Spontaneous Transdiaphragmatic Intercostal Hernia in an Elderly Patient: A Rare Case Treated by Laparoscopic Repair
Jonathan Boukla, Maria Ruiz Patino, Martina Pezzullo, Patrizia Loi, Desislava Germanova

TL;DR
A rare case of a spontaneous transdiaphragmatic intercostal hernia in an elderly man was successfully treated with laparoscopic repair.
Contribution
This paper presents a rare spontaneous case of transdiaphragmatic intercostal hernia and demonstrates the effectiveness of laparoscopic repair.
Findings
A 71-year-old man with no trauma history developed a spontaneous transdiaphragmatic intercostal hernia.
Laparoscopic repair with mesh reinforcement led to uneventful recovery and no recurrence at 8 months.
Obesity and chronic immunosuppression were identified as contributing factors.
Abstract
Transdiaphragmatic intercostal hernia is a rare entity, with fewer than 50 cases reported in the literature. The majority are post-traumatic, secondary to blunt or penetrating thoracic injuries. Spontaneous forms are exceptional and often associated with risk factors such as obesity, chronic pulmonary disease, or long-term corticosteroid and immunosuppressive therapy. We present the case of a 71-year-old man with no history of trauma, who developed progressive dyspnea and subocclusive symptoms over several months. Imaging revealed a left transdiaphragmatic intercostal hernia between the seventh and eighth ribs, containing small bowel, colon, and omentum. The patient underwent laparoscopic repair with mesh reinforcement. Postoperative recovery was uneventful, with significant clinical improvement and no recurrence at eight-month follow-up. At that point, the patient reported localized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1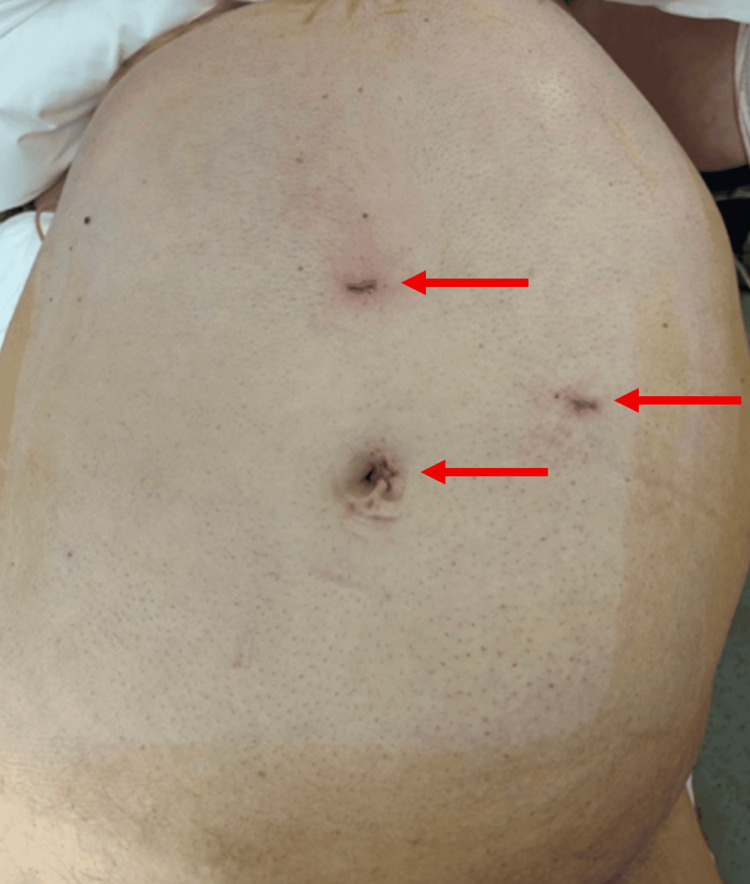 Figure 2
Figure 2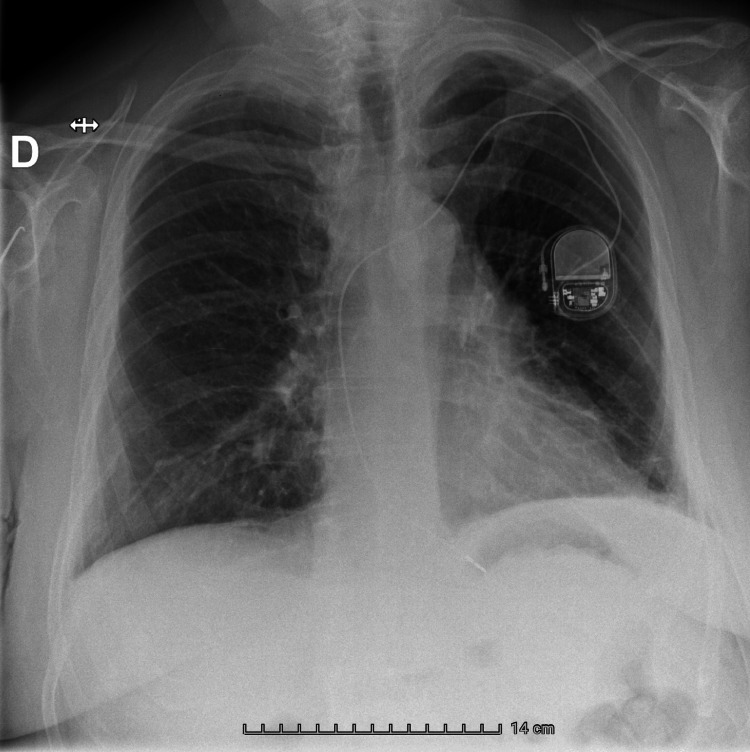 Figure 3
Figure 3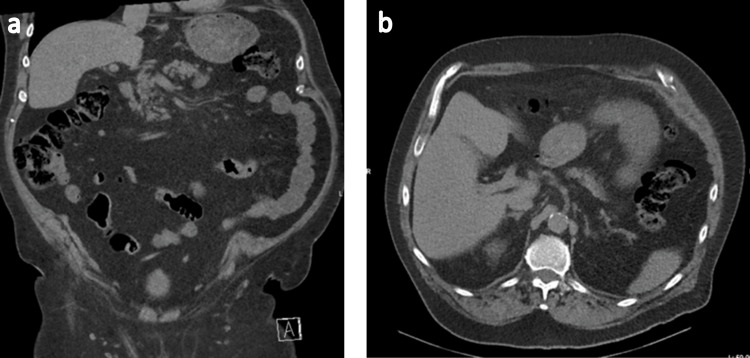 Figure 4
Figure 4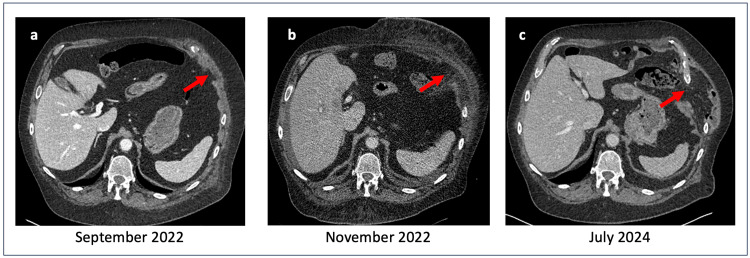 Figure 5
Figure 5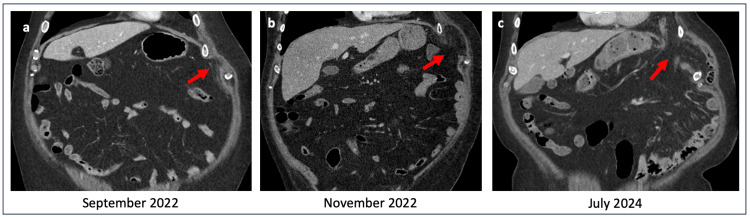 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Intestinal Malrotation and Obstruction Disorders · Stoma care and complications
Introduction
Transdiaphragmatic intercostal hernia is an exceptionally rare condition, with fewer than 50 cases reported in the literature to date [1,2]. Most reported cases are post-traumatic, occurring after high-energy blunt thoracic trauma such as road traffic accidents [1-3], or following penetrating thoracic injuries, including stab wounds and gunshot wounds [4,5]. In a smaller proportion of cases, underlying pulmonary pathology, particularly chronic obstructive pulmonary disease, has been identified as a contributing factor [6]. Spontaneous forms, occurring in the absence of trauma or obvious pulmonary disease, remain exceptional [7,8].
Spontaneous transdiaphragmatic intercostal hernias are clinically challenging, as symptoms are often progressive and non-specific, which may result in delayed diagnosis. Patients may present with respiratory complaints, chest or abdominal pain, or digestive symptoms, especially in the absence of a traumatic context.
Clinical presentation is variable, ranging from mild or progressive dyspnea to digestive symptoms related to herniation of abdominal viscera. Computed tomography is the imaging modality of choice, as it allows precise identification of the diaphragmatic and intercostal defect, characterization of hernia contents, and evaluation of associated thoracic or abdominal complications. CT imaging is also essential for surgical planning.
We report here the case of a 71-year-old man with no history of trauma, who developed a progressive transdiaphragmatic intercostal hernia. Predisposing factors included obesity and longstanding rheumatoid arthritis treated with chronic corticosteroid and immunosuppressive therapy. This case is notable for its atypical non-traumatic presentation and for its successful management using a laparoscopic approach, with a favorable outcome.
Case presentation
Patient presentation
A 71-year-old man was referred to surgical consultation for progressive dyspnea and intermittent subocclusive symptoms, which had begun approximately one year prior to diagnosis and had gradually worsened over time. The patient also reported associated abdominal pain and pyrosis of similar duration.
His past medical history included obesity (BMI 35.9), chronic renal failure, atrial fibrillation with a pacemaker, and longstanding rheumatoid arthritis treated with methylprednisolone and immunosuppressive therapy (methotrexate 25 mg/week and filgotinib 200 mg/day, later switched to sarilumab). He had required a prolonged intensive care unit stay in 2022 for respiratory failure secondary to infectious pneumonia. No history of thoracic or abdominal trauma was reported, and the patient denied any episodes of severe coughing, vomiting, or other Valsalva-type events preceding the onset of symptoms.
Diagnostic assessment
Upper gastrointestinal endoscopy revealed gastritis without evidence of Helicobacter pylori infection. A thoraco-abdominal computed tomography scan demonstrated a left intercostal transdiaphragmatic hernia between the seventh and eighth ribs, with an estimated defect size of 41 × 55 mm, containing small bowel, colon, and omentum. No hernia sac was identified (Figure 1). There were no radiological signs of bowel strangulation or ischemia, including bowel wall thickening, reduced enhancement, pneumatosis, or mesenteric congestion.
Left transdiaphragmatic intercostal hernia: preoperative thoracoabdominal CT scan imaging.a. Thoracic sagittal view b. Frontal thoracoabdominal view c. Abdominal sagittal view
Surgical management
A laparoscopic repair was performed under general anesthesia, with the patient in a supine position and legs apart. Pneumoperitoneum was established using a Veress needle at 12 mmHg. Three trocars were inserted: one 12-mm supra-umbilical port, one 5-mm epigastric port, and one 5-mm port in the left hypochondrium (Figure 2).
Port placement.A 12-mm supra-umbilical port, one 5-mm epigastric port, and one 5-mm port in the left hypochondrium
Exploration revealed a transdiaphragmatic intercostal hernia containing small bowel, colon, and omentum. Reduction was achieved easily, without adhesions. The abdominal cavity communicated directly with the thoracic cavity through the hernia defect, without interposition of a hernia sac. The thoracic cavity was free of adhesions.
After reduction, the intra-abdominal pressure was lowered to 8 mmHg, and the defect was closed using two hemi-continuous V-Lok sutures. Given the size of the defect (41 × 55 mm), a wide mesh overlap was deemed necessary, and a 15-cm circular Parietex™ (Medtronic, Minneapolis, USA) composite mesh was placed to ensure adequate coverage and reduce the risk of recurrence. Fixation was achieved using a combined technique, with lateral fixation using absorbable tackers (AbsorbaTack™ [Medtronic, Minneapolis, USA]) and medial fixation using interrupted 3-0 polypropylene sutures, in order to provide secure anchorage while limiting the risk of mesh displacement.
A pulmonary recruitment (Valsalva) maneuver was performed prior to definitive closure to minimize the risk of postoperative pneumothorax. Intraoperative thoracic surgical consultation was obtained, confirming that thoracic drainage was not required. The estimated operative time was 45 minutes, with no significant intraoperative blood loss.
Postoperative course
The postoperative course was uneventful. The patient reported mild parietal pain, which was adequately controlled with step I analgesics. Chest radiographs obtained on postoperative day (POD) 0 and POD 1 excluded pneumothorax (Figure 3). Early mobilization was initiated on POD 1, and the patient was discharged on POD 1 with oral analgesics and instructions to avoid heavy lifting (>3-4 kg).
Control chest X-ray on postoperative day one.
At the one-month follow-up, a control CT scan showed no evidence of recurrence, and the patient reported marked improvement in both respiratory and digestive symptoms.
At the eight-month follow-up, the patient was reviewed in outpatient consultation. He reported localized exertional parietal pain in the area corresponding to the previous hernia site, described as intermittent “electric discharges,” without associated dyspnea or digestive symptoms. A repeat CT scan confirmed the absence of recurrence (Figure 4). Neuropathic pain related to intercostal nerve involvement was suspected. Referral to a pain management clinic was proposed; however, the patient ultimately declined further evaluation, as symptoms were considered tolerable. No specific neuropathic pharmacological treatment was initiated.
Control CT scan eight months after surgery.No recurrence was observed in frontal view (a) nor in sagittal view (b).
Discussion
Transdiaphragmatic intercostal hernia is a very uncommon condition, with fewer than 50 cases reported in the literature [2]. The majority of reported cases are post-traumatic, following high-velocity blunt trauma or penetrating injury [2-5]. Other etiologies include underlying pulmonary pathology, notably chronic obstructive pulmonary disease, in which repeated increases in intrathoracic pressure may contribute to progressive weakening of the diaphragm and intercostal spaces [6]. Rare spontaneous cases have also been described [7,8]. In our patient, no traumatic event was identified. Two risk factors likely contributed. Obesity is known to increase intra-abdominal pressure and has been associated with the development of abdominal wall hernias [9]. In addition, longstanding rheumatoid arthritis treated with chronic corticosteroid and immunosuppressive therapy may predispose to progressive muscular and tissue fragility, potentially affecting diaphragmatic and intercostal structures [10]. Although the exact pathophysiological mechanisms remain incompletely understood, this combination of increased mechanical stress and reduced tissue resistance may facilitate hernia formation in the absence of trauma.
The natural history of transdiaphragmatic intercostal hernias may be acute or progressive, with some cases developing over several years [11]. In this patient, CT imaging from 2022 had already demonstrated early signs of an intercostal hernia associated with local inflammatory changes. Over time, the hernia progressed through the diaphragm, supporting a gradual evolution rather than an acute rupture (Figures 5, 6). Negative intrathoracic pressure during respiration has been proposed as a contributing factor to the progressive enlargement of diaphragmatic defects [12]. However, due to the rarity of this condition, it remains unclear whether negative intrathoracic pressure, increased intra-abdominal pressure, or a combination of both plays the predominant role in hernia formation.
Sagittal view of thoracoabdominal CT scan showing the evolution of the left transdiaphragmatic intercostal hernia over time.
Frontal view of thoracoabdominal CT scan evolution of the left transdiaphragmatic intercostal hernia over time.
Surgical repair remains the only curative treatment [13,14]. Both open approaches (thoracotomy or laparotomy) and minimally invasive techniques have been described. In selected cases, laparoscopy may be preferable to thoracotomy, as it allows excellent visualization of the diaphragmatic defect, facilitates safe reduction of abdominal viscera, and enables mesh reinforcement with reduced postoperative pain and faster recovery. These advantages may be particularly relevant in elderly or comorbid patients [2]. For large defects, prosthetic reinforcement with mesh is recommended to reduce the risk of recurrence [4,15]. In our case, primary closure was performed using V-Lok sutures and reinforced with a Parietex™ mesh. No thoracic drain was required, as no pneumothorax occurred, consistent with previous reports [15].
The optimal method of mesh fixation remains debated. In our patient, lateral fixation was achieved using tackers and medial fixation with interrupted sutures, providing secure fixation without displacement or recurrence. This approach differs from reports suggesting a potential risk of mesh migration when tackers alone are used [4].
Another interesting feature in this case was the absence of a hernia sac. This situation is more frequently described in acute or traumatic hernias, whereas progressive or congenital hernias generally involve a sac enclosing the herniated viscera [16]. In our patient, imaging from 2022 suggested a progressive mechanism, but the absence of a sac at surgery may indicate a superimposed acute event. The current literature does not clearly distinguish outcomes between patients with or without a sac, as this feature is inconsistently reported.
Most common early postoperative complications include pulmonary complications (pneumothorax, hemothorax, pulmonary infection), abdominal complications (ileus, bowel obstruction), and, as a late complication, recurrence and complications related to the mesh (migration, erosion, infection) [2,3].
Conclusions
Spontaneous transdiaphragmatic intercostal hernia is an exceptionally rare entity, with fewer than 50 cases reported in the literature. In this patient, the hernia developed progressively over several years without any history of trauma, illustrating that non-traumatic etiologies can occur. This case highlights the need to maintain a high index of suspicion in obese or immunosuppressed patients presenting with atypical and progressive thoracoabdominal symptoms, even in the absence of trauma. Early diagnosis and timely laparoscopic repair with mesh reinforcement can lead to favorable short- and mid-term outcomes, with a low risk of recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Post-traumatic transdiaphragmatic intercostal hernia: report of two cases Surg Today Benizri EI Delotte J Severac M 96994320132261050910.1007/s 00595-012-0197-6 · doi ↗ · pubmed ↗
- 2Transdiaphragmatic intercostal hernia-an unusual hepatic injury after a car accident: a case report and review of the literature Discoveries (Craiova) Ioannidis O Mariorakis C Malliora A 09202110.15190/d.2021.2PMC 816348834084890 · doi ↗ · pubmed ↗
- 3Strangulated intercostal liver herniation subsequent to blunt trauma. First report with review of the world literature World J Emerg Surg Bendinelli C Martin A Nebauer SD Balogh ZJ 23720122280029310.1186/1749-7922-7-23PMC 3441203 · doi ↗ · pubmed ↗
- 4Laparoscopic repair of recurrent traumatic diaphragmatic hernia J Minim Access Surg Singh D Aggarwal S Vyas S 1661681620203103131610.4103/jmas.JMAS_298_18PMC 7176003 · doi ↗ · pubmed ↗
- 5Transdiaphragmatic intercostal hernia following a penetrating thoracoabdominal injury: report of a case Surg Today Balkan ME Kara M Oktar GL UnlüE 7087113120011151060810.1007/s 005950170075 · doi ↗ · pubmed ↗
- 6Transdiaphragmatic intercostal hernia: imaging aspects in three cases J Bras Pneumol Macedo AC Kay FU Terra RM 5135173920132406827410.1590/S 1806-37132013000400016 PMC 4075857 · doi ↗ · pubmed ↗
- 7An enigma of spontaneous combined transdiaphragmatic, intercostal and abdominal wall hernia Hernia Abu-Gazala M Ratnayake A Abu-Gazala S Bala M 4154181720132235436010.1007/s 10029-012-0902-9 · doi ↗ · pubmed ↗
- 8Gastric volvulus and tension gastrothorax secondary to spontaneous transdiaphragmatic intercostal hernia BMJ Case Rep Bennet S Wang M Spiro C Tog C 15202210.1136/bcr-2021-246832 PMC 876887335039367 · doi ↗ · pubmed ↗