Helicobacter pylori infection, atrophic gastritis, and disabling dementia: the Japan Public Health Center-based Prospective Study
Takashi Matsunaga, Kazumasa Yamagishi, Hiroyasu Iso, Nobufumi Yasuda, Manami Inoue, Shoichiro Tsugane, Norie Sawada

TL;DR
This study finds that Helicobacter pylori infection and atrophic gastritis may increase dementia risk, especially when vitamin B12 intake is low.
Contribution
The study identifies a synergistic effect of H. pylori infection, atrophic gastritis, and low vitamin B12 intake on dementia risk.
Findings
H. pylori infection and severe atrophic gastritis are linked to higher dementia risk in low vitamin B12 consumers.
Combined H. pylori infection and AG increase dementia risk among individuals with low vitamin B12 intake.
No significant association was found in individuals with higher vitamin B12 intake.
Abstract
A meta-analysis reported a positive association between Helicobacter pylori (H. pylori) infection and dementia incidence. H. pylori infection leads to atrophic gastritis (AG) and affects the absorption of nutrients needed for nerve growth, such as vitamin B12 and folate. We aimed to clarify the associations of H. pylori IgG titer, AG, and their combination with disabling dementia incidence and to examine the interaction with vitamin B12 and folate. Anti-H. pylori immunoglobulin G (IgG) titer and pepsinogen levels were measured in 6,817 participants in 1993 (40–69 years), and the incidence of disabling dementia was followed during a median follow-up of 11.0 years. Associations of anti-H. pylori IgG titer, AG, and their combination with disabling dementia were examined using a multivariable-adjusted Cox proportional hazard model, with stratified analyses by dietary intake of vitamin B12…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
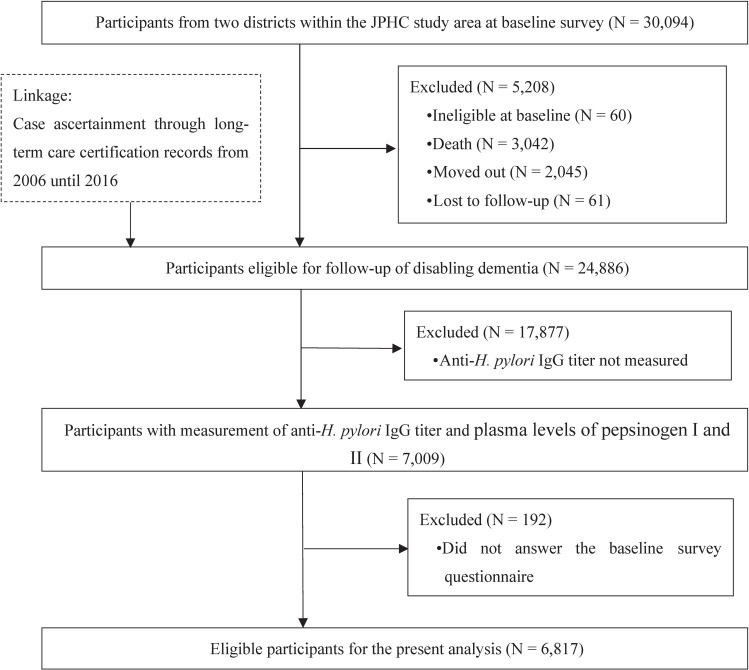 Fig. 1
Fig. 1|
|
| ||
|
| |||
|
|
|
| |
| Number of participants | 1,427 | 560 | 4,830 |
| Age (years), mean (SD) | 68.0 (8.9) | 70.3 (8.3) | 69.9 (8.3) |
| Males, n (%) | 348 (24.4) | 164 (29.3) | 1,597 (33.1) |
| Area, n (%) | |||
| Ibaraki | 835 (58.5) | 389 (69.5) | 3,315 (68.6) |
| Kochi | 592 (41.5) | 171 (30.5) | 1,515 (31.4) |
| Occupation, n (%) | |||
| Full-time agriculture/forestry/fishery | 360 (25.2) | 152 (27.1) | 1,258 (26.5) |
| Full-time hired/self-employed/professional | 374 (26.2) | 123 (22.0) | 1,217 (25.2) |
| Missing | 7 (0.5) | 8 (1.4) | 52 (1.1) |
| Smoking status (pack-years), n (%) | |||
| >30.0 pack-years | 99 (6.9) | 54 (9.6) | 495 (10.3) |
| Missing | 8 (0.6) | 4 (0.7) | 31 (0.6) |
| Alcohol consumption, n (%) | |||
| ≥450 g/week | 101 (7.1) | 37 (6.6) | 355 (7.4) |
| Missing | 1 (0.1) | 3 (0.5) | 16 (0.3) |
| Body Mass Index, n (%) | |||
| 25.0–29.9 | 325 (22.8) | 124 (22.1) | 1138 (23.6) |
| ≥30.0 | 42 (2.9) | 13 (2.3) | 95 (2.0) |
| Missing | 11 (0.8) | 11 (2.0) | 45 (0.9) |
| Frequency of leisure-time physical activity, n (%) | |||
| Almost everyday | 76 (5.3) | 34 (6.1) | 275 (5.7) |
| Missing | 19 (1.3) | 4 (0.7) | 66 (1.4) |
| Living alone, n (%) | |||
| Yes | 37 (2.6) | 16 (2.9) | 136 (2.8) |
| Missing | 10 (0.7) | 4 (0.7) | 33 (0.7) |
| History of cardiovascular disease, n (%) | 36 (2.5) | 20 (3.6) | 109 (2.3) |
| History of diabetes, n (%) | 68 (4.8) | 46 (8.2) | 248 (5.1) |
| History of hypertension, n (%) | 294 (20.6) | 123 (22.0) | 1,114 (23.1) |
| Vitamin B12 intake (µg/day), median (IQR) | 5.1 (3.5–7.1) | 5.0 (3.6–7.1) | 5.1 (3.6–7.1) |
| Folate intake (µg/day), median (IQR) | 260.3 | 282.9 | 273.1 |
|
|
|
|
|
|
|
| All participants | <10 | 1,987 | 18,506 | 349 | Reference |
| ≥10 | 4,830 | 44,269 | 976 | 1.04 (0.92–1.17) | |
| ≤3 | 1,427 | 13,494 | 235 | Reference | |
| 3.1–9.9 | 560 | 5,012 | 114 | 1.03 (0.82–1.30) | |
| ≥10 | 4,830 | 44,269 | 976 | 1.05 (0.91–1.21) | |
|
| |||||
| Dietary vitamin B12 intake | <10 | 990 | 9,411 | 148 | Reference |
| ≥10 | 2,419 | 22,355 | 490 | 1.20 (1.00–1.45) | |
| ≤3 | 703 | 6,804 | 93 | Reference | |
| 3.1–9.9 | 287 | 2,607 | 55 | 1.14 (0.82–1.60) | |
| ≥10 | 2,419 | 22,355 | 490 | 1.26 (1.01–1.58) | |
|
| |||||
| ≥median | <10 | 997 | 9,095 | 201 | Reference |
| ≥10 | 2,411 | 21,914 | 486 | 0.91 (0.77–1.08) | |
| ≤3 | 724 | 6,690 | 142 | Reference | |
| 3.1–9.9 | 273 | 2,405 | 59 | 0.98 (0.72–1.34) | |
| ≥10 | 2,411 | 21,914 | 486 | 0.91 (0.75–1.10) | |
|
| |||||
| Dietary folate intake | <10 | 1,025 | 9,701 | 175 | Reference |
| ≥10 | 2,383 | 21,949 | 478 | 1.07 (0.90–1.28) | |
| ≤3 | 773 | 7,418 | 118 | Reference | |
| 3.1–9.9 | 252 | 2,283 | 57 | 1.30 (0.94–1.79) | |
| ≥10 | 2,383 | 21,949 | 478 | 1.16 (0.94–1.42) | |
|
| |||||
| ≥median | <10 | 962 | 8,805 | 174 | Reference |
| ≥10 | 2,447 | 22,320 | 498 | 1.01 (0.85–1.20) | |
| ≤3 | 654 | 6,076 | 117 | Reference | |
| 3.1–9.9 | 308 | 2,729 | 57 | 0.86 (0.62–1.18) | |
| ≥10 | 2,447 | 22,320 | 498 | 0.95 (0.78–1.17) | |
|
|
|
|
|
|
|
| All participants | Negative | 3,882 | 36,446 | 684 | Reference |
| Mild to moderate | 2,139 | 19,833 | 412 | 1.07 (0.95–1.21) | |
| Severe | 796 | 6,496 | 229 | 1.09 (0.94–1.27) | |
|
| |||||
| Dietary vitamin B12 intake | Negative | 1,985 | 18,857 | 325 | Reference |
| Mild to moderate | 1,064 | 9,964 | 202 | 1.13 (0.94–1.35) | |
| Severe | 360 | 2,946 | 111 | 1.34 (1.06–1.68) | |
|
| |||||
| ≥median | Negative | 1,897 | 17,590 | 359 | Reference |
| Mild to moderate | 1,075 | 9,869 | 210 | 1.03 (0.86–1.22) | |
| Severe | 436 | 3,550 | 118 | 0.91 (0.73–1.13) | |
|
| |||||
| Dietary folate intake | Negative | 2,020 | 19,138 | 349 | Reference |
| Mild to moderate | 501 | 4,802 | 204 | 1.11 (0.93–1.33) | |
| Severe | 887 | 7,710 | 100 | 1.04 (0.83–1.31) | |
|
| |||||
| ≥median | Negative | 1,862 | 17,309 | 335 | Reference |
| Mild to moderate | 1,092 | 10,104 | 208 | 1.05 (0.88–1.25) | |
| Severe | 455 | 3,712 | 129 | 1.18 (0.95–1.46) | |
|
|
|
|
|
|
|
| All participants | Anti- | 1,829 | 17,187 | 310 | Reference |
| Anti- | 2,053 | 19,260 | 374 | 1.01 (0.87–1.17) | |
| Anti- | 158 | 1,319 | 39 | 1.13 (0.81–1.58) | |
| Anti- | 2,777 | 25,009 | 602 | 1.08 (0.94–1.24) | |
|
| |||||
| Dietary vitamin B12 intake | Anti- | 910 | 8,740 | 128 | Reference |
| Anti- | 1,075 | 10,116 | 197 | 1.15 (0.92–1.44) | |
| Anti- | 80 | 671 | 20 | 1.26 (0.78–2.03) | |
| Anti- | 1,344 | 12,239 | 293 | 1.30 (1.05–1.61) | |
|
| |||||
| ≥median | Anti- | 919 | 8,446 | 182 | Reference |
| Anti- | 978 | 9,144 | 177 | 0.90 (0.73–1.12) | |
| Anti- | 78 | 648 | 19 | 1.04 (0.64–1.69) | |
| Anti- | 1,433 | 12,770 | 309 | 0.93 (0.77–1.12) | |
|
| |||||
| Dietary folate intake | Anti- | 955 | 9,125 | 156 | Reference |
| Anti- | 1,065 | 10,013 | 193 | 1.07 (0.86–1.32) | |
| Anti- | 70 | 576 | 19 | 1.29 (0.79–2.08) | |
| Anti- | 1,318 | 11,936 | 285 | 1.12 (0.92–1.37) | |
|
| |||||
| ≥median | Anti- | 874 | 8,062 | 154 | Reference |
| Anti- | 988 | 9,247 | 181 | 0.95 (0.76–1.18) | |
| Anti- | 88 | 743 | 20 | 1.07 (0.67–1.72) | |
| Anti- | 1,459 | 13,073 | 317 | 1.06 (0.87–1.29) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Gastrointestinal motility and disorders · Whipple's Disease and Interleukins
1. Introduction
The prevalence of dementia is increasing with worldwide population aging and growth. The estimated number of people with dementia was 57.4 million cases globally in 2019 and is expected to reach 152.8 million cases in 2050 [1]. Dementia can cause severe cognitive, behavioral, and physical symptoms [2] and impose a profound psychological and economic burden not only on patients but also on people around them and society [3]. Effective measures to prevent dementia are urgently needed.
Among potentially modifiable factors, infectious diseases have recently received wide attention [4–6], partly due to the neuroinflammation they cause as an underlying mechanism [7]. Among these infectious diseases, Helicobacter pylori (H. pylori) is considered to affect not only the upper digestive tract but other organs also, including the brain [8]. Indeed, a meta-analysis of five cohort and five cross-sectional studies reported a positive association between H. pylori and all-cause dementia [9]. If this association is causal, the prevention and treatment of H. pylori infection will likely have considerable potential for reducing the number of people affected by dementia.
Nevertheless, some aspects of the association between H. pylori infection and dementia incidence remain unclear. For example, of the six cohort [10–15] and one case-control studies [16] of the association between H. pylori infection and dementia reported to date, only one was conducted in an Asian population [11]. Given that the prevalence of H. pylori infection and lifestyle vary by population [17], the previous studies’ findings may not be applicable to Asian populations. Secondary, the association between H. pylori infection and dementia incidence may vary with participants’ characteristics. As a biological mechanism potentially underlying the association, atrophic gastritis (AG) caused by H. pylori infection may impair the absorption of vitamin B12 and folate by reducing intrinsic factor secretion and increasing intragastric pH. Deficiencies in these vitamins impair the remethylation of homocysteine to methionine, resulting in elevated homocysteine levels. High homocysteine concentrations can lead to neuronal damage through direct toxicity to neurons and endothelial cells and impaired vasodilation [9, 18–20]. Lower dietary intakes of vitamin B12 and folate may accordingly strengthen the positive association between H. pylori infection and dementia, but to our knowledge no previous study has examined this interaction.
Against this background, we aimed to clarify the associations of H. pylori infection, AG and their combination with disabling dementia incidence using Japanese population-based cohort data, including stratified analyses by dietary intake of vitamin B12 and folate.
2. Methods
2.1. Study design and participants
The Japan Public Health Center-based Prospective (JPHC) Study Cohort II is a population-based cohort study established in 1993 with subjects aged 40–69 years residing in six public health center areas. Details of the study design have been reported previously [21]. Participants reported their lifestyle and disease history and provided blood samples at the baseline survey.
Data on the incidence of disabling dementia were obtained through national long-term care insurance (LTCI) certification records. Among the six study areas, these certification records were available in two districts (Ibaraki and Kochi areas), leaving 30,094 individuals as potential participants. The identification of disabling dementia cases started on January 1, 2006. Among the 30,094 potential participants, 5,208 became ineligible up to the start of follow-up for disabling dementia and were excluded (ineligible at baseline [N = 60], death [N = 3,042], moved out [N = 2,045], or lost to follow-up [N = 61]), leaving 24,886 individuals as eligible for follow-up for disabling dementia. For the present study, we further excluded 17,877 individuals without anti-Helicobacter pylori immunoglobulin (H. pylori IgG) titer or plasma levels of pepsinogen [PG] I and II due to their dissent against providing blood samples and 192 who did not answer the baseline survey questionnaire, leaving 6,817 individuals as eligible for the present analysis (Fig. 1).
Flowchart showing the selection of eligible participants.Legend: JPHC, Japan Public Health Center-based Prospective (JPHC) Study; IgG, immunoglobulin G.
2.2. Exposure
Plasma levels of H. pylori IgG were measured by enzyme immunoassay (E plate “Eiken” H. pylori Antibody II; Eiken Kagaku) and grouped into two (anti-H. pylori IgG titer of <10 [H. pylori-seronegative] and ≥10 U/mL [H. pylori-seropositive]) and three categories (≤3, 3.1–9.9, and ≥10 U/mL) [22, 23]. A cross-sectional study in Japan compared the diagnostic performance of the above binary categorization against endoscopic diagnosis as gold standard and reported a sensitivity of 74.8%, specificity of 99.4%, and accuracy of 96.3% [24]. Additionally, as a marker of AG, plasma levels of PG I and II were measured by latex agglutination (LZ test “Eiken” Pepsinogen I, II; Eiken Kagaku) and defined as “negative” (PG I >70 ng/mL or a ratio of PG I by PG II [PG I/II] >3.0) or “positive” (PG I ≤70 ng/mL and PG I/II ≤3.0) [22] and further as “negative” (PG I >70 ng/mL or PG I/II >3.0), “mild to moderate” (PG I ≤70 ng/mL and PG I/II ≤3.0 excluding severe cases), or “severe” (PG I ≤30 ng/mL and PG I/II ≤2.0) [25]. A meta-analysis evaluated the diagnostic performance of the above binary AG criteria against gastric endoscopic examination as gold standard and reported a sensitivity of 77%, specificity of 73%, positive predictive value of 0.77–1.25%, and negative predictive value of 99.08–99.90% [26]. To investigate a possible synergistic effect of H. pylori infection and AG, we also categorized participants into the following four groups: H. pylori-seronegative and AG-negative (H. pylori−/AG−); H. pylori-seropositive and AG-negative (H. pylori+/AG−); H. pylori-seronegative and AG-positive (H. pylori−/AG+); and H. pylori-seropositive and AG-positive (H. pylori+/AG+) [22].
2.3. Covariates
The present study considered the following factors as covariates: age (continuous), sex, area, smoking status, alcohol consumption, body mass index (BMI), frequency of leisure-time physical activity, living alone (as an index of social isolation), and history of diseases (cardiovascular disease [myocardial infarction and stroke], diabetes, and hypertension). These variables are considered dementia risk factors [27]. Covariates other than age, sex, and area were created based on self-reported information from the baseline questionnaire. Table 1 shows the cut-off values of categorical variables. Additionally, the present study considered dietary intakes of vitamin B12 and folate as potential factors that interact with H. pylori infection. These were calculated based on self-reported information from a food frequency questionnaire of the baseline survey. The validity of vitamin B12 and folate intake was assessed among subsamples (268 males and 283 females) using 28-day dietary records. The respective energy-adjusted Spearman correlation coefficients (in males and females) between intakes estimated from the questionnaire and dietary records were vitamin B12, 0.37 and 0.34; and folate, 0.39 and 0.47 (unpublished data). We categorized participants into two groups based on the medians of our sample (vitamin B12: 5.1 µg/day; folate: 271.0 µg/day). These cut-off values were generally consistent with the Dietary Reference Intakes for Japanese 2025 (vitamin B12: 4.0 µg/day; folate: 240 µg/day) [28] and the medians reported by the National Health and Nutrition Survey in Japan 2023 (vitamin B12: 4.2 µg/day; folate: 281 µg/day) [29].
2.4. Follow-up and case identification
Disabling dementia, our primary outcome, was defined according to the Japanese long-term care insurance (LTCI) certification. In the Japanese LTCI system, residents need to apply for assessment by their municipality to be eligible for LTCI benefits. This assessment requires two documents: 1) a comprehensive assessment of mental and physical conditions and 2) an opinion by a primary care physician, including a dementia rating scale. Based on these two documents, the committee of long-term care requirement certification, composed of experts in medical, health, and welfare areas, determines the care level for the applicant [30].
The dementia rating scale consists of 0, I, IIa, IIb, IIIa, IIIb, IV, and M, and are defined as follows: 0, no dementia symptoms; I, having some dementia-related symptoms but almost fully independent in daily living; IIa, sometimes having difficulty in daily living or communication outside the home but be independent in daily living life under someone’s attention; IIb, sometimes having difficulty in daily living or communication even at home but independent in daily living life under someone’s attention; IIIa, having difficulty in daily living or communication mainly during day time and requiring care; IIIb, having difficulty in daily living or communication mainly during the night and requiring care; IV, frequently having difficulties in daily living due to symptoms, behaviors, and communication problems and always requiring care; and M, having severe physical, mental, or behavioral symptoms and requiring specialized treatment [31].
The present study defined disabling dementia as a ‘certification for the level of requiring care in daily living’ and ‘dementia rating scale of IIa or above’. This definition was proved to have adequate sensitivity (73%) and specificity (96%) compared with neuropsychiatrists’ diagnoses as gold standard [32]. Participants were followed from January 1, 2006 until December 31, 2016, and the initial certification date was defined as the incidence date of the above disabling dementia.
2.5. Statistical analysis
The association of H. pylori IgG titer, AG and their combination with disabling dementia was examined with a multivariable-adjusted Cox proportional hazard model, and hazard ratios (HRs) were estimated with their 95% confidence intervals (CIs). We built one multivariable model, which incorporated covariates categorized as shown in Table 1. These models treated migration from a study area, death, loss to follow-up, and the end of follow-up (December 31, 2016) as censored events. We also conducted stratified analyses by dietary intakes of vitamin B12 and folate to examine potential interaction by these factors. These analyses stratified participants using median values of vitamin B12 and folate intakes. We also calculated P values for the interaction term between H. pylori infection (H. pylori− vs. H. pylori+) and AG (AG− vs. AG+) within each category of vitamin B12 and folate intake, followed by a likelihood ratio test. Finally, we conducted additional stratified analyses by the following factors to ascertain interactions by demographic and lifestyle variables on the association between H. pylori infection and dementia: sex, age, smoking status, alcohol consumption, BMI, and frequency of leisure-time physical activity. In all models, for covariates with missing values, a “missing” category was created and included as a dummy variable in the regression models along with the other categories. All statistical tests were two-sided and a P value <0.05 were considered to indicate statistical significance. All statistical analyses were conducted using SAS software version 9.4 (SAS Institute, Cary, NC).
3. Results
Among the 6,817 participants, 4,830 individuals (70.9%) had an anti-H. pylori IgG titer of ≥10 U/mL. Of these, 2,935 (43.1%) had AG. Table 1 shows participant characteristics by anti-H. pylori IgG titer. Individuals with a higher anti-H. pylori IgG titer tended to be male, live in the Ibaraki area, be past or current smokers, and have a history of hypertension.
During a median follow-up of 11.0 years, 1,325 participants (19.4%) had disabling dementia. Table 2 shows the association between anti-H. pylori IgG titer and disabling dementia. A higher anti-H. pylori IgG titer was not associated with the risk of disabling dementia among all participants, but was associated with increased risk among individuals consuming less vitamin B12 than the median value, with fully adjusted HRs of 1.14 (95% CI: 0.82–1.60) and 1.26 (95% CI: 1.01–1.58) for anti-H. pylori IgG levels of 3.1–9.9 and ≥10 U/mL, respectively, compared with ≤3 U/mL. On the other hand, anti-H. pylori IgG was not associated with disabling dementia regardless of folate intake.
Table 3 shows the association between AG status and disabling dementia. Whereas having AG was not associated with the risk of disabling dementia among all participants, and regardless of folate intake, having severe AG was associated with risk among individuals consuming less vitamin B12 than the median value (HR 1.34, 95% CI: 1.06–1.68).
Table 4 presents the association between the combination of H. pylori infection and AG with disabling dementia. In this analysis, having both H. pylori infection and AG among individuals consuming less vitamin B12 than the median was associated with an increased risk of dementia (HR 1.30, 95% CI: 1.05–1.61) compared with those who were H. pylori-seronegative and AG-negative, but the hazard ratio of having only H. pylori or AG was also higher than unity (HR 1.15, 95% CI: 0.92–1.44 for H. pylori-positive only; HR 1.26, 95% CI: 0.78–2.03 for AG-positive only). On the other hand, the stratified analysis by folate intake found no associations.
Finally, eTable 1 shows that there were no associations between H. pylori infection and disabling dementia in any subgroup stratified by demographic and lifestyle variables.
4. Discussion
In this study of the associations of H. pylori infection, AG, and their combination with disabling dementia using Japanese population-based cohort data, we found that H. pylori infection showed no overall association with disabling dementia. However, H. pylori infection, AG, and their combination were associated with increased risks of disabling dementia among individuals with low dietary vitamin B12 intake. This may corroborate the biological hypothesis which implicates both AG and concurrent impaired absorption of vitamin B12 as underlying factors [9]. Based on our results, dementia incidence may be associated with not only H. pylori infection but also subsequent AG and low dietary vitamin B12 intake.
Among six cohort studies [10–15] and one case-control study [16] that investigated the association between H. pylori infection and dementia, five studies found a positive association [10, 11, 13, 15, 16]. These findings are inconsistent with our lack of association among all participants. Some factors may explain this inconsistency. First, body fatness in midlife can trigger chronic inflammation, metabolic diseases (e.g., hypertension, diabetes), and cardiovascular disease, leading to an increased risk of dementia [33]. The proportion of individuals with overweight or obesity (BMI ≥25.0 kg/m^2^) was higher in these previous studies (e.g., 40–60% [13, 16]) than in our present study (25.5%), which might account for the lack of association in the present study. Indeed, in our present stratified analyses, while H. pylori infection was associated with a statistically non-significant increased risk of dementia among individuals with BMI ≥25.0 kg/m^2^ (anti-H. pylori IgG titer ≥10 U/mL: HR 1.24 [95% CI: 0.92–1.67]), no association was seen among individuals with BMI <25.0 kg/m^2^ (HR 0.97 [95% CI: 0.82–1.14]; eTable 1). Second, differences in the number of gastric cancer deaths might account for the inconsistent findings between these previous and our present study - namely, H. pylori infection might lead to premature death from gastric cancer before onset of dementia. However, an additional analysis that considered gastric cancer deaths as competing events showed no material change in the subdistribution hazard ratio among all participants from the hazard ratios of the main analysis (anti-H. pylori IgG of 3.1–9.9 U/mL: subdistribution HR 1.02 [95% CI: 0.81–1.29]; ≥10 U/mL: subdistribution HR 1.04 [95% CI: 0.90–1.20]).
In the present study, H. pylori infection, AG and their combination were associated with disabling dementia only among individuals with low dietary vitamin B12 intake. Although previous studies did not examine the influence of dietary intake of vitamin B12 and folate, our results are partially consistent with the biological hypothesis that H. pylori infection is associated with dementia incidence [9]. According to this hypothesis, AG caused by H. pylori infection can hinder the absorption of vitamin B12 and folate, thereby leading to higher homocysteine concentration [9, 18]. High concentrations of homocysteine damage vascular endothelial and neuronal cells and thereby lead to brain atrophy and degeneration [34]. A meta-analysis of 10 prospective cohort studies demonstrated a positive linear dose-response relationship between homocysteine level and risk of stroke [35]. Additionally, another meta-analysis of 13 prospective cohort studies reported positive associations between homocysteine concentration and risk of all-cause dementia, Alzheimer’s disease, and vascular dementia [36]. On this basis, low dietary intakes of vitamin B12 combined with AG may exacerbate vitamin B12 deficiency developed from AG, thereby increasing the risk of dementia. Importantly, the interaction term between H. pylori infection and AG was non-significant in participants with low vitamin B12 intake (P for interaction = 0.659, data not shown in Table 4), and having AG without H. pylori infection showed a non-significant but positive association with dementia (Table 4). Considering these points, dementia incidence might not necessarily depend on H. pylori infection but rather on AG among participants with lower vitamin B12 intakes. Interrelationships of H. pylori infection, AG and vitamin B12 intake in developing dementia warrant further investigations. Regarding the lack of synergistic effects of H. pylori infection, AG and folate, a meta-analysis of 32 clinical studies of H. pylori infection and blood or urinary micronutrient levels has provided some insights, including that H. pylori infection and eradication influence vitamin B12 level but not folate level [37]. Accordingly, dietary folate intakes could not have interacted with H. pylori infection and AG on the risk of dementia in the present study.
H. pylori infection is thought to negatively affect cognitive function through other biological mechanisms, as well as through the impaired absorption of vitamin B12 by AG [9, 16]. We speculate about two possibilities. First, H. pylori can be conveyed to the brain via the oral-nasal-olfactory pathway or by circulating monocytes, possibly causing neurodegeneration [38]. Second, gut microbiota altered by H. pylori infection could produce amyloids and lipopolysaccharides, which may modulate signaling pathways and elevate proinflammatory cytokine levels [38].
The strengths of the present study include its prospective follow-up of disabling dementia among Japanese community-dwelling adults, identification of dementia cases through standardized methods, examination on interaction among H. pylori infection, AG, and dietary intakes of vitamin B12 and folate, and extensive adjustment of covariates. The following limitations should also be mentioned. First, anti-H. pylori IgG titer was unmeasured in a large proportion of potential participants (71.8% of potential participants residing in areas where H. pylori IgG measurement was conducted), which may have limited the generalizability of the findings. Second, although we used validated criteria for AG, endoscopic results were not available, which may have led to the misclassification of AG. Third, some participants may have been affected by H. pylori between the baseline survey and the end of follow-up, which may have brought about exposure misclassification. Against this, H. pylori infection is mainly acquired in childhood, and acquisition during adulthood is rare [39]. Fourth, AG acquired after the baseline survey may also have led to exposure misclassification. To our knowledge, the typical age of AG acquisition is rarely studied. Fifth, the present study could not differentiate dementia subtypes (e.g., Alzheimer’s or vascular dementia) because the present study does not collect this information. A previous analysis that used data of the JPHC Study showed no association between H. pylori infection and stroke [40], and thus dementia caused by the infection seemed to be mainly of the Alzheimer type. However, our relatively small number of subjects prevented an additional stratified analysis by stroke concurrent with dementia. Sixth, we did not measure the blood concentrations of vitamin B12 and folate, which forced us to rely on their dietary intakes and may have led to the misclassification of concentrations. Seventh, information on the use of vitamin B12 and folate supplements or medications was not available in our study, which may have affected the results of analyses involving these vitamins. Eighth, the present study addressed missing data by creating “missing” categories, but this may have led to the misclassification of covariates.
In conclusion, H. pylori infection generally was not associated with increased risk of disabling dementia among the Japanese population. Nevertheless, the combination of H. pylori infection, subsequent AG, and low vitamin B12 intake may be related to an increased risk of dementia. Although causality cannot be inferred from our observational data, if such a synergistic relationship is confirmed, monitoring AG and vitamin B12 status, as well as promoting adequate vitamin B12 intake, could represent promising public health strategies for dementia prevention among individuals affected by H. pylori infection or AG.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7(2):e 105–25. doi: 10.1016/S 2468-2667(21)00249-8.34998485 PMC 8810394 · doi ↗ · pubmed ↗
- 2Japanese Society of Neurology. Clinical Practice Guideline for Dementia 2017. https://neurology-jp.org/guidelinem/dementia/index.html. Published 2017. Accessed March 14, 2024.
- 3Bruck CC, Wolters FJ, Ikram MA, de Kok I. Projections of costs and quality adjusted life years lost due to dementia from 2020 to 2050: A population-based microsimulation study. Alzheimers Dement. 2023;19(10):4532–41. doi: 10.1002/alz.13019.36916447 · doi ↗ · pubmed ↗
- 4Beydoun HA, Beydoun MA, Meirelles O, Erickson LD, Gamaldo AA, Weiss J, . Cardiovascular health, infection burden, and incident dementia in the UK Biobank. Alzheimers Dement. 2023;19(10):4475–87. doi: 10.1002/alz.13405.37547953 PMC 10592296 · doi ↗ · pubmed ↗
- 5Bohn B, Lutsey PL, Misialek JR, Walker KA, Brown CH, Hughes TM, . Incidence of Dementia Following Hospitalization With Infection Among Adults in the Atherosclerosis Risk in Communities (ARIC) Study Cohort. JAMA Netw Open. 2023;6(1):e 2250126. doi: 10.1001/jamanetworkopen.2022.50126.36622673 PMC 9857407 · doi ↗ · pubmed ↗
- 6Muzambi R, Bhaskaran K, Brayne C, Davidson JA, Smeeth L, Warren-Gash C. Common Bacterial Infections and Risk of Dementia or Cognitive Decline: A Systematic Review. J Alzheimers Dis. 2020;76(4):1609–26. doi: 10.3233/JAD-200303.32651320 PMC 7504996 · doi ↗ · pubmed ↗
- 7Lim SL, Rodriguez-Ortiz CJ, Kitazawa M. Infection, systemic inflammation, and Alzheimer’s disease. Microbes Infect. 2015;17(8):549–56. doi: 10.1016/j.micinf.2015.04.004.25912134 · doi ↗ · pubmed ↗
- 8Zendehdel A, Roham M. Role of Helicobacter pylori infection in the manifestation of old age-related diseases. Mol Genet Genomic Med. 2020;8(4):e 1157. doi: 10.1002/mgg 3.1157.32067423 PMC 7196471 · doi ↗ · pubmed ↗