Trapped Lung and Pneumothorax Ex Vacuo
Mashal Binte Ali, Danish Jilani, Meher Binte Ali

TL;DR
This paper discusses trapped lung and pneumothorax ex vacuo, which happen when lungs don't expand after draining fluid from the chest cavity.
Contribution
The paper provides a clinical overview of diagnosis and management strategies for these rare post-drainage complications.
Findings
Trapped lung and pneumothorax ex vacuo are rare complications after large pleural effusion drainage.
Asymptomatic patients may not require immediate treatment, while symptomatic cases often need surgery.
Iatrogenic pneumothorax typically requires chest tube placement for resolution.
Abstract
Trapped lung and pneumothorax ex vacuo occur due to failure of lungs to re‐expand after drainage of a large pleural effusion. Asymptomatic patients can be observed while symptomatic patients may need surgical decortication. Iatrogenic pneumothorax results from introduction of air into the pleural space and usually requires chest tube placement.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
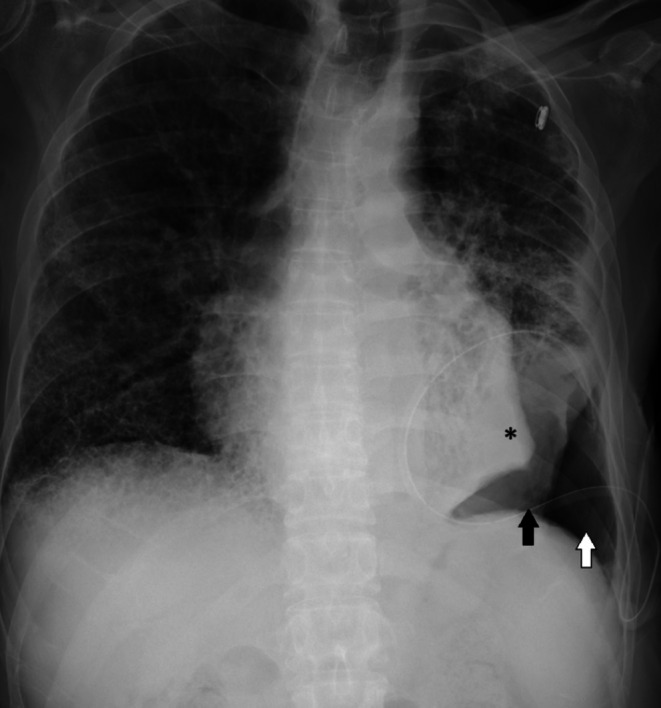 Figure 1
Figure 1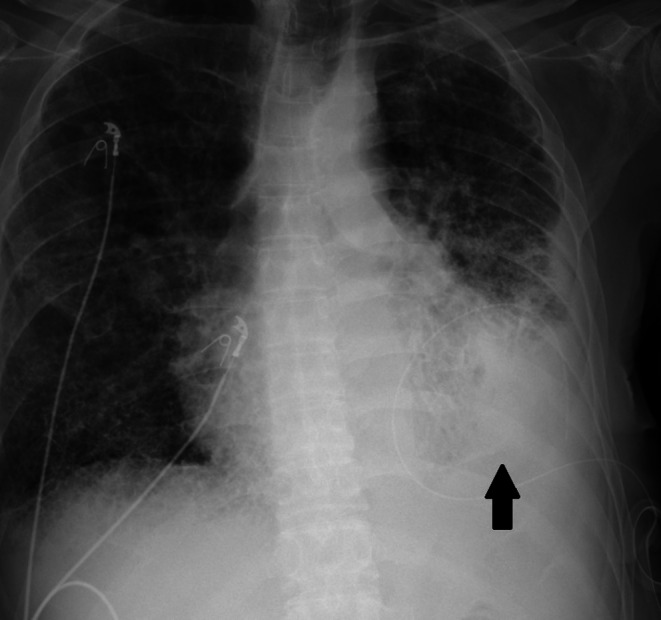 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleural and Pulmonary Diseases · Lung Cancer Diagnosis and Treatment · Trauma Management and Diagnosis
A 62‐year‐old male with a past medical history of metastatic adenocarcinoma of the lung complicated by recurrent malignant pleural effusion, emphysema, pulmonary fibrosis, and pulmonary hypertension presented with acute on chronic hypoxic respiratory failure. He had an indwelling left‐sided pleural catheter, from which he drained fluid three times a week. He required 4 L of oxygen at home. Due to hypoxia, he was placed on high‐flow nasal cannula. Chest x‐ray showed a large left‐sided pleural effusion, widespread coarsening of the interstitium, and emphysematous changes throughout both lungs (Figure 1). Almost half a liter of pleural fluid was drained daily for two days, and he was started on antibiotics for empyema due to gram‐positive cocci in the pleural fluid. On the third day, his pleural catheter was connected to a water seal, and he was able to be weaned down to his home oxygen requirements. A repeat x‐ray showed interval development of an area of trapped lung, pneumothorax ex vacuo, and hydropneumothorax (Figure 2). Repeated x‐rays showed stable size of trapped lung, and as he remained asymptomatic with no oxygen requirement beyond baseline, no surgical intervention was pursued.
Trapped lung occurs when the lung fails to fully re‐expand after pleural drainage due to the formation of a fibrous peel on the visceral pleura. This fibrous layer prevents normal apposition of the lung to the chest wall and is commonly associated with chronic inflammation from prior pneumonia, empyema, hemothorax, or malignancy [1]. A negative pressure gradient develops which draws air into the pleural space, causing a condition called pneumothorax ex vacuo. In contrast, iatrogenic pneumothorax typically results from direct pleural injury during procedures such as thoracentesis, central line placement, mechanical ventilation, or lung biopsy, which can introduce air into the pleural space [2]. It often requires chest tube drainage depending on size and symptoms. Both are important to distinguish as additional chest tubes in pneumothorax ex vacuo do not lead to re‐expansion of the lungs and can further worsen it.
Asymptomatic patients can be observed while symptomatic patients may benefit from surgical decortication to restore lung expansion. If the lung remains unexpandable, the pleural space may partially refill with fluid over time, leading to a hydropneumothorax. Most patients can be managed conservatively as long as they are clinically stable. In patients with underlying malignancy or chronic pleural disease, this condition often reflects advanced disease, and treatment goals should focus on symptom management and quality of life rather than aggressive interventions.
Author Contributions
Mashal Binte Ali: writing – original draft, writing – review and editing. Danish Jilani: writing – original draft, writing – review and editing. Meher Binte Ali: conceptualization, investigation, writing – original draft, writing – review and editing.
Funding
The authors have nothing to report.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. Feller‐Kopman , “Nonexpandable Lung: More Than Just a Call From Radiology,” Annals of the American Thoracic Society 16, no. 10 (2019): 1240–1242.31573341 10.1513/Annals ATS.201907-553ED · doi ↗ · pubmed ↗
- 2S. Siddiqui , U. Falak , and S. Navid , “Pneumothorax ex‐Vacuo or Trapped Lungs Appearing as Iatrogenic Hydropneumothorax: A Case Report and Review of Non‐Expandable Lungs (NEL),” Cureus 15, no. 7 (2023): e 41814, 10.7759/cureus.41814.37575695 PMC 10422936 · doi ↗ · pubmed ↗