A rare co-occurrence of hidradenocarcinoma and squamous cell carcinoma in situ on the left posterior calf treated with Mohs micrographic surgery
Randy W. Head, Conner M. Bacon, Richard Jahan-Tigh, Caitlin G. Robinson

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
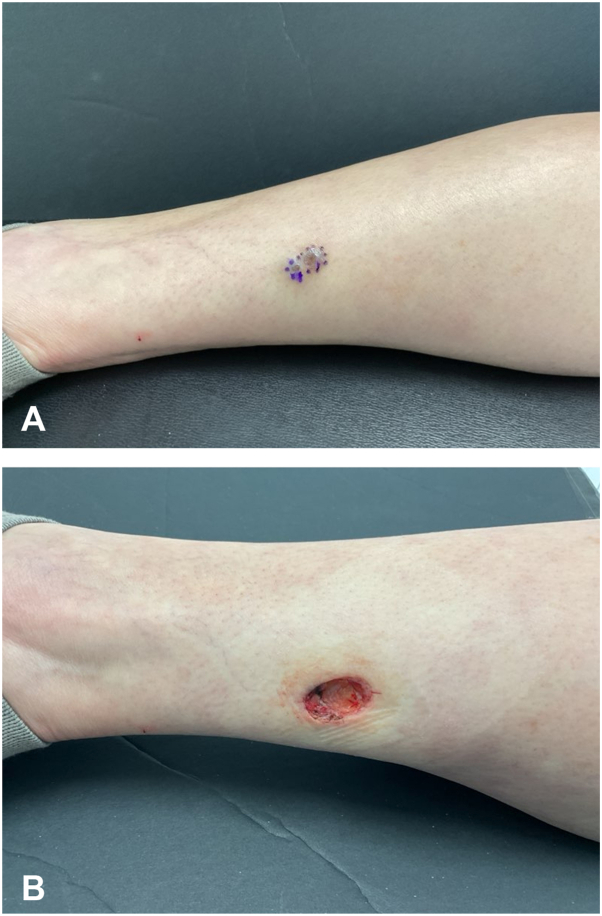 Figure 1
Figure 1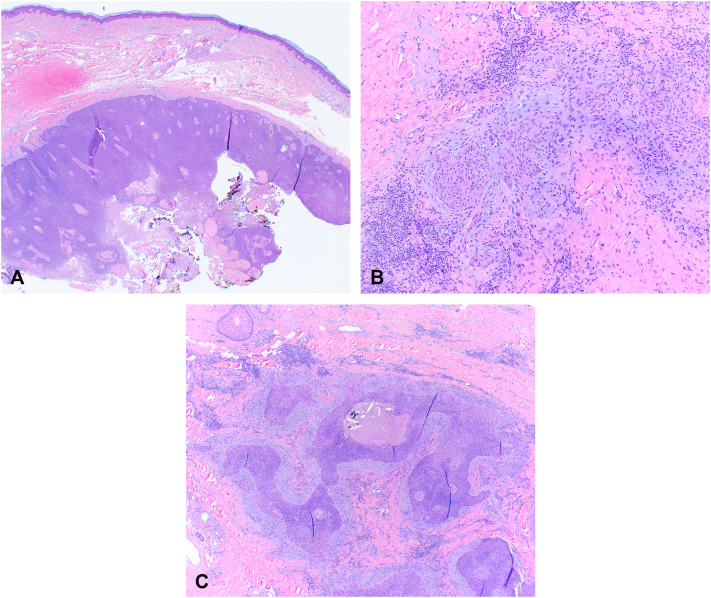 Figure 2
Figure 2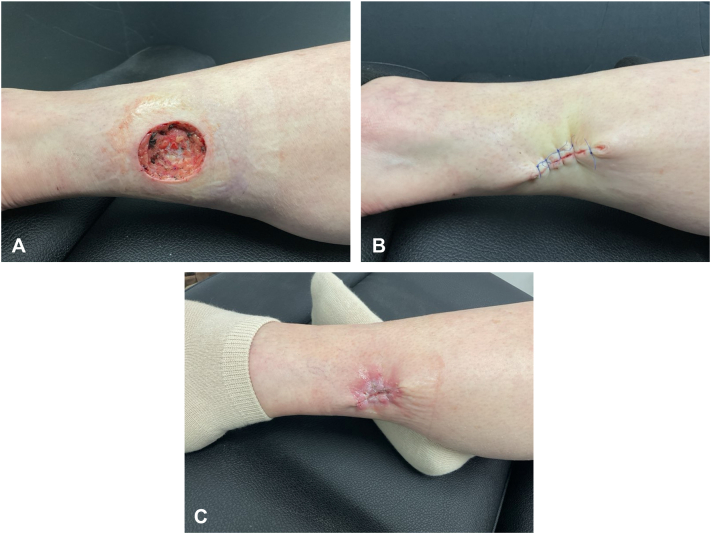 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Salivary Gland Tumors Diagnosis and Treatment · Cancer Diagnosis and Treatment
Introduction
Hidradenocarcinoma is a rare, malignant tumor of eccrine sweat glands, accounting for 6% of eccrine tumors and 0.001% of all tumors.1 Cases have been described in a wide range of ages and different anatomic sites, but are most commonly found on the face and extremities.2 In a recent study, the current 10-year overall survival rate is estimated to be 60.2%, with a high likelihood of the tumor metastasizing to distant sites.3 Diagnosing and distinguishing this cancer from its benign counterpart, hidradenoma, can be challenging for physicians from both a clinical and histologic perspective.4 Clinically, the tumor typically presents as a slow-growing, painless, firm nodule that can secrete serosanguineous fluid.1 Upon gross examination, these lesions may appear well circumscribed, but the malignant features become clear histologically. Key features include asymmetry and infiltrative growth into the dermis or subcutaneous fat, pleomorphism and necrosis. Additionally, these tumors often contain mixed epithelial cell types, including squamous, mucinous, and clear cells containing glycogen, ductal structures, and cyst formation. At higher magnification, multinodular infiltrative nests of atypical cells support the diagnosis of hidradenocarcinoma.2 Currently, there are no established guidelines for the treatment of this tumor.4 Most recommendations suggest wide local excision as the primary treatment option.2^,^5 However, in the right clinical setting, Mohs micrographic surgery could be considered.5 In the following case, a rare occurrence of hidradenocarcinoma associated with squamous cell carcinoma in situ (SCCIS) is successfully treated with Mohs micrographic surgery.
Case
A 68-year-old female presented for Mohs surgery of a biopsy-proven SCCIS located on the left posterior calf. Upon examination, 2 <1 cm pigmented nodules adjacent to the prior biopsy site were noted (Fig 1, A). Various treatment options were discussed for the SCCIS. These treatments included Mohs surgery, excisional surgery, radiation therapy, and various topical therapies. The patient was assigned a Mohs appropriate use criteria score of 6, indicating that additional information and physician judgment were required to determine appropriateness of Mohs surgery. Given the size greater than 1 cm and nodular appearance, it was decided to proceed with Mohs surgery (Fig 1, B).Fig 1A, Marked 1.7 × 1.0 cm lesion prior to first Mohs surgery. B, Postoperative excision site with a diameter of 1.9 × 1.2 cm and margins of 0.1 cm.
Due to the presence of the 2 pigmented nodules adjacent to the Mohs site, the lesion was debulked, and the debulked tissue was processed for evaluation along with the first Mohs layer. Upon interpretation of the Mohs slides, both the debulk and the first layer revealed a dermal mass consisting of monomorphic, basaloid cells. Due to the unexpected histology, Mohs surgery was paused, and the specimens (both the central debulk and first Mohs layer) were submitted for permanent sectioning and dermatopathological evaluation. The permanent section pathology resulted as hidradenocarcinoma. The diagnosis was rendered using morphology on hematoxylin and eosin stain. No immunohistochemical stains were used (Fig 2). Because the histology of the lesion was easily recognizable to the Mohs surgeon and debulk histology was available to be viewed for comparison, it was decided to continue with the original plan for Mohs surgery. The following week, Mohs surgery was continued. An initial margin of 0.5 cm was taken around the prior surgical site (Fig 3, A). Utilizing hematoxylin and eosin stains, frozen section analysis showed no evidence of residual tumor at the margin after 1 Mohs layer.Fig 2H&E sections show a dermal basaloid neoplasm with ductal differentiation, mucin production, and thickened hyalinized basement membrane material. Some parts of the tumor are cytologically atypical, glassy, and have nuclear pleomorphism. Melanin pigment is scattered throughout the neoplasm. A, 20× magnification. B, and C, 40× magnification. H&E, Hematoxylin and eosin.Fig 3A, Final Mohs surgery site with a final defect size of 3.5 × 3.0 cm. B, Suture site with intermediate purse string closure. C, Postoperative site 2 weeks postsurgery, showing proper healing and granulation.
Surgical repair was performed using a purse-string intermediate closure due to the inelasticity of the skin as well as the location of the wound in an area of active movement. The final wound length was 3.5 cm (Fig 3, B), and the patient was scheduled to return for a wound check and suture removal in 14 days. At the time of suture removal, the wound was well-healed (Fig 3, C). At her 1-month follow-up, the patient underwent ultrasound imaging of her inguinal lymph nodes to rule out regional metastasis, which demonstrated no abnormal findings. At the patient’s 6-month follow-up, there was no evidence of recurrence. She is scheduled to return for a 12-month follow-up for her final dermatologic evaluation. The patient will continue long-term surveillance with oncology.
Discussion
Hidradenocarcinoma is a malignant cutaneous neoplasm derived from the eccrine sweat glands. Sweat gland tumors are challenging to diagnose due to the morphologic overlap with other benign neoplasms.6 The incidence is similar between men and women and is most commonly diagnosed in patients between the ages of 50 and 70.2 In most cases, patients remain asymptomatic other than general pain, occasional bleeding, and discomfort from the site of the lesion. However, the tumor can metastasize, primarily involving regional lymph nodes, bones, and the skin. Though the literature is limited and cases are exceedingly rare, this tumor has an estimated recurrence rate of 60% and a 50% metastasis rate.7
After a review of the literature using the terms “hidradenocarcinoma,” “malignant clear cell hidradenoma,” “SCCIS,” and “Bowen’s disease,” no prior case of hidradenocarcinoma and SCCIS at the same anatomic site was identified. In addition to the rarity of this copresentation, our case highlights the use of Mohs surgery in discovering a more concerning malignant tumor underlying a biopsy-proven SCCIS. Had the lesion been treated with topical therapeutics or superficial destruction alone, the deeper, underlying aggressive malignancy could have been missed. This case demonstrates how important it is for providers to better investigate atypical presentations and shows how beneficial the histological assessment during Mohs surgery is in detecting unexpected neoplasms. Due to their aggressive nature, hidradenocarcinomas require timely diagnosis and treatment. Our findings also demonstrate how Mohs surgery could be considered as primary treatment due to the tumor’s recognizability on frozen sections and lack of need for special stains. A debulk section or review of initial biopsy slides could be useful to review in preparation for Mohs surgery. Further studies are needed to establish efficacy of Mohs surgery for hidradenocarcinoma. This case adds to the literature by documenting a previously unreported co-occurrence of hidradenocarcinoma and SCCIS at the same anatomic site, as well as the advantages of Mohs surgery in detecting and treating these rare presentations.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coco D.Leanza S.Campagnacci R.Clear cell hidradenocarcinoma: a rare identity difficult to recognize - case report and review of the literature Maedica (Bucur)163202152653010.26574/maedica.2020.16.3.52634925613 PMC 8643562 · doi ↗ · pubmed ↗
- 2Gauerke S.Driscoll J.J.Hidradenocarcinomas: a brief review and future directions Arch Pathol Lab Med 1345201078178510.5858/134.5.78120441512 · doi ↗ · pubmed ↗
- 3Gao T.Pan S.Li M.Su R.Prognostic analysis of hidradenocarcinoma: a SEER-Based observational study Ann Med 541202245446310.1080/07853890.2022.203231335107407 PMC 8812755 · doi ↗ · pubmed ↗
- 4Khan B.M.Mansha M.A.Ali N.Hidradenocarcinoma: five years of local and systemic control of a rare sweat gland neoplasm with nodal metastasis Cureus 162018 e 228410.7759/CUREUS.2884 PMC 611041230155386 · doi ↗ · pubmed ↗
- 5Soni A.Bansal N.Kaushal V.Chauhan A.K.Current management approach to hidradenocarcinoma: a comprehensive review of the literature Ecancermedicalscience 9201551710.3332/ecancer.2015.51725815059 PMC 4370612 · doi ↗ · pubmed ↗
- 6Van Der Horst M.P.J.Brenn T.Update on malignant sweat gland tumors Surg Pathol Clin 102201738339710.1016/j.path.2017.01.01028477887 · doi ↗ · pubmed ↗
- 7Tumors with Eccrine Differentiation Elder D.E.Elenitsas R.Johnson B.L.Murphy G.F.Lever's Histopathology of the Skin 9th ed 2005 Wolters Kluwer 898910