A Case of Extensive Maxillary Medication‐Related Osteonecrosis of the Jaw With Wound Closure Using a Pedicled Buccal Fat Pad
Ryohei Iwasaki, Karen Gomi, Yusuke Kurosawa, Akinori Moroi, Kunio Yoshizawa, Koichiro Ueki

TL;DR
This paper presents a rare case of severe jaw bone death treated with a fat pad technique instead of traditional reconstruction.
Contribution
The novel approach uses a pedicled buccal fat pad for wound closure in extensive MRONJ without jaw reconstruction.
Findings
Aggressive resection of infected bone is crucial to prevent infection spread into the maxillary sinus.
A pedicled buccal fat pad successfully closed the wound and improved oral function without reconstruction.
This method offers an alternative for managing extensive MRONJ bone defects.
Abstract
Reports of extensive medication‐related osteonecrosis of the jaw (MRONJ) with pedicled buccal fat pad wound closure without tissue reconstruction are rare. We present the case of a 78‐year‐old man with prostate cancer and extensive MRONJ on the left side of the maxilla. The patient was treated with denosumab for the multiple bone marrow and lymph node metastases. Aggressive resection of the infected bone should be considered to prevent the spread of the infection if it extends into the maxillary sinus. In cases of extensive removal of decayed bone, jaw reconstruction is necessary to address the bone defect because it impairs the ability to eat, speak, and communicate. However, it was possible to close the wound and improve oral function by using a pedicled buccal fat pad for extensive MRONJ without maxillary reconstruction.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1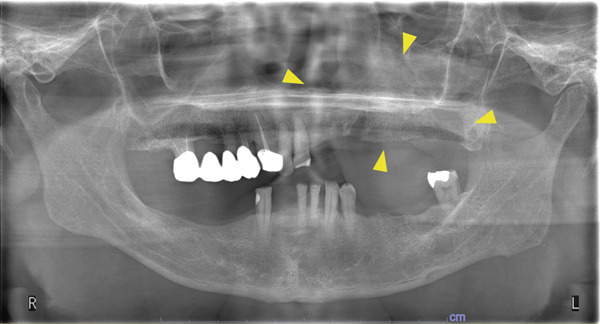 Figure 2
Figure 2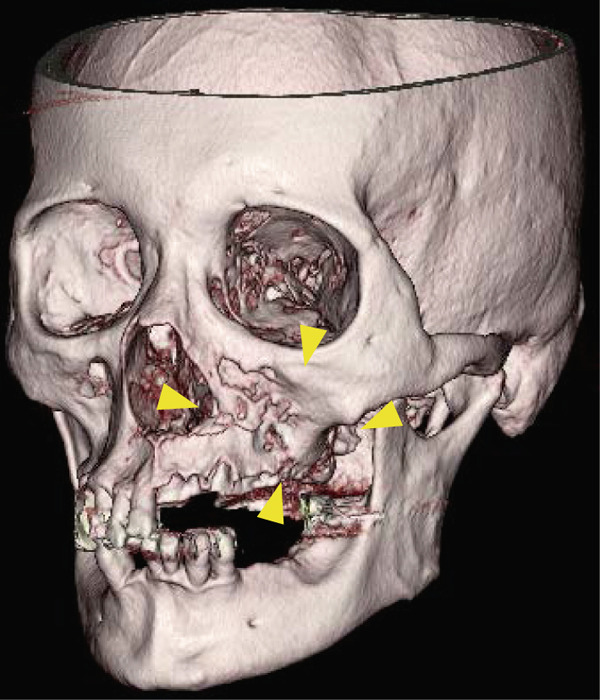 Figure 3
Figure 3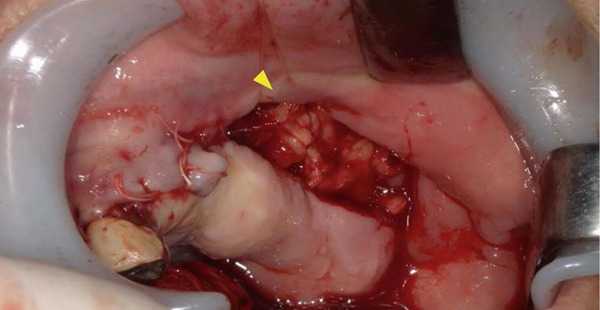 Figure 4
Figure 4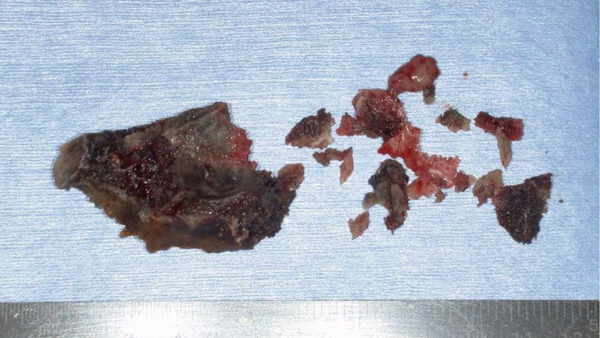 Figure 5
Figure 5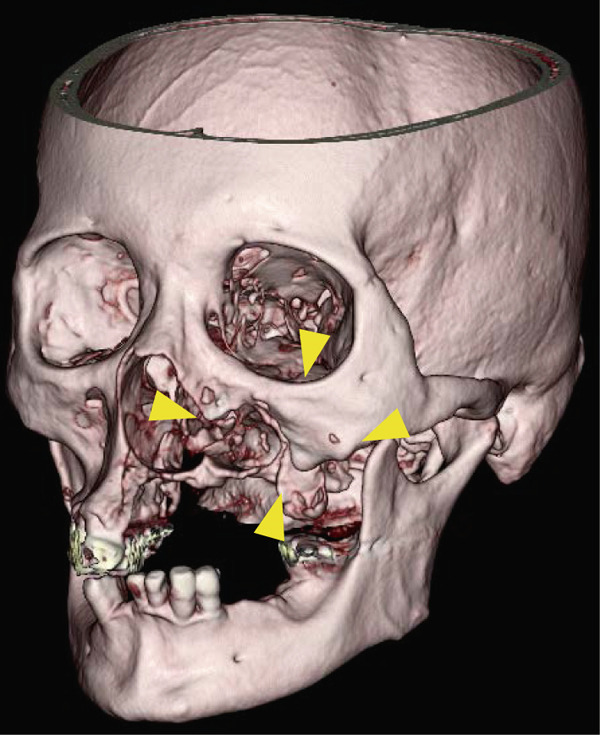 Figure 6
Figure 6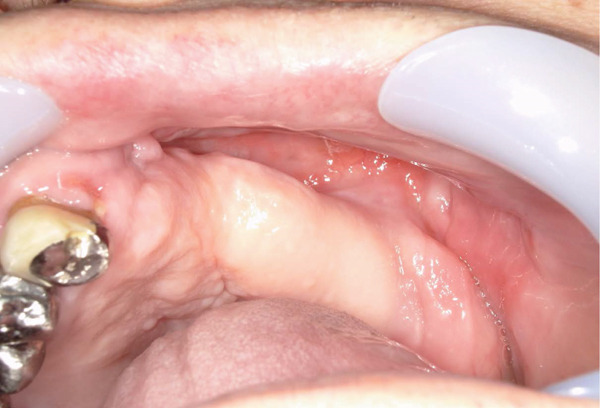 Figure 7
Figure 7 Figure 8
Figure 8|
|
|
|
|
| |
|---|---|---|---|---|---|
| André Ferreira Leite (2006) [ | Male | 82 | Zolendronic acid | 34 × 14 | Primary closure with intranasal |
| Jan Rustemeyer (2014) [ | Male | 44 | Methamphetamine | Undocumented | Primary closure with intranasal |
| Yoshinari Myoken (2022) [ | Female | 64 | Alendronic acid | 30 × 50 | Buccal fat pad flap |
| Andreas Sakkas (2021) [ | Female | 45 | Tocilizumab | Undocumented | Primary closure with intranasal |
| Panagiotis Koulocheris (2008) [ | Male | 49 | Zolendronic acid | 48 × 20 | Primary closure with intranasal |
| Luiz Fernando Mathias Duart (2015) [ | Female | 58 | Zolendronic acid | Undocumented | Buccal fat pad flap |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Rejuvenation and Surgery Techniques · Temporomandibular Joint Disorders · Oral health in cancer treatment
1. Introduction
Medication‐related osteonecrosis of the jaw (MRONJ) can be triggered by several antiresorptive and antiangiogenic medications, including bisphosphonates (BRONJ), denosumab (DRONJ), and other medications used to treat osteoporosis and metastatic bone cancer [1]. Henien et al. [2] reported that osteonecrosis of the jaw, which is not a lymphoproliferative disease, occurs in patients receiving long‐term methotrexate therapy without concomitant use of bone resorption inhibitors or angiogenesis inhibitors. In the present case, denosumab was administered for a long period, and it was thought that this drug may have been involved in the development of MRONJ. In recent years, reports of MRONJ in patients treated for cancer or osteoporosis have emerged [3]. MRONJ is caused by bone exposure resulting from treatment that is invasive to the jawbone at the site and so on. Mandibles have thicker cortical bone and sparser blood flow than the maxilla, which is why MRONJ occurs more frequently in the mandible. Therefore, MRONJ has been reported less frequently in the maxilla, and more extensive cases are rare [4].
When MRONJ was first named in 2003, conservative treatment was the preferred option, and aggressive surgical intervention was not recommended. However, in recent years, reports of successful surgical treatment have increased [5]. Nevertheless, there is no established method for determining the extent of bone removal and wound treatment. Even if a patient is cured through surgery, significant deterioration of oral function can be expected if extensive jaw resection is performed. Tissue reconstruction is required when extensive jaw resection is necessary. In this report, we present a case in which a wound was closed using buccal fat.
2. Case Presentation
A 78‐year‐old man presented to the Department of Oral and Maxillofacial Surgery, University of Yamanashi Hospital, complaining of bone exposure in the left maxilla. He had a history of bone metastasis from prostate cancer for more than 4 years and was receiving denosumab subcutaneous injection at 120 mg/1.7 ml. His medical history included diabetes mellitus, hypertension, angina pectoris, and dyslipidemia, and he was allergic to atenolol, cephem, and penicillin. The face was symmetrical, and drainage occurred from the exposed left maxilla. The local lymph nodes were normal, and there was no trismus. An intraoral examination revealed gingival swelling, erythema, and purulent discharge (Figure 1). Panoramic radiography revealed extensive necrotic bone fragments in the left maxilla (Figure 2). Computed tomography (CT) revealed bone sclerosis extending from the right maxillary lateral incisor region to the left maxillary premolar region, anterior nasal floor, and left maxillary palatal region, along with necrotic bone from the left maxillary anterior region to the molar region, indicating maxillary osteonecrosis and sinusitis (Figure 3). The administration and cleaning of the exposed bone with povidone‐iodine did not relieve the symptoms, and the patient underwent left maxillectomy under general anesthesia with drainage of the maxillary sinus. The buccal fat pad was bluntly dissected from the full‐layer valve, and the defect was covered with the left buccal fat pad and tied over with a Terramamycin ointment gauze (Figures 4 and 5).
Intraoral photographs at initial examination.
Panoramic image at initial examination.
Preoperative 3DCT images.
Intraoral images during the necrotic bone removal.
Surgically removed the necrotic bone.
The patient′s 10‐day postoperative course was uneventful, and he was discharged from the hospital. Subsequent CT revealed no residual necrotic bone (Figure 6). The wound epithelialized 1 month after surgery. After epithelialization, the prefabricated prosthesis was immediately fitted. 3 months after the surgery, no maxillary sinus fistulas were observed. The oral cavity was in good condition (Figure 7). There were no problems with the fit of the maxillary denture to the bone defect, and the patient had good occlusion (Figure 8).
Postoperative 3DCT images.
Intraoral image after the necrotic bone removal.
Maxilla denture for bone defects after removal of the necrotic bone.
3. Discussion
In 2003, Marx described the first case of osteonecrosis of the jaw after bisphosphonate treatment, which manifested as painful bone exposure of the jaw that was unresponsive to medical and surgical therapies [6]. He attributed it to the use of bisphosphonates such as pamidronate and zoledronate, prescribed to patients. The diagnosis of MRONJ is defined by the American Association of Oral and Maxillofacial Surgeons (AAOMS) [7], and our understanding of this disease has advanced significantly over the past decade. Antiresorptive drugs, including bisphosphonates and denosumab, are increasingly associated with this condition. Angiogenesis inhibitors, certain anticancer agents, tyrosine kinase inhibitors (TKIs), mammalian targets of rapamycin inhibitors, and immunotherapeutic agents have also been implicated in MRONJ [8]. The pathogenesis of MRONJ is not well understood [9]; however, the inhibition of bone resorption and alterations in bone remodeling are thought to play significant roles in the pathogenesis of MRONJ. The rapid rate of alveolar bone remodeling contributes to the high incidence of MRONJ in the jaw. The presence of inflammation of the periodontal ligament and the functional loading of the alveolar bone by dentition further increase the demand for bone remodeling in the alveolar bone, thus heightening dependence on osteoclast‐mediated bone resorption and remodeling. Periodontal infection, tooth extraction, and ill‐fitting dentures can also precipitate MRONJ [10].
In the present case, the patient had been using denosumab for more than 4 years, which suppressed bone metabolism. Risk factors such as periodontal infection and tooth extraction may have further increased the need for bone remodeling, leading to the development of MRONJ.
Various medical and surgical treatments have been attempted to manage MRONJ. Traditionally, the management of MRONJ has been aimed at controlling infection and preventing further progression of necrosis [11]. In the early stages, such as when there is no clinical evidence of necrotic bone but nonspecific clinical findings, radiographic changes, and symptoms (Stage 0), or when there is exposed and necrotic bone or fistulae that probe to the bone in asymptomatic patients with no evidence of infection (Stage 1), conservative treatment is most advocated. Various local and systemic antimicrobial agents, such as pentoxifylline, vitamin E, hyperbaric oxygen therapy, and teriparatide, have been used with inconsistent results [12]. Surgical treatment is often reserved for patients with advanced stages that are refractory to medical therapy. Excision, debridement, and coverage of surgical defects using vascular flaps are the most commonly performed surgical procedures. Complete coverage of the exposed bone is essential to prevent disease recurrence and progression [13].
Preoperative CT images revealed that the inflammation in this case involved the mucosa of the left maxillary sinus floor and extended from the left maxillary dentition across the center to the right maxillary canine. Compared with previous cases (Table 1), the degree of bone collapse was relatively extensive, and conservative treatment was judged to be difficult owing to the expected expansion of the lesion in the future; thus, the decision was made to proceed with surgical treatment. In the present case, because the gingival mucosa was preserved as much as possible, we decided to use a buccal fat body with a pedicle for wound closure.
Because recent studies have shown that subcutaneous adipose tissue differentiates into multiple lineages and expresses multiple growth factors, a buccal fat pad (BFP) was performed [19]. Mucosal healing is impaired in MRONJ. This is predominantly because of the soft tissue effects of these drugs. These medications have also been associated with decreased proliferation and induction of apoptosis in keratinocytes and fibroblasts, resulting in impaired healing and wound differentiation. Furthermore, the poor vascularity of the mucosal flap can also be attributed to poor wound healing. Therefore, the chances of wound dehiscence and impaired wound healing are relatively high when only a mucosal flap is used for coverage.
There are a few reports of extensive MRONJ of the maxilla, most of which involved reconstructive surgeries (Table 1). Some cases ranged in size from 31 × 14 mm to 30 × 50 mm. In the present case, the rotator bone was 63 × 24 mm in size, and there were no cases of MRONJs in this size range that were closed using only layer BFP without tissue reconstruction. In this case, a maxillary denture was created for the bone defect to restore oral function. After surgical treatment, occlusal reconstruction is essential for improving the patient′s quality of life. Functional reconstruction with normal dentures is often difficult with occlusal reconstruction, and continuous follow‐up is essential.
In conclusion, determining whether tissue reconstruction is necessary for extensive MRONJ is difficult. However, buccal fat bodies may be an option for postoperative occlusal recovery.
Funding
No funding was received for this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ali I. E. and Sumita Y. , Medication-Related Osteonecrosis of the Jaw: Prosthodontic Considerations, Japanese Dental Science Review. (2022) 58, 9–12, 10.1016/j.jdsr.2021.11.005, 34984072.34984072 PMC 8693001 · doi ↗ · pubmed ↗
- 2Henien M. , Carey B. , Hullah E. , Sproat C. , and Patel V. , Methotrexate-Associated Osteonecrosis of the Jaw: A Report of Two Cases, Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology. (2017) 124, no. 6, e 283–e 287, 10.1016/j.oooo.2017.09.005, 2-s 2.0-85031827587, 29056286.29056286 · doi ↗ · pubmed ↗
- 3Mauceri R. , Coppini M. , Attanasio M. , Bedogni A. , Bettini G. , Fusco V. , Giudice A. , Graziani F. , Marcianò A. , Nisi M. , and Isola G. , MRONJ in Breast Cancer Patients Under Bone Modifying Agents for Cancer Treatment-Induced Bone Loss (CTIBL): A Multi-Hospital-Based Case Series, BMC Oral Health. (2023) 23, no. 1, 10.1186/s 12903-023-02732-6, 36739399.PMC 989937536739399 · doi ↗ · pubmed ↗
- 4Leite A. F. , Figueiredo P. T. , Melo N. S. , Acevedo A. C. , Cavalcanti M. G. , Paula L. M. , Paula A. P. , and Guerra E. N. , Bisphosphonate-Associated Osteonecrosis of the Jaws. Report of a Case and Literature Review, Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. (2006) 102, no. 1, 14–21, 10.1016/j.tripleo.2005.10.045, 2-s 2.0-33745752665.16831667 · doi ↗ · pubmed ↗
- 5Goker F. , Grecchi E. , Grecchi F. , Francetti L. , and Del Fabbro M. , Treatment of Medication-Related Osteonecrosis of the Jaw (MRONJ). A Systematic Review, European Review for Medical & Pharmacological Sciences. (2021) 25, no. 6, 2662–2673, 10.26355/eurrev_202103_25430, 33829453.33829453 · doi ↗ · pubmed ↗
- 6Marx R. E. , Pamidronate (Aredia) and Zoledronate (Zometa) Induced Avascular Necrosis of the Jaws: A Growing Epidemic, Journal of Oral and Maxillofacial Surgery. (2003) 61, no. 9, 1115–1117, 10.1016/S 0278-2391(03)00720-1, 2-s 2.0-0042861578, 12966493.12966493 · doi ↗ · pubmed ↗
- 7Ruggiero S. L. , Dodson T. B. , Fantasia J. , Goodday R. , Aghaloo T. , Mehrotra B. , and O′Ryan F. , American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw—2014 Update, Journal of Oral and Maxillofacial Surgery. (2014) 72, no. 10, 1938–1956, 10.1016/j.joms.2014.04.031, 2-s 2.0-84909619222, 25234529.25234529 · doi ↗ · pubmed ↗
- 8King R. , Zebic L. , and Patel V. , Deciphering Novel Chemotherapy and Its Impact on Dentistry, British Dental Journal. (2020) 228, no. 6, 415–421, 10.1038/s 41415-020-1365-5, 32221440.32221440 · doi ↗ · pubmed ↗