Association of serum high creatinine-to-albumin ratio with increased 1-year mortality in older patients following hip fracture surgery
Peipei Jin, Jian Huang, Wei Yuan, Housheng Wang, Wubin Chen, Ling Chen, Wenbin Lu

TL;DR
High creatinine-to-albumin ratio in older patients after hip fracture surgery is linked to higher 1-year mortality.
Contribution
Identifies CAR as an independent predictor of 1-year mortality in older hip fracture patients.
Findings
High CAR was independently associated with increased 1-year mortality (HR = 1.49).
Kaplan–Meier analysis showed higher mortality in patients with high CAR (p < 0.0001).
The association remained consistent across all subgroups.
Abstract
Creatinine-to-albumin ratio (CAR) was associated with short-term and long-term prognosis in various clinical settings. However, the relation of CAR with prognosis in older patients with hip fracture remains unclear. This retrospective study was performed in older patients undergoing hip fracture surgery in our hospital from January 2018 to December 2023. Serum creatinine and albumin were recorded at admission. The primary outcome was 1-year mortality after surgery in patients with hip fracture. The association between preoperative serum creatinine-to-albumin ratio and 1-year mortality was assessed by Kaplan–Meier curves, Cox regression models, and stratified analyses. The mean age of the participants was 79.5 ± 8.1 years and the median CAR was 1.9 (1.5–2.4). The prevalence of 1-year mortality following hip fracture surgery was 8.6%. Multivariate Cox regression analysis indicated that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
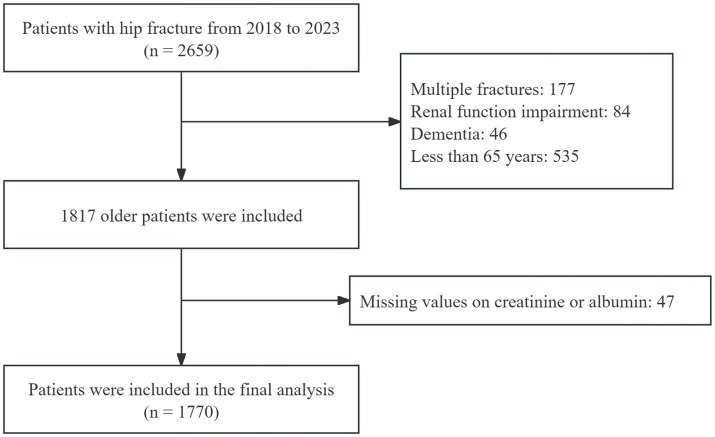 Figure 1
Figure 1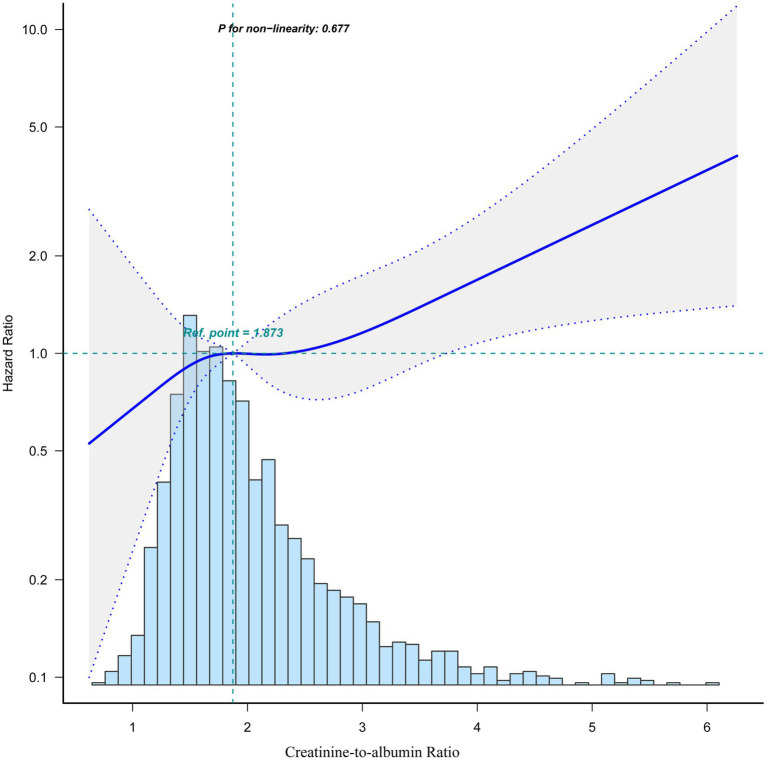 Figure 2
Figure 2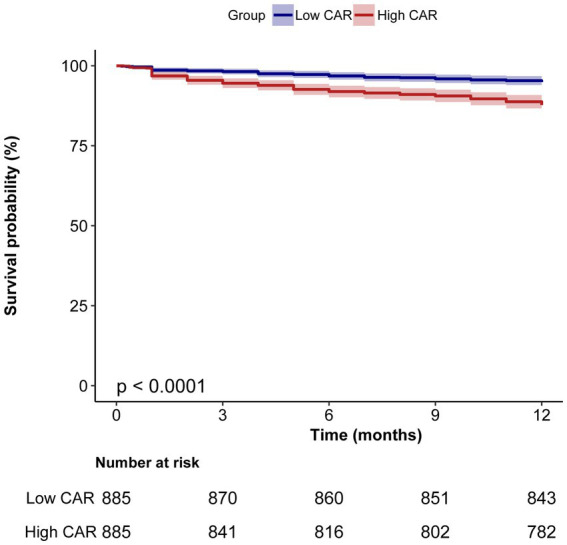 Figure 3
Figure 3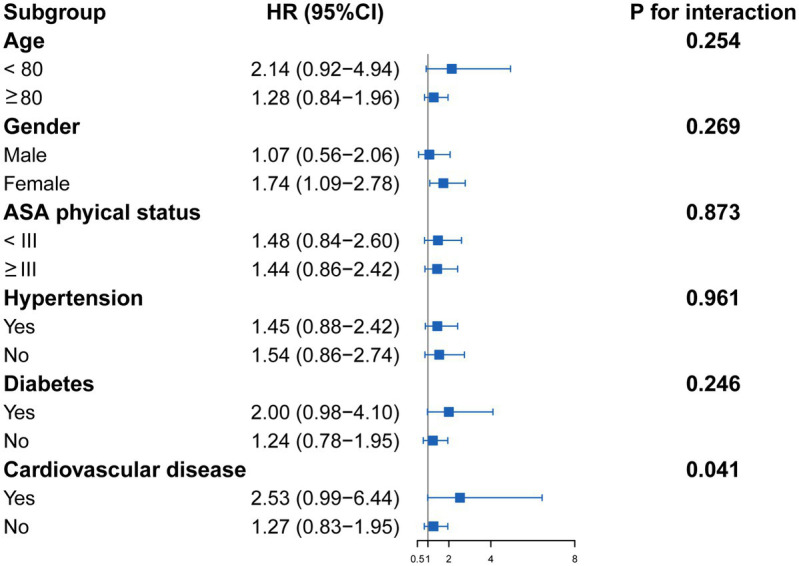 Figure 4
Figure 4| Variables | Total ( | Survival group ( | Death group ( |
|
|---|---|---|---|---|
| Age (years) | 79.4 ± 8.1 | 78.8 ± 7.9 | 85.5 ± 7.5 | <0.001 |
| Gender | 0.028 | |||
| Male | 555 (31.4) | 495 (30.6) | 60 (39.2) | |
| Female | 1,215 (68.6) | 1,122 (69.4) | 93 (60.8) | |
| BMI (kg/m2) | 22.4 ± 3.7 | 22.5 ± 3.7 | 21.4 ± 3.8 | <0.001 |
| ASA physical status | <0.001 | |||
| <III | 1,068 (60.3) | 999 (61.8) | 69 (45.1) | |
| ≥III | 702 (39.7) | 618 (38.2) | 84 (54.9) | |
| Anesthesia | 0.558 | |||
| General anesthesia | 283 (16.0) | 256 (15.8) | 27 (17.6) | |
| Spinal anesthesia | 1,487 (84.0) | 1,361 (84.2) | 126 (82.4) | |
| Type of fracture | 0.266 | |||
| Femoral neck fractures | 955 (54.0) | 879 (54.4) | 76 (49.7) | |
| Intertrochanteric fractures | 815 (46.0) | 738 (45.6) | 77 (50.3) | |
| Type of surgery | 0.288 | |||
| Total hip arthroplasty | 214 (12.1) | 202 (12.5) | 12 (7.8) | |
| Hemiarthroplasty | 546 (30.8) | 496 (30.7) | 50 (32.7) | |
| Proximal femoral nail | 770 (43.5) | 697 (43.1) | 73 (47.7) | |
| Open reduction and internal fixation | 240 (13.6) | 222 (13.7) | 18 (11.8) | |
| Alcohol history | 29 (1.6) | 27 (1.7) | 2 (1.3) | 1 |
| Smoking history | 62 (3.5) | 60 (3.7) | 2 (1.3) | 0.122 |
| Hypertension | 973 (55.0) | 889 (55) | 84 (54.9) | 0.986 |
| Diabetes | 493 (27.9) | 446 (27.6) | 47 (30.7) | 0.408 |
| Cardiovascular disease | 406 (22.9) | 364 (22.5) | 42 (27.5) | 0.165 |
| Cerebrovascular disease | 272 (15.4) | 237 (14.7) | 35 (22.9) | 0.007 |
| Lung disease | 156 (8.8) | 127 (7.9) | 29 (19) | <0.001 |
| Cancer | 49 (2.8) | 40 (2.5) | 9 (5.9) | 0.033 |
| Time to admission (h) | 20.0 (6.5–48.0) | 19.5 (6.0–48.0) | 24.0 (10.0–72.0) | 0.007 |
| Creatinine (μmol/L) | 66.0 (56.0–82.0) | 66.0 (56.0–81.0) | 71.0 (60.0–90.0) | 0.002 |
| Albumin (g/L) | 36.0 (33.0–39.0) | 36.0 (33.0–39.0) | 33.0 (30.0–35.0) | <0.001 |
| CAR | 1.9 (1.5–2.4) | 1.8 (1.5–2.3) | 2.2 (1.8–2.9) | <0.001 |
| LDH (U/L) | 221.0 (190.0–257.0) | 220.0 (190.0–256.0) | 228.0 (197.0–274.0) | 0.041 |
| Glucose (mmol/L) | 6.7 (5.7–8.4) | 6.7 (5.7–8.3) | 6.7 (5.8–9.6) | 0.283 |
| D-dimer (mg/L) | 3.7 (1.8–8.3) | 3.6 (1.7–8.4) | 3.9 (2.5–7.5) | 0.166 |
| APTT (s) | 36.8 (33.3–40.5) | 36.8 (33.4–40.3) | 36.5 (33.2–42.0) | 0.480 |
| INR | 1.1 (1.0–1.1) | 1.1 (1.0–1.1) | 1.1 (1.1–1.2) | <0.001 |
| Hemoglobin (g/L) | 115.0 (101.0–128.0) | 115.0 (102.0–129.0) | 103.0 (89.0–123.0) | <0.001 |
| Lymphocytes (109/L) | 1.0 (0.8–1.4) | 1.1 (0.8–1.4) | 0.9 (0.6–1.2) | <0.001 |
| Monocytes (109/L) | 0.6 (0.4–0.8) | 0.6 (0.4–0.8) | 0.6 (0.4–0.8) | 0.432 |
| Neutrophils (109/L) | 6.4 (4.9–8.1) | 6.3 (4.9–8.0) | 7.1 (5.3–9.2) | <0.001 |
| Platelets (109/L) | 177.0 (138.0–218.0) | 177.0 (138.0–218.0) | 186.0 (150.0–224.0) | 0.061 |
| Variable | Model I | Model II | Model III | Model IV | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| HR (95% CI) |
| HR (95% CI) |
| |
| CAR | 1.67 (1.43–1.94) | <0.001 | 1.33 (1.10–1.61) | 0.003 | 1.33 (1.10–1.61) | 0.003 | 1.30 (1.07–1.58) | 0.009 |
| Low CAR | Rf | Rf | Rf | Rf | ||||
| High CAR | 2.50 (1.77–3.55) | <0.001 | 1.50 (1.04–2.18) | 0.032 | 1.49 (1.03–2.17) | 0.035 | 1.49 (1.02–2.17) | 0.039 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Inflammatory Biomarkers in Disease Prognosis · Cardiac, Anesthesia and Surgical Outcomes
Introduction
1
With the acceleration of global population aging, the incidence of hip fractures in the older individuals is on the rise, becoming a significant public health issue (1, 2). Hip fractures are one of the most common injuries in the older patients, with poor prognosis, high complication rates, and a 1-year mortality rate of up to 15–25% (3, 4), which put unprecedented demands on healthcare infrastructure. In this context, identifying factors associated with postoperative mortality is critical to improve risk stratification and guide personalized treatment strategies.
Previous studies have shown that inflammation, malnutrition, and renal function impairment were related with poor prognosis after surgery (5–7). Accumulating evidence has shown that creatinine-to-albumin ratio (CAR), a biomarker that integrates renal function, inflammation and nutrition, was associated with short-term and long-term prognosis in patients with acute coronary syndrome, diabetes and inflammatory diseases (8–10). In addition, recently, a retrospective cohort study indicated that increased CAR can serve as a risk factor for 28-day mortality in patients undergoing cardiac surgery (11). Furthermore, a prospective cohort study showed that CAR was related to 1-year mortality after surgery in patients with non-ST-elevation acute coronary syndrome (12). However, the association between CAR and mortality in older patients following hip fracture surgery has not been investigated.
Therefore, we hypothesized that serum CAR levels were associated with 1-year mortality after surgery in older patients with hip fractures. Our study provided a new insight to identify risk factors for mortality after surgery and optimize personalized care pathways for older patients with hip fractures.
Materials and methods
2
Study design and population
2.1
This retrospective observational study was performed in patients undergoing hip fracture surgery in our hospital from January 2018 to December 2023. This study was conducted in line with the Declaration of Helsinki and was approved by the ethical review committee in our hospital (CHEC2024-257). Due to the retrospective collection of de-identified clinical data from patients, informed consent was waived by the ethical review committee in our hospital.
Older adults with hip fracture (including femoral neck fractures and intertrochanteric fractures) who underwent surgery were eligible for study enrollment. Exclusion criteria included multiple fractures, renal function impairment, dementia, and age <65 years old. We also excluded patients with missing values on creatinine or albumin. Renal function impairment was defined according to an estimated glomerular filtration rate <60 mL/(min × 1.73 m^2^) using the Chinese-based equation (13).
Variables
2.2
We selected the variables based on existing literature and clinical practice (14, 15). Data regarding age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification, type of anesthesia, alcohol history, smoking history, time to admission (time from injury to admission) and medical history were recorded in this study. Medical history included hypertension, diabetes, cardiovascular disease, cerebrovascular disease, lung disease, and cancer. In addition, creatinine, albumin, lactate dehydrogenase (LDH), glucose, D-dimer, activated partial thromboplastin time (APTT), international normalized ratio (INR), hemoglobin, lymphocyte, monocyte, neutrophil, and platelet were recorded at admission. The CAR was calculated as preoperative creatinine (μmol/L)/albumin (g/L). We employed multiple imputation to address variables with missing values <10%, with exception of CAR.
Outcome
2.3
The primary endpoint was 1-year mortality after surgery in older patients with hip fracture.
Statistical analysis
2.4
Participants were divided into two groups based on their survival status. Continuous variables with normally distributed data were presented as mean ± SD and were compared using Student’s t-test. Mann–Whitney U-test was used to compare continuous variables in non-normal distribution data described as medians (quartiles). Categorical variables were presented as frequencies (%) and analyzed using χ^2^ test.
The CAR levels were categorized as low CAR (<1.9) or high CAR (≥1.9), based on the median. Kaplan–Meier survival curves with log-rank testing were constructed to compare cumulative survival probabilities across low and high CAR groups. Dose–response relationship between CAR and 1-year mortality was assessed by the restricted cubic splines. We used multivariate Cox proportional hazard models to evaluate the association of CAR with 1-year mortality after surgery when CAR were both continuous and binary variables.
Variates with a p-value of <0.05 in the comparison of baseline characteristics between survival and death group were incorporated into multivariate models for covariate adjustment. In Model I, no covariates were adjusted. Model II was adjusted for age, gender, and BMI. Model III was adjusted for model II plus ASA physical status, time to admission, cerebrovascular disease, lung disease and cancer. In the model IV, LDH, INR, hemoglobin, lymphocyte count and neutrophil count were further adjusted.
Stratified and interaction analyses were performed, considering age (<80 years or ≥80 years), gender (male or female), ASA physical status (<III or ≥III), and the presence or absence of hypertension, diabetes, and cardiovascular disease. For each stratification, adjustments were made for potential confounders, including age, gender, BMI, ASA physical status, time to admission, cerebrovascular disease, lung disease, cancer, LDH, INR, hemoglobin, lymphocyte count, and neutrophil count, with exception of the stratification factor itself. The R software packages (The R Foundation)1 and Free Statistics software versions 1.7.1 were used to perform all statistical analyses. A p-value of less than 0.05 was considered to indicate statistical significance.
Results
3
In total, 2,659 patients underwent hip fracture surgery were identified. After excluding 889 patients (177 had multiple fractures, 84 had renal function impairment, 46 had dementia, 535 were under the age of 65 years, and 47 had missing data on creatinine or albumin), the final data analysis included 1770 patients. The participant flow diagram is shown in Figure 1.
Flowchart of the study population selection process.
Participants characteristics
3.1
Table 1 shows the baseline information for all patients. The mean age of the study patients was 79.4 ± 8.1 years. The median baseline CAR was 1.9 (1.5–2.4); 1-year mortality rate after hip fractures surgery was 8.6% in older patients. Compared with survival group, patients in death group were older, predominantly male, had lower BMI, higher ASA physical status, and longer time from injury to admission (all p < 0.05). Additionally, patients with cerebrovascular disease, lung disease or cancer were more likely to experience 1-year mortality. In terms of laboratory parameters, patients in the death group exhibited lower levels of albumin, hemoglobin, and lymphocytes, while having higher levels of creatinine, CAR, LDH, INR, and neutrophils compared with those in the survival group (all p < 0.05).
Relationship between CAR and mortality after surgery
3.2
Figure 2 shows the linear relationship between CAR and 1-year mortality after surgery in older patients with hip fracture. Kaplan–Meier survival analysis further revealed that patients in the low CAR group had better survival probabilities compared to those in the high CAR group (p < 0.0001; Figure 3). Moreover, multivariate Cox regression analysis showed that a high CAR was independently related to increased 1-year mortality regardless of continuous variable [hazard ratio (HR) = 1.30, 95% confidence interval (CI) = 1.07–1.58] or categorical variable [HR = 1.49, 95% CI = 1.02–2.17] in the adjusted model (Table 2).
Dose–response relationship between CAR and 1-year mortality following hip fracture surgery by smooth curve fitting. Data were fit by a Cox proportional hazard regression model based on restricted cubic splines. CAR was entered as continuous variable. Data were adjusted for the factors (age, gender, BMI, ASA physical status, time to admission, cerebrovascular disease, lung disease, cancer, LDH, INR, hemoglobin, lymphocyte count and neutrophil count). The curves line and shaded areas around depict the estimated values and their corresponding 95% confidence intervals. The histogram depicts the distribution of the CAR. BMI, body mass index; ASA, American Society of Anesthesiologists; LDH, lactate dehydrogenase; INR, international normalized ratio; CAR, creatinine-to-albumin ratio.
Kaplan–Meier survival curves of 1-year mortality for patients with hip fracture surgery.
Subgroup analysis
3.3
Subgroup analysis showed that there was an interaction (p for interaction = 0.041) between cardiovascular disease and CAR on 1-year mortality. In addition, patients with high CAR generally exhibited a higher risk of 1-year mortality than those who had low CAR in all subgroups. Moreover, the association remained significant (HR = 1.74, 95% CI = 1.09–2.78) in female patients with hip fracture (Figure 4).
Forest plots of subgroup analysis of the relationship between CAR and 1-year mortality in patients with hip fracture surgery. Low CAR was the reference for high CAR. Each stratification adjusted for the factors (age, gender, BMI, ASA physical status, time to admission, cerebrovascular disease, lung disease, cancer, LDH, INR, hemoglobin, lymphocyte count, and neutrophil count) in the multivariable Cox regression, except for the stratification factor itself. BMI, body mass index; ASA, American Society of Anesthesiologists; LDH, lactate dehydrogenase; INR, international normalized ratio; CAR, creatinine-to-albumin ratio; HR, hazard ratio; CI, confidence interval.
Discussion
4
This retrospective study included 1,770 older patients who underwent hip fracture surgery, with a 1-year mortality rate after surgery of 8.6%. Kaplan–Meier survival analysis indicated that patients with low CAR exhibited a high 1-year survival rate after surgery. In addition, multivariate Cox regression analysis revealed that high level of CAR was independently associated with increased 1-year mortality after hip fracture surgery. Furthermore, we found that the association remained consistent across all subgroups.
Increasing evidence shows that advanced age, low BMI, comorbidities, and prolonged time from injury to admission, have been identified as significant risk factors for increased mortality in patients with hip fracture (16–19). In addition, previous evidence has shown that peripheral blood inflammatory markers and nutritional indicators are related to prognosis in many clinical settings (20, 21). This is consistent with our findings. Moreover, we found that patients with high CAR had a high 1-year mortality rate after surgery.
Serum creatinine was used as a predictor for renal clearance capacity, which was associated with short- and long-term morbidity and mortality in patients with critical illness and cardiovascular disease (22, 23). Previous study has shown that elevated creatinine was associated with all-cause, cardiovascular and cancer mortality of American adults in a nationwide cohort study (24). In addition, a retrospective cohort study indicated that high level of creatinine was associated with an increased risk of mortality in patients undergoing surgery (25). Consistent with previous studies, we found that patients with 1-year mortality after surgery had a high level of serum creatinine.
Albumin is an important serum protein and has a wide range of physiological functions, such as immune regulation, endothelial stabilization, antioxidant effects (26–28). Besides, albumin can also be used as a biomarker for prognosis in many diseases, including inflammatory diseases, cancer, and hip fracture (29-31). Recent study showed that hypoalbuminemia was linked to poor postoperative recovery and increased mortality (32), which was similar with our study.
The CAR, as a comprehensive indicator, can more comprehensively reflect the metabolism, inflammation and nutritional status of patients, and is more closely related to the pathological and physiological characteristics in various clinical settings. Growing studies have reported that high level of CAR was linked to poor outcomes in patients with sepsis and acute pancreatitis (33, 34). In our study, we demonstrated the association of high CAR with increased 1-year mortality after hip fracture surgery in older patients. However, the definite causes and pathophysiological mechanisms underlying the relationship between CAR and a poor prognosis remain unclear. High CAR signifies a baseline state of elevated inflammation, coupled with probable muscle wasting and nutritional deficit, which cumulatively contribute to frailty and reduced physiological reserve after surgery in older patients with hip fracture.
We also found an interaction between cardiovascular disease and CAR on 1-year mortality. The association appeared substantially stronger in patients with cardiovascular disease (HR = 2.53), although the estimate was imprecise with a wide confidence interval (0.99–6.44). This imprecision is likely due to the limited sample size within the cardiovascular disease stratum. Biologically, this interaction may indicate that the inflammatory burden reflected by CAR synergizes with the compromised cardiovascular reserve in patients with cardiovascular disease, leading to a higher risk of mortality.
This study had several strengths. To our knowledge, it is the first large-scale retrospective study to examine the association between CAR and 1-year mortality in older patients undergoing hip fracture surgery. Second, the robustness of our findings was enhanced by comprehensive multivariable adjustments for potential confounders, minimizing selection bias and residual confounding. Third, subgroup analyses confirmed the consistency of our primary findings across different patient subgroups.
However, this study also had limitations. First, as a single-center retrospective study, the generalizability and causal relationship of our findings may be constrained. Second, despite rigorous statistical adjustments, unmeasured confounders such as variations in clinical care, postoperative complications, and socioeconomic factors could have influenced the observed association. Third, we excluded the patients with eGFR<60 mL/(min × 1.73 m^2^), limiting the generalizability of findings to patients with moderate-to-severe pre-existing kidney disease. Finally, the CAR levels were measured preoperatively but not tracked postoperatively, limiting insights into dynamic changes influencing outcomes. Therefore, multicenter studies with larger cohorts are needed to conform the association.
Conclusion
5
Our study demonstrated that high CAR was associated with increased 1-year mortality in older patients undergoing hip fracture surgery. Preoperative CAR could be a simple and effective strategy to flag patients at high risk for complications and poor recovery after surgery. However, multicenter, prospective studies are needed to validate these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rhayem C Ghosn A Issa ZA Alwan JS Dimassi H Haidar R . Secular trends in hip fracture mortality and predictors of mortality from the NSQIP database. J Clin Endocrinol Metab. (2025) 110:3210–9. doi: 10.1210/clinem/dgaf 087, 39980170 PMC 12527425 · doi ↗ · pubmed ↗
- 2Viamont-Guerra MR Guimarães R Bridges C Antonioli E Lenza M. Ultra-early versus early surgery for hip fracture. Cochrane Database Syst Rev. (2024) 6:Cd 015697. doi: 10.1002/14651858.cd 015697, 39804112 PMC 11170678 · doi ↗ · pubmed ↗
- 3Salis F Buffoli I Belfiori M Bellisai A Gianoglio B Marongiu G . Handgrip strength as a predictor of one-year mortality in elderly patients with fragility hip fracture. Aging Clin Exp Res. (2025) 37:112. doi: 10.1007/s 40520-025-03019-2, 40172770 PMC 11965246 · doi ↗ · pubmed ↗
- 4Sundet M Martinsen M Paus M Valland H Halvorsen HH Sexton J . Predictors of 1-year mortality in a clinical cohort of hip fracture patients. Eur J Trauma Emerg Surg. (2025) 51:147. doi: 10.1007/s 00068-025-02812-y, 40111487 PMC 11925984 · doi ↗ · pubmed ↗
- 5Meermans G van Egmond JC. Malnutrition in older hip fracture patients: prevalence, pathophysiology, clinical outcomes, and treatment-a systematic review. J Clin Med. (2025) 14:5662. doi: 10.3390/jcm 14165662, 40869488 PMC 12386537 · doi ↗ · pubmed ↗
- 6Shan X Littlejohn JE Peng K Ji F Liu H. The effect of perioperative AKI on surgical outcomes. Anesthesiol Perioper Sci. (2023) 1:28. doi: 10.1007/s 44254-023-00032-4, 39877395 PMC 11774244 · doi ↗ · pubmed ↗
- 7Wu L Li Y Li L Pan G You Y Chen X . Postoperative serum NLRP 1 as a biochemical predictor of delirium and cognitive decline after hip fracture surgery in elderly patients: a single Center observational study. Clin Interv Aging. (2025) 20:2005–17. doi: 10.2147/cia.s 556318, 41255934 PMC 12621587 · doi ↗ · pubmed ↗
- 8Dai H Liu L Xu W. Association of albumin-to-creatinine ratio with diabetic retinopathy among US adults (NHANES 2009-2016). Endocrinol Diabetes Metab. (2025) 8:e 70029. doi: 10.1002/edm 2.70029, 39826101 PMC 11742259 · doi ↗ · pubmed ↗