
3.4. Mediation Analysis of Hypertension
To explore the mechanism connecting periodontitis to stroke, a mediation analysis was performed with hypertension as the proposed mediator (Figure 2). Notably, no mediating association was identified for the other variables. The analysis revealed a significant pathway from periodontitis to hypertension and from hypertension to stroke. The results demonstrated a significant indirect association of periodontitis on stroke through hypertension (indirect association coefficient = 0.3685, 95% CI: 0.085–0.868, p = 0.033). This indirect pathway accounted for 31.30% of the total association. In contrast, the direct association of periodontitis on stroke, after controlling for hypertension (path c’), was not statistically significant (direct association coefficient = 1.1023, 95% CI: 0.924–9.811, p = 0.067). Given that the direct association was nonsignificant while the indirect association was significant, these findings are consistent with complete mediation.
A proposed associative pathway model among periodontitis, hypertension, and stroke history, based on cross‐sectional data.
4. Discussion
In this study, we explored the relationship between periodontitis and the risk of stroke using data from NHANES 2009–2014 comprising 2783 adults. Our discussion focuses on three core findings. First, our analysis indicated a significant association between periodontitis and stroke in unadjusted models, which exhibited an OR of 5.69 (95% CI: 2.24–20.61). However, after adjusting for potential confounders, including sociodemographic variables, lifestyle factors, and comorbidities, this association became nonsignificant. The fully adjusted model resulted in a nonsignificant OR of 1.48 (95% CI: 0.53–5.67), indicating that periodontitis may not be independently associated with stroke history in this population when accounting for hypertension. Second, hypertension emerged as a key variable strongly linked to both conditions. It absorbed a significant portion of the variance, suggesting it plays a central role in the comorbidity profile of these patients. Third, our mediation analysis revealed that hypertension serves as a significant mediator in the periodontitis‐stroke relationship, accounting for ~31.30% of the total association. This identifies hypertension as an important node in the associative network, but longitudinal studies are required for verification. This finding suggests that the impact of periodontal health on cerebrovascular events may operate primarily through its influence on blood pressure regulation rather than through direct mechanisms.
Our results align with several large epidemiological studies that have reported a diminished association between periodontitis and stroke after adjusting for cardiovascular risk factors. For instance, a meta‐analysis conducted by Leira et al. [23] found that while crude estimates indicated a strong relationship, the associations weakened significantly when controlling for potential confounders. Similarly, Lafon et al. [24], in a prospective cohort study, revealed that the association was no longer significant after adjustment for traditional risk factors. Conversely, some studies have shown conflicting conclusions, such as those by Grau et al. [25] and Chen et al. [26], which demonstrated significant associations after adjusting for certain covariates. These differences may stem from variations in study design, definitions of periodontal disease, and the extent of confounding factors accounted for. Our comprehensive adjustment strategy, particularly the inclusion of hypertension as a potential mediator, allows us to more accurately assess the independent association of periodontitis with stroke. This finding provides a clearer perspective on the relationship between periodontal health and cardiovascular health.
The role of hypertension as a mediator between periodontitis and stroke highlights the importance of addressing blood pressure when managing periodontal disease. Chronic periodontal inflammation can initiate systemic inflammatory responses, resulting in increased levels of pro‐inflammatory markers such as C‐reactive protein and interleukin‐6, which are known to contribute to hypertension [27]. Furthermore, the direct invasion of periodontal pathogens into the vascular system can exacerbate hypertension and increase stroke vulnerability [28]. This mechanistic insight underscores the potential benefits of periodontal interventions that may indirectly lower stroke risk by improving hypertension outcomes. Studies have indicated that periodontal therapy can lead to significant reductions in blood pressure, making it a vital consideration in managing patients with both periodontal disease and hypertension [29]. This bi‐directional relationship suggests that healthcare providers should integrate periodontal assessments and treatment into cardiovascular risk management protocols to mitigate both hypertension and stroke risk.
Our findings underscore the need for an interdisciplinary approach to cardiovascular health that includes dental and periodontal care. These results indicate that while periodontal disease may not independently be associated with stroke, the significant mediation through hypertension suggests that enhancing periodontal health could have important repercussions for managing hypertension and preventing cerebrovascular events [30]. Public health initiatives could focus on raising awareness of the links between periodontal health and hypertension, encouraging individuals to seek preventive dental care as part of comprehensive cardiovascular health strategies [31]. Targeting both conditions simultaneously may prove beneficial and warrants further research into integrative health models.
This study is not without limitations. The cross‐sectional design precludes any inference of causality, and the temporal sequences among periodontitis, hypertension, and stroke cannot be established. Therefore, we cannot rule out reverse causality; for instance, post‐stroke motor impairment or cognitive decline might lead to compromised oral hygiene and subsequent periodontitis. Crucially, while the mediation analysis statistically identified an indirect associative pathway through hypertension, the implied causal direction (periodontitis → hypertension → stroke) cannot be confirmed by the concurrent measurement of all variables. Therefore, the reported proportion mediated should be interpreted as a descriptive estimate of the associative structure under a specific statistical model, not as a measure of causal effect. Furthermore, the reliance on self‐reported stroke diagnoses may introduce misclassification bias; however, previous validations have demonstrated acceptable accuracy for such self‐reports. Additionally, despite thorough adjustment for potential confounding variables, residual confounding from unmeasured factors remains a possibility. The selection criteria, requiring at least one remaining tooth, may have resulted in the exclusion of individuals with more severe periodontal disease, affecting the generalizability of our findings.
5. Conclusion
In conclusion, our analysis of NHANES 2009–2014 data revealed no independent association between periodontitis and stroke after comprehensive adjustment for confounding factors. However, mediation analysis suggested a statistical pattern where hypertension accounted for a significant portion of the association between periodontitis and stroke history. While these findings suggest that periodontal health may interact with cardiovascular risk primarily through blood pressure regulation, the cross‐sectional design limits causal inference. Therefore, we strongly advocate for future prospective cohort studies to rigorously investigate their potential temporal sequences and causal relationships. Clinically, these results support an integrated approach where managing periodontal health is considered part of the broader strategy for hypertension control and stroke prevention.
Author Contributions
Shi-Yin Jin: conceptualization, methodology, investigation, formal analysis, writing. Qing Liu: investigation, data curation, resources, validation. Xiao-Qing Cao: methodology, investigation. Dian-Wei Wu: conceptualization, writing. Yun-Fan Cai: investigation, writing. Li-Na Niu: conceptualization, supervision. Wen Qin: conceptualization, methodology, formal analysis, supervision, project administration, funding acquisition, writing. Tao Ye: conceptualization, methodology, formal analysis, supervision, project administration, funding acquisition, writing. All authors contributed to the study conception and design.
Funding
This work was supported by the National Natural Science Foundation of China (Grants 82501152 and 82571121) and the Project of State Key Laboratory of Oral & Maxillofacial Reconstruction and Regeneration (Grant 2024QN02).
Disclosure
All authors read and approved the final manuscript.
Ethics Statement
The authors have nothing to report.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Papapanou P. N. , Sanz M. , and Buduneli N. , et al.Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions, Journal of Clinical Periodontology. (2018) 45, no. S 20, S 162–S 170, 10.1111/jcpe.12946, 2-s 2.0-85048803676.29926490 · doi ↗ · pubmed ↗
- 2Kassebaum N. J. , Bernabé E. , Dahiya M. , Bhandari B. , Murray C. J. L. , and Marcenes W. , Global Burden of Severe Periodontitis in 1990–2010, Journal of Dental Research. (2014) 93, no. 11, 1045–1053, 10.1177/0022034514552491, 2-s 2.0-84910049225.25261053 PMC 4293771 · doi ↗ · pubmed ↗
- 3Hajishengallis G. , Periodontitis: From Microbial Immune Subversion to Systemic Inflammation, Nature Reviews Immunology. (2015) 15, no. 1, 30–44, 10.1038/nri 3785, 2-s 2.0-84971323731.PMC 427605025534621 · doi ↗ · pubmed ↗
- 4The GBD 2016 Lifetime Risk of Stroke Collaborators , Feigin V. L. , and Nguyen G. , et al.Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016, New England Journal of Medicine. (2018) 379, no. 25, 2429–2437, 10.1056/NEJ Moa 1804492, 2-s 2.0-85058877243.30575491 PMC 6247346 · doi ↗ · pubmed ↗
- 5Benjamin E. J. , Muntner P. , and Alonso A. , et al.Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association, Circulation. (2019) 139, no. 10, e 56–e 528, 10.1161/CIR.0000000000000659, 2-s 2.0-85062154232.30700139 · doi ↗ · pubmed ↗
- 6Lockhart P. B. , Bolger A. F. , and Papapanou P. N. , et al.Periodontal Disease and Atherosclerotic Vascular Disease: Does the Evidence Support an Independent Association?, Circulation. (2012) 125, no. 20, 2520–2544, 10.1161/CIR.0b 013e 31825719 f 3, 2-s 2.0-84861336354.22514251 · doi ↗ · pubmed ↗
- 7Sanz M. , Marco Del Castillo A. , and Jepsen S. , et al.Periodontitis and Cardiovascular Diseases: Consensus Report, Journal of Clinical Periodontology. (2020) 47, no. 3, 268–288, 10.1111/jcpe.13189.32011025 PMC 7027895 · doi ↗ · pubmed ↗
- 8D’Aiuto F. , Parkar M. , and Andreou G. , et al.Periodontitis and Systemic Inflammation: Control of the Local Infection is Associated With a Reduction in Serum Inflammatory Markers, Journal of Dental Research. (2004) 83, no. 2, 156–160, 10.1177/154405910408300214, 2-s 2.0-3242773959.14742655 · doi ↗ · pubmed ↗