Serum Aspergillus Immunoglobulin G as an Independent Biomarker for Extrasinonasal Involvement in Chronic Invasive Aspergillus Rhinosinusitis
Jun-Tian Huang, Ling-Hong Zhou, Wen-Jia Qiu, Hui Tang, Rong-Sheng Zhu, Ying-Kui Jiang, Hua-Zhen Zhao, Zhong-Qing Chen, Li-Ping Zhu

TL;DR
This study shows that Aspergillus IgG antibodies in the blood can predict if a fungal sinus infection has spread beyond the sinuses and how well patients respond to treatment.
Contribution
The study identifies serum Aspergillus IgG as a novel noninvasive biomarker for predicting extrasinonasal involvement and monitoring treatment in chronic invasive fungal rhinosinusitis.
Findings
Seropositivity for Aspergillus IgG was significantly higher in patients with extrasinonasal involvement (59.2%) compared to those without (8.9%).
Aspergillus IgG antibodies were an independent predictor of extrasinonasal involvement with an odds ratio of 11.28.
Antibody levels decreased significantly in patients achieving radiological and clinical remission after antifungal therapy.
Abstract
To investigate the seroprevalence of Aspergillus IgG antibodies among patients with chronic invasive Aspergillus rhinosinusitis (CIARS) and to assess their prognostic value for extrasinonasal involvement and therapeutic outcomes. A total of 132 patients with histopathologically confirmed CIARS were included. Serum Aspergillus IgG antibody levels were measured by enzyme-linked immunosorbent assay. Univariate and multivariable analyses were conducted to identify independent predictors of extrasinonasal involvement. To evaluate the prognostic value of antibody monitoring, serial Aspergillus IgG levels were assessed, and their association with radiological remission was analyzed. Among the 132 patients, 50 (37.9%) tested positive for Aspergillus IgG antibodies. Seropositivity was significantly higher among patients with extrasinonasal involvement than among those without such involvement…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
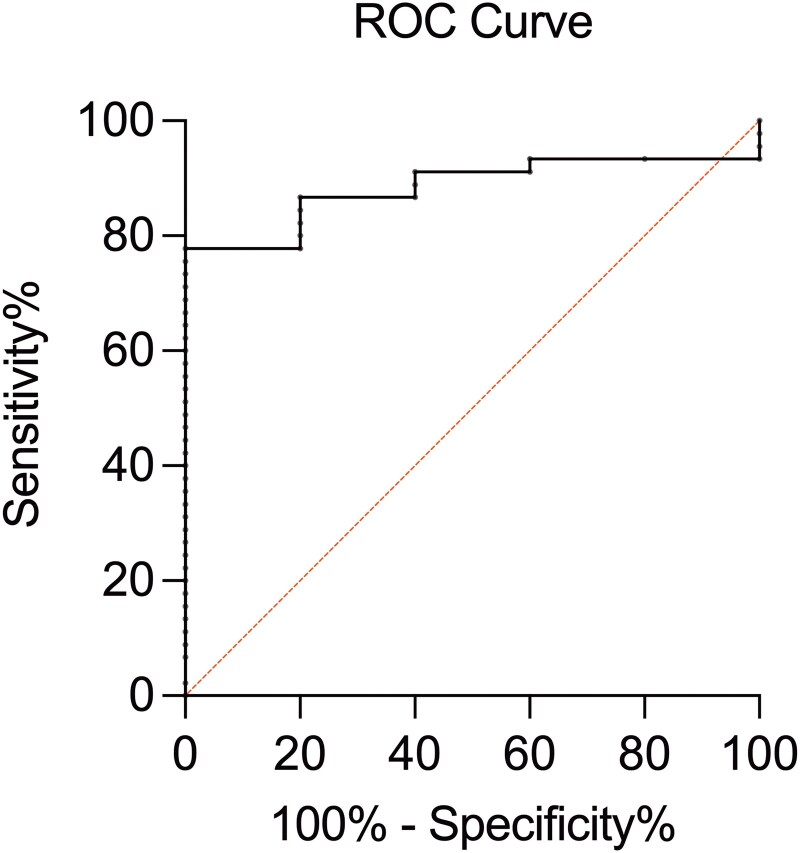 Figure 1
Figure 1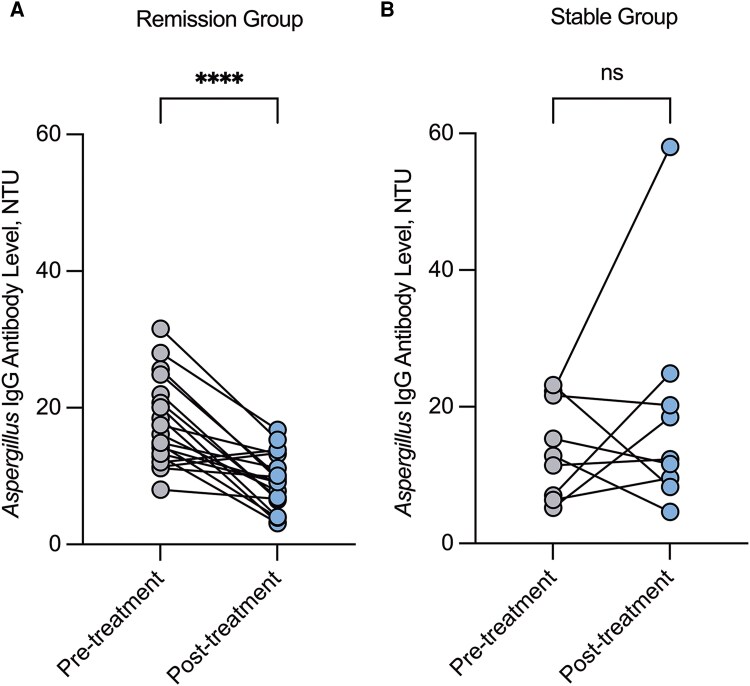 Figure 2
Figure 2| Variable | CIARS Cases (n = 132) | |
|---|---|---|
| Male, n (%) | 56 | (42.4) |
| Age(y), median (IQR) | 56 | (49–66) |
| Predisposing factors, n (%) | 55 | (41.7) |
| Diabetes mellitus | 35 | (26.5) |
| Glucocorticosteroids | 17 | (12.9) |
| Chronic kidney disease | 13 | (9.8) |
| Autoimmune diseases | 11 | (8.3) |
| Radiotherapy or chemotherapy | 8 | (6.1) |
| Solid malignancy | 7 | (5.3) |
| Trauma or destruction of facial structures | 5 | (3.8) |
| Hematologic malignancy | 4 | (3.0) |
| Liver cirrhosis | 2 | (1.5) |
| Paranasal sinuses involvement, n (%) | ||
| Maxillary sinus | 109 | (82.6) |
| Ethmoid sinus | 108 | (81.8) |
| Sphenoid sinus | 71 | (53.8) |
| Frontal sinus | 31 | (23.5) |
| Extrasinonasal involvement, n (%) | 76 | (57.6) |
| Orbit | 53 | (40.2) |
| Cranial | 29 | (22.0) |
| Cavernous sinus | 26 | (19.7) |
| Mastoid | 19 | (14.4) |
| Pterygopalatine fossa | 11 | (8.3) |
| Pituitary fossa | 8 | (6.1) |
| Variable | CIARS Cases With Orbital Apex Syndrome (n = 32) | |
|---|---|---|
| Manifestations at baseline, n (%) | ||
| Visual impairment | 32 | (100.0) |
| Blindness | 23 | (71.9) |
| Unilateral | 19 | (59.4) |
| Bilateral | 4 | (12.5) |
| Impaired eye movement | 29 | (90.6) |
| Ptosis | 28 | (87.5) |
| Periorbital pain | 26 | (81.3) |
| Proptosis | 20 | (62.5) |
| Epiphora | 3 | (9.4) |
| Paranasal sinuses involvement, n (%) | ||
| Ethmoid sinus | 30 | (93.8) |
| Sphenoid sinus | 25 | (78.1) |
| Maxillary sinus | 24 | (75.0) |
| Frontal sinus | 7 | (21.9) |
| Variable | CIARS Cases With Cranial Involvement (n = 29) | |
|---|---|---|
| Paranasal sinuses involvement, n (%) | ||
| Ethmoid sinus | 28 | (96.6) |
| Maxillary sinus | 24 | (82.8) |
| Sphenoid sinus | 22 | (75.9) |
| Frontal sinus | 9 | (31.0) |
| Intracranial sites involvement, n (%) | ||
| Temporal lobe | 18 | (62.1) |
| Frontal lobe | 15 | (51.7) |
| Occipital lobe | 2 | (6.9) |
| Hypophysis | 2 | (6.9) |
| Cerebral falx | 2 | (6.9) |
| Cerebellum | 2 | (6.9) |
| Single intracranial site involvement, n (%) | 19 | (65.5) |
| Multiple intracranial site involvement, n (%) | 10 | (34.5) |
| Variable | Univariate Analysis | Multivariable Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CIARS Cases with Extrasinonasal Involvement (n = 76) | CIARS Cases without Extrasinonasal Involvement (n = 56) |
| OR | (95% CI) |
| |||||
| Male, n (%) | 39 | (51.3) | 17 | (30.4) | .017 | 2.48 | (.96–6.40) | .060 | ||
| Age(y), median (IQR) | 57 | (51–68) | 56 | (48–62) | .246 | |||||
| Predisposing factors, n (%) | 36 | (47.4) | 19 | (33.9) | .123 | |||||
| Diabetes mellitus | 24 | (31.6) | 11 | (19.6) | .128 | |||||
| Glucocorticosteroids/immunosuppressants | 12 | (15.8) | 5 | (8.9) | .251 | |||||
| Autoimmune diseases | 9 | (11.8) | 2 | (3.6) | .109 | |||||
| Trauma or destruction of facial structures | 2 | (2.6) | 3 | (5.4) | .427 | |||||
| Chronic kidney disease | 9 | (12.8) | 4 | (7.1) | .375 | |||||
| Malignancy | 4 | (5.3) | 3 | (5.4) | .981 | |||||
| Paranasal sinuses involvement, n (%) | ||||||||||
| Sphenoid sinus | 54 | (71.1) | 17 | (30.4) | <.001 | 4.72 | (1.89–11.79) | <.001 | ||
| Ethmoid sinus | 69 | (90.8) | 39 | (69.6) | .003 | 5.22 | (1.53–17.86) | .008 | ||
| Maxillary sinus | 60 | (78.9) | 49 | (87.5) | .205 | |||||
| Frontal sinus | 22 | (28.9) | 9 | (16.1) | .088 | |||||
| Time from diagnosis to antifungal treatment > 3 m, n (%) | 25 | (32.9) | 10 | (17.9) | .056 | |||||
| Positive serum | 45 | (59.2) | 5 | (8.9) | <.001 | 11.28 | (3.67–34.64) | <.001 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSinusitis and nasal conditions · IgG4-Related and Inflammatory Diseases · Autoimmune Bullous Skin Diseases
Chronic invasive Aspergillus rhinosinusitis (CIARS) is a progressive, life-threatening fungal infection characterized by hyphal invasion of the sinonasal mucosa with extension into adjacent bony or neurovascular structures [1]. CIARS typically presents with nonspecific symptoms, including nasal obstruction, facial pain, and neuro-ophthalmic disturbances. The insidious nature of disease progression, combined with these vague clinical manifestations, often results in diagnostic delay, with a median time to diagnosis exceeding 6 months (range, 4–24 months) [2]. The protracted course of CIARS allows fungal invasion to progress over months to years, ultimately breaching bony barriers and involving extrasinonasal structures [3]. Extrasinonasal involvement is a critical determinant of prognosis in invasive fungal sinusitis (IFS): orbital invasion might precipitate vision-threatening orbital apex syndrome, whereas intracranial dissemination could result in life-threatening cranial neuropathies [4]. Reported mortality rates increase stepwise with anatomical progression, reaching ∼33% with orbital involvement, 50% with skull base invasion, and nearly 100% with cerebral dissemination [5]. Therefore, early diagnosis is critical to prevent irreversible tissue damage and reduce mortality. Current management strategies rely on endoscopic surgical debridement combined with systemic antifungal therapy, typically administered for 6–12 weeks postoperatively [6]. However, therapeutic success largely depends on identifying the disease before irreversible extrasinonasal extension occurs. Consequently, identifying validated predictors of extrasinonasal invasion is essential for effective risk stratification and timely intervention.
CIARS diagnosis currently requires histopathological confirmation of fungal invasion in conjunction with radiographic evidence of bony or soft tissue destruction. Although definitive, these approaches are invasive, labor intensive, and poorly suited for early diagnosis or longitudinal disease monitoring. Serum biomarkers, such as the (1,3)-β-D-glucan (BDG) and galactomannan (GM) assays, are widely used for diagnosing systemic fungal infections; however, their clinical utility in CIARS remains limited. Recent clinical investigations have demonstrated suboptimal diagnostic performance for both assays, with positivity rates of 13.6% for the BDG test and 9.1% for the GM test [7]. These findings underscore the need for more specific, noninvasive biomarkers for CIARS.
Aspergillus immunoglobulin G (IgG) antibodies serve as a validated diagnostic biomarker for chronic pulmonary aspergillosis (CPA), demonstrating a specificity of 89.6% (95% confidence interval [CI]: 86.2–92.3) and a positive predictive value of 100% [8, 9]. Given its high specificity in CPA diagnosis, Aspergillus IgG antibodies might serve as a reliable biomarker for CIARS, particularly when interpreted in conjunction with clinical and radiological findings. In this cohort study, we analyzed 132 histopathologically confirmed cases of CIARS to assess the utility of serum Aspergillus IgG antibodies for risk stratification and prognostic evaluation. Specifically, we aimed to investigate their role in identifying high-risk patients and to evaluate their potential as tools for early detection and monitoring of treatment response.
METHODS
Participants and Procedures
This retrospective cohort study was conducted at Huashan Hospital, a national medical center for infectious diseases in Shanghai, China, between January 2017 and June 2025. Adult patients (≥18 years) with histopathologically confirmed CIARS during this period were consecutively included. A confirmed CIARS diagnosis was established based on the following criteria: (1) disease duration exceeding 12 weeks and (2) histopathological evidence of tissue invasion by fungal hyphae consistent with Aspergillus species, characterized by dense hyphal aggregates, sparse inflammatory responses, and occasional vascular invasion [10–12]. All pathology specimens were confirmed by an experienced pathologist using standardized diagnostic criteria. Exclusion criteria included acute disease onset (less than 4 weeks) and incomplete clinical data. A total of 132 patients met the inclusion criteria. Patient data were extracted from medical records and included demographic characteristics, predisposing factors, clinical signs and symptoms, laboratory findings, serial radiological assessments, histopathological results, antifungal treatment regimens, and clinical outcomes. Institutional Review Board approval was obtained from the Medical Ethics Committee of Huashan Hospital, Fudan University, Shanghai, China (IRB approval reference number: KY2022-1014). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Definitions
Orbital involvement in CIARS was defined by the following criteria: (1) radiological evidence of orbital extension and (2) compatible clinical features ophthalmologic symptoms [5]. Orbital apex syndrome was defined as the presence of vision loss due to optic neuropathy and restricted ocular motility, ptosis, or proptosis resulting from involvement of the ocular motor nerves within the orbital apex.
Cerebral involvement in CIARS was defined by radiological evidence of meningeal enhancement or cerebral parenchymal abnormalities consistent with invasive fungal disease (IFD), including cerebral abscesses, parenchymal lesions, ventricular enlargement, or ventriculomegaly [13].
Serum Aspergillus Immunoglobulin G Antibody and Galactomannan Detection
Baseline serum Aspergillus IgG antibody levels were measured after histopathologic confirmation and before the initiation of systemic antifungal therapy in all patients. Serum Aspergillus IgG antibody levels were measured using a commercial Aspergillus IgG enzyme-linked immunosorbent assay kit (IBL International, Hamburg, Germany), according to the manufacturer's predefined thresholds: positive (>11 NovaTec units [NTU]), equivocal (9–11 NTU), and negative (<9 NTU). Each sample was assayed in triplicate. A receiver operating characteristic (ROC) curve analysis was conducted to determine the optimal Aspergillus IgG antibody cutoff for predicting extrasinonasal involvement among patients with IgG-positive . Serum GM test was performed using Aspergillus GM detection kit (Genobio Pharmaceutical Co. Ltd., Tianjin, China) according to the manufacturer's instructions, with positivity defined as optical density index ≥ 0.5. All serum samples were collected at admission and stored at −80°C until analysis.
Longitudinal Aspergillus Immunoglobulin G Antibody Monitoring and Outcome Assessment
For longitudinal evaluation, follow-up serum Aspergillus IgG antibody levels were measured after 3–5 months of continuous antifungal therapy (median: 4 months) in 28 patients without modification of the treatment regimen. Follow-up assessments included physical examination, laboratory testing, and radiological evaluation using paranasal sinus computed tomography and cranial magnetic resonance imaging. Comparative analyses of pretreatment and post-treatment Aspergillus IgG levels were performed in relation to clinical and radiological findings. Patients who achieved both symptom resolution and radiological improvement were classified as the remission group, whereas those with persistent or progressive disease were classified as the stable group.
Statistical Analysis
Continuous variables with a normal distribution are presented as mean ± standard deviation (x ± s), while variables with a non-normal distribution are presented as median interquartile range (IQR). Categorical variables were analyzed using the chi-square test or Fisher's exact test, as appropriate. Continuous variables were analyzed using independent t-tests for normally distributed data, with normality assessed using the Shapiro–Wilk test. Univariate analyses were conducted to identify the risk factors associated with extrasinonasal involvement in CIARS. Variables with P < .05 in univariate analyses were included in a multivariable binary logistic regression model to identify independent risk factors for extrasinonasal involvement. Results are reported as adjusted odds ratios (ORs) with 95% CIs. A P value < .05 was considered statistically significant. ROC curve analyses were performed, and areas under the curve (AUCs) were calculated to assess diagnostic discrimination. The optimal cutoff value was determined using Youden's J statistic (sensitivity + specificity − 1). For longitudinal assessment of Aspergillus IgG antibody levels, paired t-tests were used to compare pre- and post-treatment IgG levels within each response group after confirming normality using the Shapiro–Wilk test (P > .05 for both groups). All statistical analyses were performed using SPSS version 29.0 (SPSS Inc.) or GraphPad Prism version 10.0 (GraphPad Software Inc.).
RESULTS
Patient Demographics and Baseline Characteristics
This study included 132 patients with a median age of 56 years (IQR: 49–66). Of these, 56 (42.4%) were male, and 55 (41.7%) had at least 1 predisposing factor. Baseline characteristics, predisposing factors, sinus involvement, and extrasinonasal extension are summarized in Table 1. Among patients with extrasinonasal involvement, orbital involvement was the most common (40.2%, 53/132), with 32 patients (24.2%) presenting with orbital apex syndrome (Table 2). This was followed by cranial involvement (22.0%, 29/132) and mastoid involvement (14.4%, 19/132; Table 3).
Serum Aspergillus Immunoglobulin G Antibody and Galactomannan Detection in Chronic Invasive Aspergillus Rhinosinusitis
Serum Aspergillus IgG antibody levels were measured in all 132 patients, of whom 50 (37.9%) tested positive. Positivity was significantly higher among patients with extrasinonasal involvement than among those with disease confined to the sinonasal region (59.2% [45/76] vs 8.9% [5/56]; P < .001). The highest IgG seropositivity rate was observed in patients with orbital apex syndrome (62.5% [20/32]), followed by cranial involvement (62.1% [18/29]) and orbital involvement (60.4% [32/53]) (Supplementary Figure 1A). In contrast, serum GM testing was positive in only 6.8% (9/132) of the patients (Supplementary Figure 1B). To further investigate the potential confounding by immune status, we also performed a stratified analysis in Supplementary Table 1, which summarizes IgG positivity and levels by immune status. However, no significance was identified.
ROC curve analysis using Youden's index identified an optimal serum Aspergillus IgG cutoff value of 13.08 NTU for distinguishing extrasinonasal involvement from disease confined to the sinonasal region among patients with IgG-positive. This cutoff yielded a sensitivity of 77.8% and a specificity of 100.0% (AUC = 0.884, 95% CI: 0.79–0.98; Figure 1).
ROC curve distinguishing extrasinonasal involvement from disease confined to the sinonasal region among patients with positive serum Aspergillus IgG antibody. The AUC was 0.884 (standard error: 0.049; 95% CI: 0.79–0.98). The optimal cutoff value was 13.08 NTU. Abbreviations: ROC, receiver operating characteristic; IgG, immunoglobulin G; AUC, area under the curve; CI, confidence interval.
Independent Risk Factors Associated With Extrasinonasal Involvement in Chronic Invasive Aspergillus Rhinosinusitis
Univariate analysis revealed several factors associated with extrasinonasal involvement, including male sex (51.3% vs 30.4%; P = .017), sphenoid sinus involvement (71.1% vs 30.4%; P < .001), ethmoid sinus involvement (90.8% vs 69.6%; P = .003), and positive serum Aspergillus IgG antibodies (59.2% vs 8.9%; P < .001). Positive serum Aspergillus IgG antibody (OR 11.28, 95% CI: 3.67–34.64, P < .001), sphenoid sinus involvement (OR 4.72, 95% CI: 1.89–11.79, P < .001), and ethmoid sinus involvement (OR 5.22, 95% CI: 1.53–17.86, P = .008) were identified as independent risk factors for extrasinonasal involvement in CIARS (Table 4).
Treatment Outcome
All patients received combined surgical intervention and antifungal therapy. Voriconazole was the most frequently administered agent (n = 124), followed by posaconazole (n = 4), itraconazole (n = 2), isavuconazole (n = 1), and amphotericin B deoxycholate (n = 1). The median duration of antifungal therapy was 6 months (range: 1–47 months). Treatment duration did not differ significantly among antifungal regimens. Notably, delayed initiation of antifungal therapy (> 1 month postoperatively) was confirmed as an independent risk factor for post-surgery recurrence, associated with a significantly higher recurrence rate of 54.8% (23/42) compared with 6.7% (6/90) in patients treated within 1 month (P < .001) (Supplementary Table 2).
Pre- and Post-antifungal Treatment Aspergillus Immunoglobulin G Antibody Dynamics and Therapeutic Response
Among the 28 patients with available paired baseline and prespecified follow-up serum Aspergillus IgG measurements, 19 (68.9%) achieved combined clinical and radiological remission (remission group). In contrast, 9 (32.1%) demonstrated persistent or progressive disease (stable group). The remission group demonstrated a significant reduction in serum Aspergillus IgG antibody levels from baseline, consistent with therapeutic response (median, 16.12 NTU; IQR, 12.87–21.96 vs median, 9.21 NTU; IQR, 6.52–13.23; P < .001; Figure 2A), corresponding to a median relative decrease of 51.5% (IQR, 24.6%–68.6%) from baseline. In contrast, no significant change in IgG levels was observed in the stable group (median, 12.84 NTU; IQR, 6.71–21.98 vs median, 12.30 NTU; IQR, 8.94–22.56; P = .381) (Figure 2B).
*Changes in serum Aspergillus IgG levels reflecting therapeutic response in 28 patients with CIARS. A, The remission group (n = 19) exhibited a significant decline post-treatment in IgG levels (P < .001). B, The stable group (n = 9) showed no significant change in IgG levels after treatment (P = .345). Abbreviations: CIARS, chronic invasive Aspergillus rhinosinusitis; IgG, immunoglobulin G; NS, not significant; NTU, NovaTec units. ***, P < .001.
DISCUSSION
The findings of this study indicate that patients with CIARS are at increased risk of developing extrasinonasal complications when sphenoid or ethmoid sinus involvement is present. More importantly, Aspergillus IgG—which plays a central role in CPA diagnosis [14]—was identified as a novel noninvasive biomarker with potential utility for risk stratification and prognostic assessment in CIARS.
In this study, patients with CIARS and extrasinonasal involvement more frequently exhibited sphenoid or ethmoid sinus involvement, findings that are consistent with prior studies identifying these sinuses as common sources of orbital complications [15–17]. Ethmoid sinus involvement has been reported as an independent risk factor for orbital complications in 43 patients with acute rhinosinusitis (OR = 31.1, 95% CI: 2.3–430.6) [18] Similarly, a retrospective study by Twu et al [19] involving 38 patients demonstrated that IFS originating from the sphenoid sinus (OR = 21.875, 95% CI: 3.295–145.237) or the posterior ethmoid sinus (OR = 14.0, 95% CI: 1.234–158.844) was more likely to disseminate to the orbital region . Although sphenoid and ethmoid sinus involvement have previously been identified as risk factors for orbital complications, this study is the first to demonstrate their association with broader extrasinonasal involvement, including cranial, orbital, and mastoid extension. These findings indicate that clinicians should remain vigilant for the development of multiple extrasinonasal complications in patients with CIARS who present with sphenoid or ethmoid sinus involvement.
Diagnostic challenges in CIARS remain substantial. The disease is frequently associated with orbital apex syndrome, which could lead to visual impairment or blindness, and intracranial extension might be fatal. However, establishing a definitive diagnosis in routine clinical practice is often difficult, as it typically relies on histopathological confirmation of fungal hyphae invading mucosal or submucosal tissues, vasculature, or bone. Galactomannan testing, one of the most commonly used assays for fungal infections, has been recommended as a primary screening tool for the early diagnosis of IFD. However, in non-neutropenic patients, GM testing demonstrates limited diagnostic performance, with a sensitivity of 23.1% and a specificity of 76.1% in individuals with nonhematologic disorders [20]. Moreover, GM testing was negative in 25 patients with histopathologically confirmed fungal ball of the paranasal sinuses [7], a finding consistent with our results.
Therefore, there is an urgent need to identify methods that enable the early and rapid detection of extrasinonasal involvement. Given the indolent course of CIARS, we evaluated the diagnostic performance of Aspergillus-specific IgG antibody testing in this patient population. Aspergillus-specific IgG antibodies are a well-established marker of infection in CPA and are recommended for clinical use in international guidelines [8]. Detection of Aspergillus-specific IgG antibodies is simple, inexpensive, and readily applicable in most clinical settings [21]. However, prior to this study, IgG testing had been used primarily for CPA, allergic bronchopulmonary aspergillosis and allergic fungal rhinosinusitis [22–24]. To date, only Hung et al reported that Aspergillus-specific IgG antibodies could be used in the diagnosis of chronic rhinosinusitis (CRS) [24], though their study was limited to type 2 CRS and extrasinonasal involvement was not evaluated. Notably, our study demonstrated that IgG seropositivity was substantially more prevalent among patients with CIARS and extrasinonasal involvement, suggesting that IgG detection could be a promising biomarker for prognostic assessment in CIARS. Thus, clinicians should remain alert to the possibility of extrasinonasal involvement when patients with CIARS present with relevant clinical symptoms and a positive Aspergillus IgG result.
Although not formally recommended by guidelines, Aspergillus IgG quantification has been used to diagnose CPA in large cohorts [25, 26]. Reported optimal diagnostic cutoffs vary by assay: 1.5 AU/mL for Bio-Rad (93% sensitivity, 98% specificity), 25 mg/L for Immulite (93% sensitivity, 99% specificity), 50 mg/L for ImmunoCAP (84% sensitivity, 96% specificity), and 50 U/mL for Serion (84% sensitivity, 91% specificity) [25]. However, positive results have been reported in approximately one-third of healthy individuals, underscoring the need to interpret Aspergillus IgG levels in conjunction with radiological findings [26]. In this study, we included patients with CIARS diagnosed based on histopathological and radiological findings. We further demonstrated that an Aspergillus IgG level > 13.08 NTU might serve as a promising indicator of extrasinonasal involvement at diagnosis, offering a potential strategy for risk stratification and treatment monitoring.
The mainstay of treatment for CIARS is surgical debridement combined with timely systemic antifungal therapy. Although some authors have suggested that surgery alone might be sufficient [27], our findings indicate that systemic antifungal treatment is an essential component of CIARS management. Since histopathological confirmation does not exclude an invasive process [19], delays in antifungal initiation are associated with an increased risk of CIARS progression. Therefore, our study indicates that patients with fungal rhinosinusitis and clinically evident neuro-orbital complications might still benefit from postoperative systemic antifungal therapy.
Evidence from multiple CPA cohorts support the potential value of monitoring Aspergillus IgG antibody levels to assess treatment response. Clinical management statements for CPA also acknowledge that serologic markers might serve as a valuable adjunct to clinical and radiological assessments during follow-up [28]. Li et al [9] examined longitudinal changes in Aspergillus IgG levels during antifungal therapy in CPA. They reported that serum IgG levels decreased in patients who responded to treatment but increased in those with subsequent disease progression, indicating that temporal IgG trends might reflect long-term therapeutic effectiveness. Similarly, Hung et al found an association between Aspergillus-specific IgG antibodies and symptom scores evaluated by the Sino-Nasal Outcome Test-22 [24]. Consistent with these observations, our study demonstrated that serial Aspergillus IgG monitoring in responders (66.7% of the follow-up cohort) was associated with significant declines in IgG levels, suggesting that IgG dynamics might serve as a potential marker of treatment response in CIARS.
This retrospective, single-institution study might represent the first cohort to examine the factors associated with extrasinonasal involvement in CIARS. Nevertheless, several limitations should be acknowledged. Given the rarity of CIARS, the subgroup sample sizes were relatively small. The retrospective design and incomplete data also limit the robustness of the findings. Additionally, cohort inclusion required histopathological confirmation, which might have preferentially selected patients undergoing surgery and potentially underrepresented milder disease presentations. Prospective, multicenter studies are required to validate the generalizability of these findings, including the transportability of the ROC-derived cutoff across assays and clinical settings. Future investigations should standardize sampling time points, incorporate longer-term serial measurements, and apply harmonized outcome definitions with prespecified analyses stratified by immune status. Systematic microbiological characterization, including species-level identification, would further strengthen the interpretation of the results and their clinical applicability.
CONCLUSION
This study demonstrates that serum Aspergillus IgG is an independent predictor of extrasinonasal involvement in CIARS. Serial IgG measurements could help evaluate treatment responses and support their use in long-term disease surveillance. Incorporating Aspergillus IgG testing into clinical practice might enable earlier risk recognition and facilitate timely intervention.
Supplementary Material
ofag059_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deutsch PG, Whittaker J, Prasad S. Invasive and non-invasive fungal rhinosinusitis- A review and update of the evidence. Med Kaunas Lith 2019; 55:319.10.3390/medicina 55070319 PMC 668135231261788 · doi ↗ · pubmed ↗
- 2Zhou LH, Wang X, Wang RY, et al Entities of chronic and granulomatous invasive fungal rhinosinusitis: separate or not? Open Forum Infect Dis 2018; 5:ofy 228.30302354 10.1093/ofid/ofy 228PMC 6171569 · doi ↗ · pubmed ↗
- 3Amedee RG . Survival outcomes in acute invasive fungal sinusitis: a systematic review and quantitative synthesis of published evidence. Am J Rhinol Allergy 2013; 27:338.29021077 10.2500/194589213807245011 · doi ↗ · pubmed ↗
- 4Cho HJ, Jang MS, Hong SD, Chung SK, Kim HY, Dhong HJ. Prognostic factors for survival in patients with acute invasive fungal rhinosinusitis. Am J Rhinol Allergy 2015; 29:48–53.25590320 10.2500/ajra.2015.29.4115 · doi ↗ · pubmed ↗
- 5Roland LT, Humphreys IM, Le CH, et al Diagnosis, prognosticators, and management of acute invasive fungal rhinosinusitis: multidisciplinary consensus statement and evidence-based review with recommendations. Int Forum Allergy Rhinol 2023; 13:1615–714.36680469 10.1002/alr.23132 · doi ↗ · pubmed ↗
- 6Denning DW, Chakrabarti A. Pulmonary and sinus fungal diseases in non-immunocompromised patients. Lancet Infect Dis 2017; 17:e 357–66.28774699 10.1016/S 1473-3099(17)30309-2 · doi ↗ · pubmed ↗
- 7Wei H, Li Y, Han D, et al The values of (1,3)-β-D-glucan and galactomannan in cases of invasive fungal rhinosinusitis. Am J Otolaryngol 2021; 42:102871.33412381 10.1016/j.amjoto.2020.102871 · doi ↗ · pubmed ↗
- 8Denning DW, Cadranel J, Beigelman-Aubry C, et al Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J 2016; 47:45–68.26699723 10.1183/13993003.00583-2015 · doi ↗ · pubmed ↗