Partially covered or uncovered metal stent efficacy in malignant unresectable distal biliary obstruction (METARSI): Randomized multicenter trial
Silvia Cocca, Flavia Pigò, Helga Bertani, Roberta Rea, Giuseppina Pontillo, Michele Campigotto, Giuseppe Grande, Salvatore Russo, Margherita Marocchi, Marinella Lupo, Gian Maria Prati, Giovanni Aragona, Raffaele Manta, Carmelo Barbera, Fabio Monica, Francesco Di Matteo

TL;DR
A study compared two types of metal stents for biliary drainage in patients with unresectable malignant biliary strictures and found no significant differences in effectiveness or survival.
Contribution
This randomized multicenter trial provides evidence on the comparative efficacy of partially covered versus uncovered metal stents in malignant biliary obstruction.
Findings
Partially covered and uncovered stents showed similar patency and survival rates.
Tumor ingrowth was rare and no patency advantage was observed with partially covered stents.
Procedure-related complications trended higher with partially covered stents but were not statistically significant.
Abstract
There is no consensus regarding optimal selection of self-expandable stents (SEMS) for biliary drainage with endoscopic retrograde cholangiopancreatography (ERCP). This study compared stent dysfunction, patient survival, and adverse events in patients with unresectable malignant distal biliary strictures (DBS) treated with ERCP, randomized to partially covered (PC-SEMS) or uncovered (U-SEMS) stents A prospective, multicenter, randomized controlled trial was performed in adult patients with DBS (March 2021-February 2023) with 12-month follow-up. Analyses were conducted according to intention-to-treat (ITT) and per-protocol (PP) principles. Procedural and post-procedural outcomes were evaluated using PP analyses and stent patency was evaluated with Kaplan-Meier analysis. Among 261 patients, 130 were randomized to PC-SEMS and 131 to U-SEMS. Baseline features were similar between groups…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
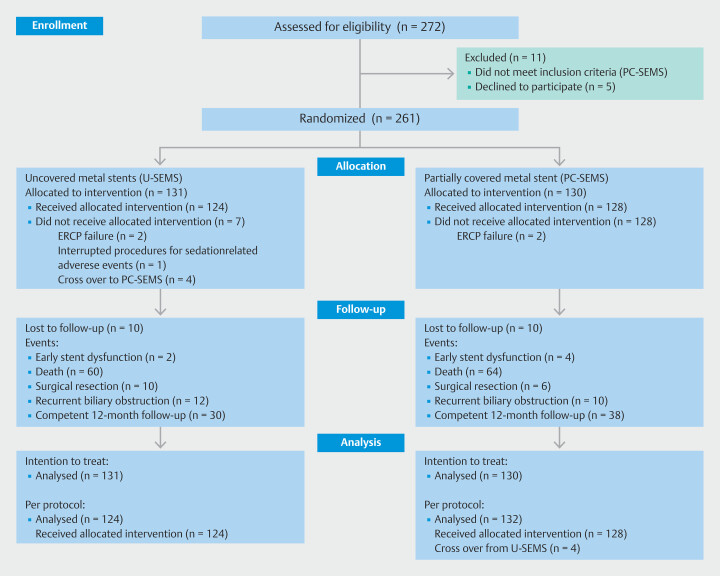 Fig. 1
Fig. 1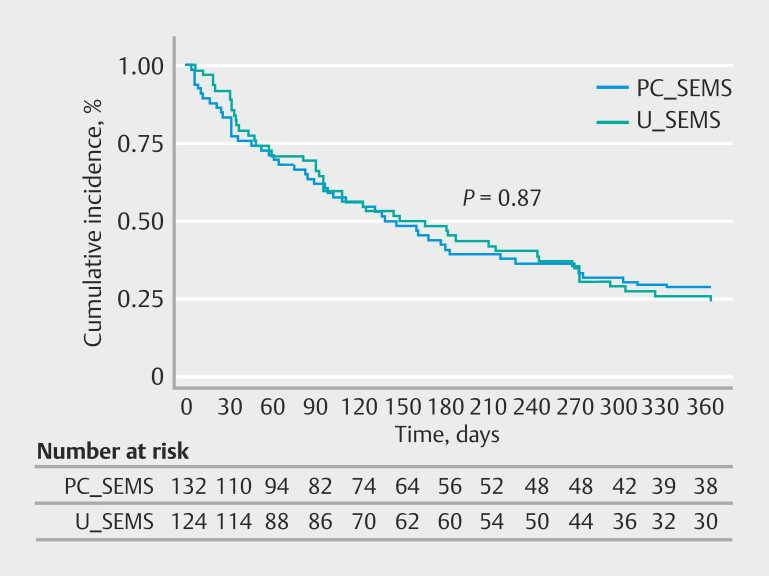 Fig. 2
Fig. 2|
|
| |||||||
|
|
|
|
|
|
|
|
| |
| CI, confidence interval; SD, standard deviation. | ||||||||
| Characteristics | ||||||||
| Age (years), mean ± SD | 73.5 ± 10.5 | 74.1 ± 9.8 | 73.9 ± 11.7 | 0.61 | 73 ± 11 | 74.5 ± 10.7 | 73.4 ± 12.8 | 0.59 |
| Sex (male), number (%;95% CI) | 132 (51%) | 58 (44.6%) | 74 (56;48–65) | 0.06 | 130 (51%) | 60 (48;39–58) | 70 (53;44–62) | 0.72 |
| Comorbidities, number | ||||||||
Hypertension | 66 (25%) | 28 (21;15–29) | 38 (29;22–37) | 0.20 | 64 (25%) | 30 (24;17–33) | 34 (26;19–34) | 0.88 |
Cardiac disease | 78 (30%) | 32 (25;18–33) | 46 (35;27–44) | 0.07 | 74 (29%) | 32 (25;18–34) | 42 (32;24–40) | 0.33 |
Metabolic disease | 46 (18%) | 18 (14;9–21) | 28 (21;15–29) | 0.14 | 44 (17%) | 20 (16;10–24) | 24 (18;12–26) | 0.74 |
Respiratory disease | 24 (9%) | 12 (9;5–16) | 12 (9;5–15) | 10.0 | 22 (8%) | 14 (11;6–18) | 8 (6;3–12) | 0.18 |
Neurological disease | 24 (9%) | 12 (9;5–16) | 12 (9;5–15) | 10.0 | 22 (8%) | 14 (11;6–18) | 8 (6;3–12) | 0.18 |
Renal disease | 20 (8%) | 8 (6;3–12) | 12 (9;5–15) | 0.48 | 18 (7%) | 10 (8;4–14) | 8 (6;3–12) | 0.62 |
Liver disease | 16 (6%) | 2 (1;0.1–6) | 14 (11;6–17) | 10.0 | 12 (5%) | 6 (5;2–12) | 6 (4;2–10) | 10.0 |
Gastrointestinal disease | 10 (4%) | 2 (1;0.1–6) | 8 (6;3–12) | 0.10 | 6 (2%) | 2 (2;0.1–6) | 4 (3;1–8) | 0.68 |
Other | 10 (4%) | 2 (1;0.1–6) | 8 (6;3–12) | 0.10 | 10 (4%) | 2 (2;0.1–6) | 8 (6;3–12) | 0.10 |
| No. comorbidities, number | ||||||||
None | 79 (30%) | 36 (27;21–36) | 43 (33;25–41) | 0.41 | 76 (30%) | 32 (25;18–34) | 44 (33;25–42) | 0.21 |
1 | 100 (38%) | 54 (35;33–50) | 46 (35;27–44) | 0.30 | 102 (40%) | 56 (45;36–54) | 46 (35;27–44) | 0.09 |
(≥ 2) | 82 (31%) | 40 (31;23–39) | 42 (32;25–40) | 0.89 | 78 (30%) | 36 (29;21–38) | 42 (32;24–40) | 0.51 |
| Etiology of distal malignant biliary obstruction, number (%; 95% CI) | ||||||||
Pancreatic adenocarcinoma | 196 (75%) | 96 (74;66–81) | 100 (76;68–82) | 0.66 | 188 (73%) | 92 (74;66–82) | 96 (73;64–80) | 1 |
Distal cholangiocarcinoma | 20 (8%) | 12 (9;5–16) | 8 (6;3–12) | 0.36 | 20 (8%) | 12 (10;5–16) | 8 (6;3–12) | 0.52 |
Ampullary adenomas | 25 (19%) | 10 (8;4–14) | 15 (11;7–18) | 0.40 | 28 (11%) | 8 (6;3–12) | 20 (15;10–22) | 0.15 |
Metastatic disease | 20 (8%) | 12 (9;5–16) | 8 (6;3–12) | 0.36 | 20 (8%) | 12 (10;5–16) | 8 (6;3–12) | 0.52 |
| Disease stage, number (%; 95% CI) | 0.90 | 0.80 | ||||||
Locally advanced neoplasia | 134 (51%) | 66 (51;42–59) | 68 (52;43–60) | 134 (53%) | 66 (53;44–62) | 68 (51;43–60) | ||
Metastatic neoplasia | 127 (49%) | 64 (49;41–58) | 63 (48;40–57) | 122 (48%) | 58 (47;38–56) | 64 (48;40–57) | ||
| Gallbladder lithiasis, number (%; 95% CI) | 16 (6%) | 6 (5;2–10) | 10 (8;4–14) | 0.44 | 14 (5%) | 8 (6;3–12) | 6 (4;2–10) | 0.71 |
| History of cholecystectomy, number (%; 95% CI) | ||||||||
Total bilirubin (mg/dL) | 11.2 ± 7.6 | 12.4 ±7.3 | 11.2 ± 8.3 | 0.30 | 11.8± 7.7 | 12.5 ± 7.2 | 11.0 ± 8.1 | 0.28 |
Direct bilirubin (mg/dL) | 7.8 ± 5.2 | 8.2 ± 4.8 | 7.4 ± 5.5 | 0.51 | 7.7 ± 5.1 | 8.0 ± 4.9 | 7.3 ± 5.4 | 0.49 |
Alanine aminotransferase (IU/L) | 198.1 ± 236.6 | 196.7 ± 189.2 | 212.6 ± 291.5 | 0.37 | 202.0 ± 245.8 | 192.8 ± 199.2 | 212.6 ± 291.5 | 0.66 |
Gamma-glutamyltransferase (IU/L) | 689.1 ± 568.1 | 757.5 ± 610.3 | 614.6 ± 514.0 | 0.43 | 679.0 ± 571.2 | 754.2 ± 620.1 | 604.5 ± 523.1 | 0.34 |
Alkaline phosphatase (IU/L) | 556.1±463.0 | 597.7±486.1 | 512.1±440.2 | 0.38 | 556.8 ± 463.9 | 597.7 ± 486.1 | 512.1 ± 440.2 | 0.38 |
| Neoadjuvant chemotherapy or radiotherapy candidates, number (%;95% CI) | 140 (54%) | 66 (51;42–59) | 74 (56;48–65) | 0.38 | 138 (54%) | 68 (55;46–64) | 70 (53;44–62) | 0.86 |
| Karnofsky performance scores, mean ± SD | 82.5 ± 10.2 | 81.3 ± 11.0 | 82.4 ± 10.9 | 0.64 | 81.3 ±10.9 | 80.9 ± 10.4 | 81.7 ± 11.3 | 0.94 |
|
|
|
|
|
|
| CI, confidence interval; ERCP, endoscopic retrograde cholangiopancreatography; PC-SEMS, partially- covered self-expandable stent; U-SEMS, uncovered self-expandable stent. | ||||
| Bile duct access, number (%; 95% CI) | ||||
Direct | 212 (83%) | 112 (90; 84–95) | 100 (76; 68–83) | 0.04 |
Precut | 36 (14%) | 10 (8; 4–14) | 26 (20; 13–28) | 0.07 |
Trans-pancreatic septotomy | 8 (3%) | 2 (2; 1–6) | 6 (4; 2–10) | 0.61 |
| Sphincterotomy, number (%; 95% CI) | 194 (76%) | 90 (72; 64–80) | 104 (79; 71–85) | 0.53 |
| Cystic duct infiltration number (%; 95% CI) | 38 (15%) | 24 (19; 13–27) | 14 (11; 6–17) | 0.28 |
| Size of study stent, length in mm × diameter in mm, number (%; 95% CI) | ||||
40 × 10 | 68 (26%) | 26 (21; 14–29) | 42 (32; 24–40) | 0.23 |
60 × 10 | 174 (68%) | 88 (71; 62–79) | 86 (65; 56–73) | 0.57 |
80 × 10 | 14 (5%) | 10 (8; 4–14) | 4 (3; 1–8) | 0.26 |
| Stent placement over cystic duct origin, number (%;95% CI) | 64 (25%) | 32 (26; 18–34) | 32 (24; 17–32) | 0.84 |
| Stent model, number (%; 95% CI) | ||||
WallFlex | 190 (74%) | 88 (71; 62–79) | 102 (77; 69–84) | |
ComVi | 44 (17%) | 14 (11; 6–18) | 30 (23; 16–31) | |
Evolution | 22 (8%) | 22 (18; 11–26) | N/A | |
|
|
| |||||
|
|
|
|
|
|
| |
| CI, confidence interval; ERCP, endoscopic retrograde cholangiopancreatography; PC-SEMS, partially-covered self-expandable stent; U-SEMS, uncovered self-expandable stent. | ||||||
| Characteristic | ||||||
| Technical success, number (%; 95% CI) | 127 (98; 93–99) | 129 (98; 95–100) | 0.68 | 124 (100) | 132 (100) | 1.0 |
| Clinical success, number (%; 95% CI) | 86 (66; 57–74) | 92 (70; 62–78) | 0.50 | 84 (68; 59–76) | 94 (71; 63–79) | 0.58 |
| Procedure related complications, number (%; 95% CI) | ||||||
Early adverse events | 3 (3; 1–8) | 8 (6; 3–12) | 0.37 | 3 (2; 1–7) | 9 (7; 3–13) | 0.13 |
Pancreatitis | 1 (1; 0.1–4) | 1 (1; 0.1–4) | 1.00 | |||
Acute cholecystitis | 0 | 2 (1; 0.1–5) | 0.49 | |||
Stent malfunction | 1 (1; 0.1–4) | 2 (1; 0.1–5) | 1.00 | |||
Bleeding | 0 | 0 | 0 | |||
Perforation | 0 | 0 | 0 | |||
Cholangitis (without stent occlusion) | 1 (1; 0.1–4) | 4 (3; 0.1–6) | 0.37 | |||
Late adverse events | 0 | 0 | 1.00 | |||
| Overall stent dysfunction rate, number (%; 95% CI) | 15 (11; 7–18) | 17 (13; 8–20) | 0.85 | 14 (11; 6–18) | 18 (14; 8–21) | 0.70 |
| Recurrent biliary obstruction (stent dysfunction rate), number (%; 95% CI) | 13 (10; 5–16) | 13 (10; 5–16) | 1.00 | 12 (10; 5–16) | 14 (11; 6–17) | 1.00 |
Migration | 0 | 2 (2;0.1–5) | 0.23 | |||
Occlusion | 10 (8;4–14) | 12 (9;5–15) | 0.82 | |||
| Time stent patency, days (median, 25th-75th percentiles) | 210 (27–270) | 92 (5–201) | 0.52 | 268 (34–273) | 87 (5–193) | 0.45 |
| Time to stent patency adjusted, days (median, 25th-75th percentiles) | 132 (57–273) | 127 (61–219) | 0.78 | |||
| Post-ERCP surgical resection, number (%;95% CI) | 8 (6; 3–12) | 6 (4; 2–10) | 0.71 | |||
| Time to surgical resection, days (mean ± SD) | 95.8 ± 45.9 | 83.0 ± 61.5 | 0.06 | |||
| Death, number (%;95% CI) | 62 (50; 41–59) | 64 (48; 40–57) | 0.44 | |||
| Survival time, days (median, 25th-75th percentiles) | 106 (34–168) | 103 (36–177) | 0.30 | 108 (47–215) | 100 (33–178) | 0.14 |
| Follow-up | ||||||
| Total time, days (median, 25th-75th percentiles) | 132 (48–273) | 109 (45–206) | 0.22 | |||
| Lost to follow-up, number (%;95% CI) | 10 (8; 4–14) | 10 (7; 4–13) | 1.0 | |||
| Time to lost follow-up, days (median, 25th-75th percentiles) | 62 (31–181) | 31 (31–61) | 0.40 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Pancreatic and Hepatic Oncology Research
Introduction
It is estimated that 80% to 95% of biliary strictures in adults are malignant 1 2 . The most common cause of malignant distal biliary duct stricture (DBS) is pancreatic adenocarcinoma (extrahepatic). Other causes include cholangiocarcinoma, ampullary carcinoma, lymphoproliferative disorders, metastatic disease, and other local cancers (gallbladder and liver malignancies) 3 . Common clinical symptoms of malignant DBS are painless jaundice due to obstruction of bile flow, which can lead to various adverse events (AEs), including ascending cholangitis, vitamin and fat malabsorption, and coagulopathy complications 2 4 . Typically, patients with DBS have poor quality of life and prognosis, with an overall 5-year survival rate of less than 5%. It has been reported that at time of diagnosis, most lesions (70%) are unfit for curative tumor surgery, due to late symptom presentation and typical onset in elderly patients unfit for surgery. Therefore, palliative strategies are most commonly adopted 1 3 5 .
European guidelines recommend biliary drainage for biliary decompression for selected cases involving cholangitis, severe symptomatic jaundice, delayed demolitive tumor surgery, or neoadjuvant chemotherapy in jaundiced patients 4 . Drainage can be performed with various interventional strategies, including endoscopic, radiologic, or surgical approaches 4 6 .
The European Society of Gastrointestinal Endoscopy (ESGE) recommends endoscopic retrograde cholangiopancreatography (ERCP) because it is less invasive with a better cost-benefit ratio than surgery or percutaneous interventions 4 6 7 and has a lower risk of tumor seeding and complications compared with radiologic approaches 3 4 . If ERCP fails, ESGE recommends an endoscopic ultrasound (EUS)-guided approach 4 5 .
ERCP in patients with DBS can be performed with deployment of plastic or metallic self-expandable stents (SEMS). Compared with plastic, SEMS have been associated with lower risk of stent dysfunction and cholangitis and fewer reinterventions 6 8 . Commercially available SEMS are fully covered (FC-SEMS), uncovered (U-SEMS), or partially covered (PC-SEMS).
FC-SEMS were developed to prevent stent occlusion by tumor/tissue ingrowth with introduction of an internal covered mesh. However, although FC-SEMS are less likely to permit tumor ingrowth, no clear patency advantages associated with FC-SEMS have been reported. High rates of tumor overgrowth around the stent and sludge formation, coupled with risk of migration, have been observed 9 10 . Theoretical risk of cholecystitis in the case of coverage of the cystic duct by stent obstruction has also been highlighted. Therefore, PC-SEMS with uncovered flare ends were introduced. Both U-SEMS and PC-SEMS are permanently deployed and are most frequently selected for patients with DBS who are unfit for curative tumor surgery 11 12 .
A consensus regarding optimal stent selection between PC-SEMS and U-SEMS in ERCP for DBS is lacking. Several studies have compared FC-SEMS and U-SEMS; randomized controlled trials (RCTs) were performed in Canada and South Korea and authors concluded that PC-SEMS do not seem to provide benefits compared with U-SEMS 13 14 15 . Park et al. called for more RCTs to clarify the optimal role of PC-SEMS. Our study provides evidence for a European population. Further, our data contribute to the number of DBS patients enrolled in RCTs for future meta-analyses or to provide further evidence for development of a consensus.
The primary aim of this study was to compare overall stent dysfunction in DBS with PC-SEMS and U-SEMS. Secondary aims were to evaluate technical and clinical success, recurrent biliary obstruction/stent patency time, patient survival, and incidence of procedural-related complications.
Patients and methods
Study design
This investigator-led, prospective, multicenter RCT was conducted between March 2021 and December 2022 in four Italian centers (Azienda Ospedaliero-Universitaria of Modena, Campus BioMedico University of Rome, Cattinara University Hospital of Trieste and Hospital of Piacenza-Piacenza). The study was approved by the Ethics Committee of the coordinating center (Comitato Etico Area Vasta Emilia Nord, prot n.947/2020) and participating centers. The study was registered on ClinicalTrials.gov, protocol number: NCT04431427.
Study population
Consecutive subjects undergoing ERCP for placement of SEMS for a malignant DBS during the study period were evaluated for study enrolment. Criteria for study inclusion specified: 1) patient age > 18 years; 2) neoplasia of the biliary or pancreatic tract unsuitable for surgical resection at the time of the ERCP procedure; 3) malignant distal biliary obstruction (≥ 1 cm distal to the biliary hilum); 4) assessment with the Karnofsky performance score; and 5) informed consent for study participation. Exclusion criteria specified: 1) history of biliary tract surgery (other than cholecystectomy); 2) previous biliary SEMS placement; and 3) coagulopathy (INR > 1.5 or platelet count < 50,000).
Karnofsky performance score, widely used in oncology and palliative care, evaluates disease burden and treatment efficacy on a scale ranging from 0 (death) to 100 (normal functioning). Scores were classified as mild (80–100), moderate (50–70), and severe impairment (< 50) 16 .
Comorbidities, diagnoses of malignancy, and Karnofsky performance scores were based on clinical, laboratory, radiologic, and/or pathologic findings. Disease stages and neoadjuvant chemotherapy and/or radiotherapy eligibility were determined from computed tomography and EUS findings. Data were collected at each participating center in dedicated case report forms and Excel databases. A central data manager combined the local databases into a single study dataset for analysis.
Randomization
Patients were randomly allocated in a 1:1 ratio using a block size of four, stratified according to trial site. No competitive policy for the patient recruitment process was used. Patients were assigned to each group by a central registration method. After medical classification of study suitability, endoscopic procedure feasibility was determined when biliary duct access was achieved. The case was then communicated to a data manager at the coordinating center for electronic patient randomization to PC-SEMS or U-SEMS. Crossovers were permitted in cases in which multidisciplinary consideration for patient future surgery changed during the ERCP procedure.
Procedures
All patients underwent ERCP in a supine or lateral position using a standard duodenoscope under deep sedation. Prophylaxis of post-ERCP pancreatitis (indomethacin or diclofenac suppository and Ringer's Lactate infusion) was performed in all patients without specific contraindications 17 . Access to the papilla was achieved directly. In cases of difficult biliary cannulation (defined as > 5 contacts with the papilla or > 5 minutes of cannulation attempts or > 1 pancreatic duct cannulation/opacification 17 ), a precut biliary sphincterotomy (fistulotomy [needle-knife sphincterotome], transpapillary septotomy [standard sphincterotome]), or endoscopic-radiologic rendezvous (salvage technique) was performed.
After biliary access, features of the stricture (such as angulation and length) were evaluated with cholangiography. Cystic duct occlusion (opacification during cholangiography) and stent placement covered the cystic duct origin were recorded. Stents were placed under fluoroscopic and endoscopic guidance by experienced pancreaticobiliary endoscopists. Stent length was chosen to extend approximately 1 cm beyond both the proximal and distal stricture margins. Available stents were WallFlex (Boston Scientific Japan, Tokyo, Japan), ComVi (Taewoong, South Korea) and Evolution (CookMedical, Livery, Ireland).
All patients received periprocedural antibiotic prophylaxis. In cases of fever with positive blood cultures, antibiotic treatment was prescribed for 7 days.
Follow-up
Follow-up consisted of clinical visits or telephone contact at 3, 6, 9, and 12 months (± 3 weeks). Laboratory exams were requested between 3 to 6 weeks post-procedure and at each subsequent follow-up point.
Recurrent biliary obstruction was suspected in patients with clinical symptoms of obstructive jaundice or cholangitis and evaluated for reintervention via ERCP.
Patients unreachable by phone were considered lost to follow-up. Analyses were performed using intention-to-treat (ITT) and per-protocol (PP) approaches, with patients censored at time of the most recent follow-up.
Technical, procedure, and follow-up data for procedure-related complications and recurrent biliary obstruction were recorded.
Definitions and endpoints
Primary endpoints
Overall stent dysfunction was defined as loss of adequate biliary drainage due to occlusion or migration requiring endoscopic reintervention. Time to stent patency was measured from initial SEMS placement to occlusion or migration .
Secondary endpoints
Technical success was defined as SEMS deployment in the intended location with sufficient coverage of the stricture 18 19 , technical radiological stent visualization, and flow of contrast medium or bile through the stent 18 20 .
Clinical success followed ESGE criteria 4 : bilirubin < 2 mg/dL within 3 weeks if baseline bilirubin < 10 mg/dL, or within 6 weeks if baseline bilirubin ≥ 10 mg/dL.
Suspected obstruction and migration were confirmed during ERCP reintervention.
Procedure-related complications included pancreatitis, cholecystitis (acute), cholangitis, stent malfunction (incomplete opening), bleeding/ulceration, and perforation, registered within 30 days 17 21 . Early complications were defined as ≤ 7 days; late complications > 7 days. Early stent dysfunction was defined as incomplete drainage due to sludge or incomplete expansion within ≤ 7 days. Early stent dysfunction was defined as incomplete drainage of the stent (from sludge or incomplete opening) ≤ 7 days. Recurrent biliary obstruction was defined as loss of adequate biliary drainage (due to occlusion or migration) requiring endoscopic reintervention > 7 days from base intervention. Adjusted patency time excluded early dysfunction cases (< 7 days).
Stent migration was defined as symptomatic dislodgement from the intended and original implant position, confirmed by imaging and/or clinical evidence of cholangitis or obstructive jaundice. Patient survival was defined from initial stent placement to all-cause mortality or lost to follow-up.
Statistics
Previous pooled results reported an overall stent dysfunction relative risk of 0.85 (absence of recurrent symptomatic biliary obstruction was equivalent to the duration from primary stent placement to stent dysfunction), corresponding to an incidence of 25% in U-SEMS patients 22 . Assuming a 15% decrease in stent dysfunction with PC-SEMS, with an alpha-error of 0.05 and a power of 0.8, calculations approximated 100 patients were required for each group. Accounting for drop-outs and competing risks (surgical resection and high mortality within 1-year) target enrollment was increased by 30%.
Continuous variables were expressed as mean ± standard deviation or median and interquartile range (IQR) according to parametric or non-parametric distribution. Categorical variables were expressed as percentage. Patency was evaluated with the Kaplan-Meier method and compared with the log-rank test. Unadjusted and adjusted patency times were calculated. Patients with patent stents were censored at the last follow-up or death; surviving patients were censored at their last follow-up.
Group comparisons used chi-square or Fisher’s exact test for categorical variables and t -test or Wilcoxon test for continuous variables, according to distribution. ITT and PP analyses were performed. Protocol deviations (such as randomization before biliary cannulation) and untreated patients were excluded from PP analysis. P <.05 was considered significant. The analysis was conducted with the Stata statistical software, version 13.1 (StataCorp, Texas, United States).
Results
Patient characteristics
Of the 272 patients assessed for the present study, 261 met inclusion criteria and were enrolled. Of these, 131 were randomized to U-SEMS and 130 to PC-SEMS. Allocated interventions were not performed in two and seven patients, respectively. In both arms, 10 patients were lost to follow-up ( Fig. 1 ) 23 .
Consort flow diagram.
Patients included in ITT and PP analyses are shown in Table 1 . No statistically significant differences were observed between treatment groups at baseline with either analysis. Mean Karnofsky performance scores were mild. Mean age was 73 ± 11 years and 51% were male in the total population. The most commonly reported comorbidities were cardiac (30%) and metabolic diseases (18%) and hypertension (25%). Most DBS cases were due to pancreatic adenocarcinoma (75%). Patients had either locally advanced neoplasia (51%) or metastatic disease (49%) and just over half were classified as candidates for neoadjuvant chemotherapy or radiotherapy (54%).
: Table 1 Baseline patient characteristics: Intention-to-treat and per-protocol analyses.
In PP analysis, direct bile duct access was achieved in over 80% of patients, with a significantly higher representation in the U-SEMS group ( P = 0.04). In cases of ERCP failure, a rendezvous procedure was performed. SEMS length ranged from 40 to 80 mm (10-mm diameter). Intentional stent deployment over the origin of the cystic duct was performed in 25% of procedures. Procedure characteristics are summarized in Table 2 .
: Table 2 ERCP procedure characteristics (per-protocol analysis).
Post-ERCP characteristics were similar between groups. In PP analyses, technical success was achieved in 100% of procedures and clinical success was registered in 68% (U-SEMS) and 71% (PC-SEMS). A trend toward more overall procedure-related complications was observed in the PC-SEMS group ( P = 0.07).
Two patients developed moderate pancreatitis within 7 days of the ERCP procedure; both patients were successfully managed with medical treatment. Acute cholecystitis developed in two patients from the PC-SEMS group; both patients were subjected to an ERCP reintervention with PC-SEMS removal and substitution with U-SEMS. Five patients developed cholangitis: four patients (PC-SEMS) without stent occlusion were treated with antibiotic therapy alone and the remaining patient had stent occlusion by biliary sludge (U-SEMS) and was treated with an endoscopic reintervention to insert a coaxial biliary plastic stent. Stent malfunction was registered in three patients (1 U-SEMS and 2 PC-SEMS), each requiring endoscopic placement of a coaxial plastic stent. No cases of bleeding or perforation were reported. All complications occurred within 7 days of the procedure. All post-ERCP data are summarized in Table 3 .
Post-ERCP stent dysfunction was observed in 15 patients (11%; 95%CI 7–18) treated with U-SEMS and 17 patients (13%; 95% confidence interval [CI] 8–20) treated with PC-SEMS (not significant). Surgical resection rates were slightly higher in the U-SEMS group, which also had marginally longer follow-up duration. Recurrent biliary obstruction due to tumor ingrowth with or without biliary sludge impaction occurred in 22 (U-SEMS n = 10, PC-SEMS n = 10). Both cases of stent migration were observed in patients treated with PC-SEMS. All obstructions and migrations were treated with ERCP reinterventions with deployment of coaxial plastic stents. Patency rates were unstable (wide [CIs) and meaningful interpretation is difficult to make ( Fig. 2 ). Ten patients were lost to follow-up in each group; the overall rate was 7.7%. These patients did not attend scheduled visits and were unable to be reached by telephone.
Patency rates.
: Table 3 Post-procedure characteristics (intention to-treat and per protocol analysis).
There were no differences in survival time between stent types over the 360-day observation period (range 34–177 days). Post-procedure characteristics are outlined in Table 3 .
Discussion
This prospective investigator-led, multicenter, randomized trial reports similar stent dysfunction, patient survival, and procedure-related complications in patients with unresectable malignant DBS treated with ERCP with either U-SEMS or PC-SEMS. A trend toward a higher complication rate was observed in the PC-SEMS group.
ERCP is the preferred palliative treatment for patients with DBS, compared with surgery or percutaneous approaches. Among available stents, SEMS have been shown to provide superior patency and a more favorable cost-effectiveness profile than plastic stents 24 . However, evidence remains inconsistent regarding optimal SEMS design for DBS.
Many SEMS types are commercially available, including PC-SEMS, FC-SEMS, and U-SEMS. U-SEMS typically demonstrate higher rates of tumor ingrowth (16%-46%) 6 24 , whereas FC-SEMS are associated with increased sludge deposition, tumor overgrowth, stent migration, cholecystitis, and pancreatitis 15 17 . Few studies have directly compared PC-SEMS with U-SEMS; however, most dedicated investigations concur that PC-SEMS are associated with lower rates of tumor ingrowth and AEs, while maintaining comparable migration rates and overall patient survival to U-SEMS 17 .
A systematic review and metanalysis published in 2013 identified eight RCTs and three prospective studies reporting SEMS deployment in all types of malignant obstructions of the digestive tract 25 . Only a limited number of these patients had undergone ERCP specifically for DBS (range 3–307). The authors reported substudy outcomes demonstrating comparable rates of stent patency, overall survival, and stent dysfunction-free survival to those observed in our study. Yang et al. similarly found no significant differences in overall AEs, including pancreatitis and cholecystitis, over a 12-month follow-up period. Accordingly, the review concluded that FC-/PC-SEMS and U-SEMS perform equivalently in these metrics 25 . A more recent RCT in patients with unresectable malignant DBS treated with PC-SEMS and U-SEMS (n = 258 patients) reported no clear advantages in stent patency or overall survival, but underscored lower tumor ingrowth rates with PC-SEMS 17 .
Despite the theoretical advantage conferred by the internal mesh of PC-SEMS, our study found no difference in tumor ingrowth between groups. Park et al. Previously reported reduced tumor ingrowth with PC-SEMS and suggested that chemotherapy may enhance stent patency by reducing disease burden. However, our findings did not confirm these associations, despite similar rates of chemotherapy exposure across cohorts.
In our study, both cases of stent migration observed were treated with PC-SEMS. Because these events were detected early, we hypothesize that migration may have occurred before the flared ends had adequately embedded into the biliary duct wall. A single-center, three-armed RCT in patients with unresectable DBS reported longer stent patency, fewer AEs (including cholangitis and cholecystitis), and lower migration rates with PC-SEMS 26 . Although our trial similarly demonstrates comparable patency and survival between PC- and U-SEMS, we observed a trend toward higher complication rates in the PC-SEMS group.
Most patients were classified with a mild Karnofsky score at baseline. Nevertheless, most deaths were registered within 4 months. Although mortality rates were similar between treatment groups, overall survival in our study was shorter than that reported in comparable cohorts. Yokota et al 11 reported median survival periods of 172 and 161 days for PC-SEMS and U-SEMS in a similar patient cohort (treated with Wallflex SEMS), whereas our cohort demonstrated notably shorter survival (108 and 100 days). This discrepancy may reflect overestimation of patient baseline functional status, raising the issue of applicability of patient classification with the Karnofsky score in this patient population for meaningful comparison.
In addition, the relatively low number of AEs observed in our study may be attributable to limited patient survival, which shortened the window for late complications to manifest.
Performance of SEMS may also be influenced by underlying disease. A recent review comparing FC-SEMS and U-SEMS reported that locally advanced pancreatic cancer was associated with greater cumulative patency than other cancer types, whereas no significant differences were observed in metastatic pancreatic cancer, likely due to shortened survival 27 . In our study, the small number of recorded events precluded meaningful assessment of disease-specific effects on patency and survival. Notably, none of the patients with pancreatic adenocarcinoma were alive at 12-month follow-up, underscoring the aggressive clinical trajectory of this disease.
This study is mainly limited by a lower-than-expected number of events, protocol deviations, and potential inclusion of patients with moderate to severe disease burden. The original sample size calculation assumed a stent dysfunction rate of approximately 25%. Although the study had sufficient power to detect large differences, it was underpowered to detect the small absolute difference observed between arms. Consequently, this trial cannot exclude either equivalence or a small benefit of one stent over another. The initial protocol specified patient classification as “fit” and “unfit”; however, the limited number of events, short patient survival, and relatively high rate of loss to follow-up restricted the ability to perform meaningful post-procedure comparisons. Nonetheless, the proportion of patients lost to follow-up was in line with other RCTs 15 .
The authors emphasize that SEMS outcomes are also influenced by radial and longitudinal forces exerted on the biliary duct, the specific anchoring mechanism, and morphology of the obstruction, which were not evaluated in this study. Meta-analyses and larger multicenter studies are required for complete risk factor analyses. Generalizability of our study results is limited to settings with experienced endoscopists. Further, more recent technological advancements in SEMS, such as drug-eluting, antireflux, and multi-hole- EMS 28 , were not included in our study and are expected to further improve outcomes. Although biliary drainage can improve the clinical condition of DBS patients, assessment of all aspects of well-being in this patient population should be included in future research 29 .
Although our findings did not demonstrate differences in overall stent patency, PC-SEMS may still play a role in selected patient subgroups. In particular, in patients with longer expected survival or who may convert from unfit to fit for surgery after effective chemotherapy, the partial covering could theoretically reduce late tumor ingrowth and facilitate reintervention. In our cohort, late tumor ingrowth was not observed, likely due to short patient survival, which limited the time window in which ingrowth typically becomes clinically relevant and may have masked any potential difference between stent types. Although this theoretical advantage of PC-SEMS could not emerge within the timeframe and clinical characteristics of our study, future trials stratified by survival expectancy and treatment response are warranted to determine whether PC-SEMS offer a meaningful benefit in patients with better prognoses.
Conclusions
Results from our prospective multicenter RCT indicate that, in the clinical scenario of malignant unresectable distal biliary strictures, the choice between PC-SEMS and U-SEMS does not substantially affect stent patency or survival. A trend toward a higher incidence of procedure-related complications with PC-SEMS was observed, highlighting the need for careful patient selection and further targeted investigations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singh A Gelrud A Agarwal B Biliary strictures: diagnostic considerations and approach Gastroenterol Rep (Oxf)20153223110.1093/gastro/gou 07225355800 PMC 4324869 · doi ↗ · pubmed ↗
- 2Elmunzer BJ Maranki JLGómez VACG Clinical Guideline: Diagnosis and Management of Biliary Strictures Am J Gastroenterol 202311840542610.14309/ajg.000000000000219036863037 · doi ↗ · pubmed ↗
- 3Tanisaka Y Mizuide M Fujita A Current Status of Endoscopic Biliary Drainage in Patients with Distal Malignant Biliary Obstruction J Clin Med 202110461934640637 10.3390/jcm 10194619 PMC 8509542 · doi ↗ · pubmed ↗
- 4Dumonceau J-M Tringali A Papanikolaou IS Endoscopic biliary stenting: indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline - Updated October 2017 Endoscopy 20185091093010.1055/a-0659-986430086596 · doi ↗ · pubmed ↗
- 5Marzioni M CrinòSF Lisotti A Biliary drainage in patients with malignant distal biliary obstruction: results of an Italian consensus conference Surg Endosc 2024386207622639317905 10.1007/s 00464-024-11245-4PMC 11525304 · doi ↗ · pubmed ↗
- 6Scatimburgo MVCV Ribeiro I Bde Moura DTH Biliary drainage in inoperable malignant biliary distal obstruction: A systematic review and meta-analysis World J Gastrointest Surg 20211349350634122738 10.4240/wjgs.v 13.i 5.493PMC 8167848 · doi ↗ · pubmed ↗
- 7Glazer ES Hornbrook MC Krouse RSA meta-analysis of randomized trials: immediate stent placement vs. surgical bypass in the palliative management of malignant biliary obstruction J Pain Symptom Manage 20144730731410.1016/j.jpainsymman.2013.03.01323830531 PMC 4111934 · doi ↗ · pubmed ↗
- 8Jang S Stevens T Parsi MA Superiority of self-expandable metallic stents over plastic stents in treatment of malignant distal biliary strictures Clin Gastroenterol Hepatol 202220 e 182e 19510.1016/j.cgh.2020.12.02033346140 · doi ↗ · pubmed ↗