Adrenal Metastasis of Hepatocellular Carcinoma With Unknown Primary: A Case Report
Colleen Conger, John Yassa, Mohit Agarwal, Sukeshi Arora, Neil Newman

TL;DR
A rare case of adrenal metastasis from hepatocellular carcinoma with an unknown primary was successfully treated with high-dose radiation, showing good long-term outcomes.
Contribution
This case report presents a rare clinical scenario and demonstrates the effectiveness of SBRT for treating HCC with an unknown primary.
Findings
The patient showed marked tumor shrinkage and biochemical response after SBRT treatment.
27 months post-treatment, the patient remains disease-free with normal AFP levels.
SBRT can provide excellent local and biochemical control for oligometastatic HCC with an unknown primary.
Abstract
Solitary extrahepatic hepatocellular carcinoma (HCC) with an unknown primary has been rarely reported in the literature. We report a case of a 69-year-old Hispanic male with no history of malignancy presenting with a solitary 5cm adrenal mass found incidentally on CT surveillance for high-risk liver disease secondary to chronic hepatitis C (HCV). Biopsy returned as metastatic poorly differentiated hepatocellular carcinoma. A dedicated liver MRI was performed to evaluate for a primary site, but no dominant lesion was noted. Follow-up abdominal CT two months later revealed interval enlargement of the mass to 6.2cm with an alpha-fetoprotein (AFP) of 169 ng/ml. After a multidisciplinary discussion, this was deemed a tumor of unknown primary. The patient was offered definitive treatment with stereotactic body radiotherapy (SBRT) 60 Gy in 8 fractions, with careful attention paid to the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
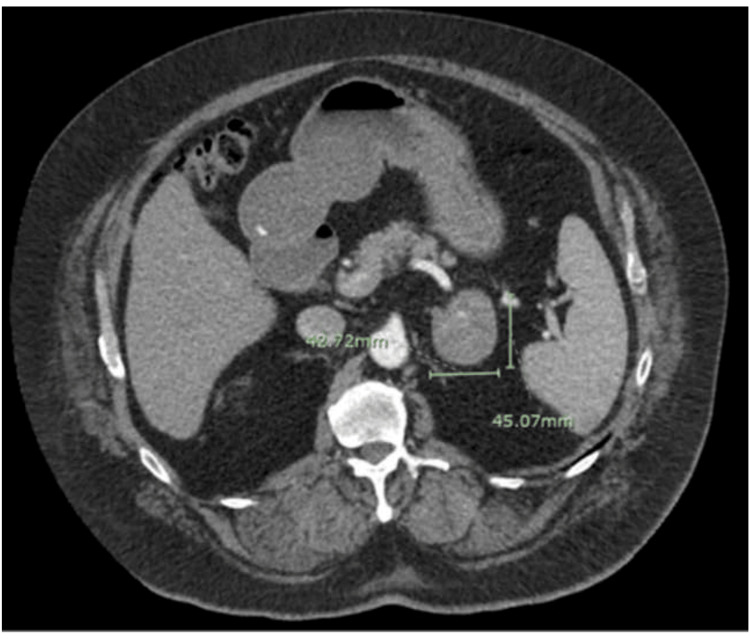 Figure 1
Figure 1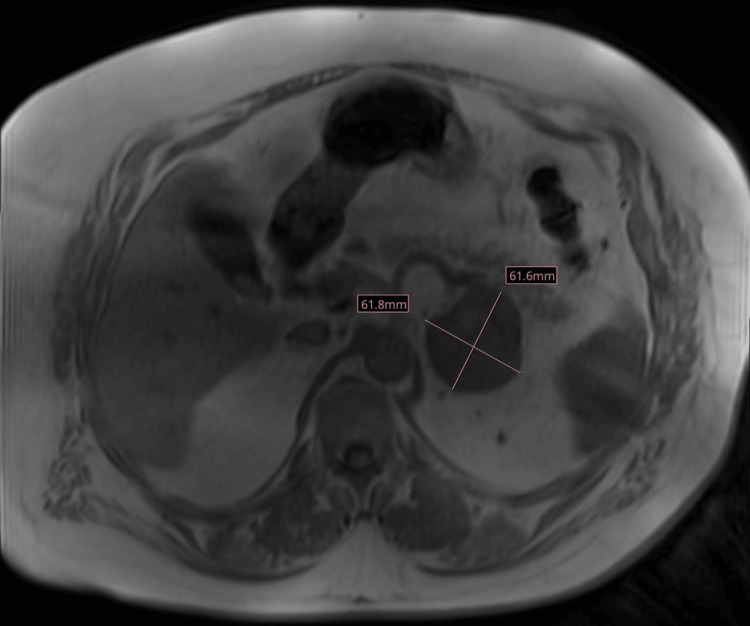 Figure 2
Figure 2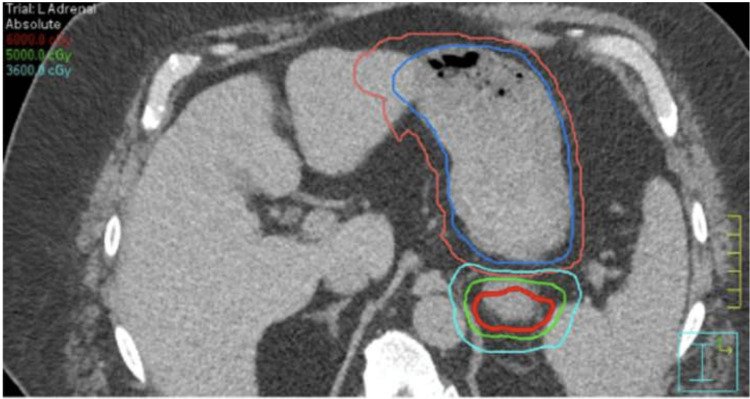 Figure 3
Figure 3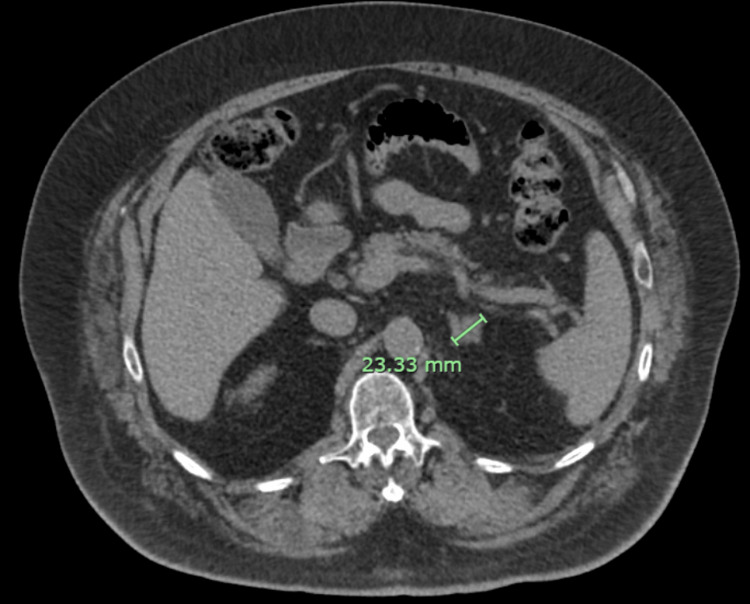 Figure 4
Figure 4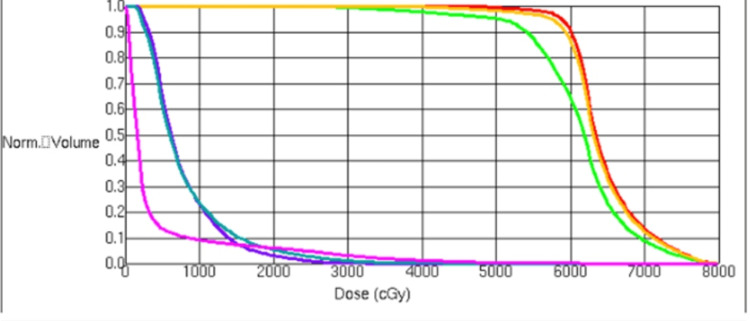 Figure 5
Figure 5| AFP Reference range | Pre-treatment AFP | Immediate post-treatment AFP | 3 months post-treatment AFP | 45 months post-treatment AFP |
| <20.0 ng/mL | 27.6 | 169 | 20 | 8.16 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Hepatocellular Carcinoma Treatment and Prognosis · Testicular diseases and treatments
Introduction
As of 2018, primary liver cancer is the seventh most common cancer worldwide, with 75% of new cases being hepatocellular carcinoma (HCC) [1]. In 2019, 35,563 new cases of liver cancer and 27,958 deaths due to liver cancer were reported in the United States alone [2], with an estimated 80% of these being HCC [3]. Risk factors for HCC include American Indian/ Alaska native race [4], HBV and HCV infection [5], excessive alcohol consumption [6], metabolic syndrome, including diabetes and obesity [7], and NAFLD.
Extrahepatic metastases of HCC are most common in the lungs, abdominal lymph nodes, and bones [8]. Metastases to the adrenal glands occur in about 10% of cases [9]. Metastasis almost exclusively occurs when the primary tumor is stage III or IVA [9]. Despite the frequency of HCC metastasis, HCC rarely presents as a metastatic tumor of unknown primary. Only isolated cases have been reported, with the prevalence of HCC of unknown primary remaining unknown [10-15].
The currently agreed-upon first-line therapy for advanced unresectable or metastatic HCC is immunotherapy [16-17]. Stereotactic body radiotherapy (SBRT) has also previously demonstrated excellent local control of advanced primary liver disease (95% at 5 years [18], with an overall survival benefit in a phase 3 randomized trial showing no increased rates of grade 3 toxicity [19]. We present a case in which SBRT was used to treat HCC of unknown primary, with the only known site of disease in the adrenal glands.
Case presentation
A 69-year-old Hispanic male, with a history of decompensated liver disease secondary to hepatitis C (HCV) cirrhosis (Child-Pugh class A6) treated with Harvoni (ledipasvir/sofosbuvir) with sustained viral response, presented due to an oligometastatic adrenal mass of unknown origin. The solitary 4.2 x 4.5 cm indeterminate adrenal mass was found incidentally while he was receiving CT surveillance for his high-risk liver disease (Figure 1). The mass was concerning for malignancy, as comparison CT imaging from eight months prior did not reveal an adrenal mass. At the time of diagnosis, the liver was noteworthy for only mild nodular liver margins with a slightly enlarged caudate lobe, but no masses on CT. The patient’s alpha-fetoprotein (AFP) level at this time was elevated to 27.6 ng/ml (normal = <20). Biopsy of the mass returned as metastatic poorly differentiated HCC.
Abdominal CT 3-phase demonstrating a 4.2 x 4.5 cm adrenal mass.
A dedicated liver MRI was performed to evaluate for a possible HCC primary site, but no dominant lesion was noted. Follow-up abdominal MRI two months later revealed interval enlargement of the mass to 6.2 x 6.2 cm (Figure 2). It was noted to be heterogeneously enhancing and centrally necrotic, with a moderate thrombus in the left adrenal vein. Further lab workup at this time revealed an AFP of 118.6 ng/ml. After a multidisciplinary discussion, this was deemed a tumor of unknown primary.
Abdominal MRI showing interval enlargement of the mass to 6.2 x 6.2 cm.
The patient was offered definitive treatment with SBRT to 60 Gy in 8 fractions, with careful attention paid to the stomach, which bordered the superior 2 cm of the tumor. The patient was simulated supine, arms up, in a Vac-Lok bag, with IV contrast, after fasting for 6 hours prior to simulation. He had a 4-dimensional CT scan, with which the tumor motion was tracked in space throughout his entire respiratory cycle.
The gross tumor volume (GTV) was 128 cc, with a planned target volume (PTV) expansion to 195 cc (Figure 3). The stomach was constrained to a dose of 5 cc (D5cc) of less than 31 Gy and a D0.035cc of less than 40 Gy. A planning organ at risk volume (PRV) was created for the stomach and small intestines and kept to a 40 Gy maximum. These PRVs were comprised of the motion of these structures in the 4D CT with an additional 0.5cm margin. Daily imaging required cone beam CT scans, with isodose lines imported into the structures.
Isodose lines of the tumor and stomach. Note the proximity of the stomach to the superior 2 cm of the tumor.
AFP levels as well as serial imaging were used to track treatment efficacy and disease response (Table 1). Two weeks after completion of treatment, the patient’s AFP was elevated (an expected acute reaction) to 169 ng/ml. Retesting three months later, however, showed a reduced AFP of 20 ng/ml. CT imaging at the one-year follow-up was also consistent with a marked decrease in the size of the tumor from 6.2 cm to 2.3 cm (Figure 4). At 12-month follow-up, his tumor had shrunk to 2.1 cm in greatest dimension, and his AFP was 19 ng/ml. At the time of this case report, 45 months after treatment completion, the patient remains without signs of disease progression. His most recent AFP was 8.16 ng/ml, and the mass size on imaging was 1.5 cm. This patient has not received any systemic therapy.
One-year follow-up abdominal CT 3-Phase showing an interval decrease in tumor size to 2.3 cm
Discussion
HCC is the most common primary hepatic malignancy, particularly in patients with preexisting liver disease. The adrenal gland is the sixth most common site of metastasis after the lungs, peritoneum, bone, lymph nodes, and spleen [20]. This patient’s presentation of metastasis to the adrenal gland, with an unknown primary hepatic tumor, has not been previously reported. Previous literature on HCC metastases with unknown primary is currently limited to the cervical spine, pelvic bones, chest wall, skull, and sternum [10-15].
As of 2018, the current standard of treatment in the United States for HCC is systemic therapy utilizing immunotherapy with Atezolizumab and Bevacizumab or Durvalumab and Tremelimumab [17]. The use of radiotherapy in the treatment of HCC is currently only strongly recommended in the case of liver-confined multifocal or unresectable HCC [21]. Due to its rarity, there is no known literature on primary radiotherapy treatment alone of hepatocellular carcinoma metastases with an unknown primary tumor.
The current recommendation for treating liver-confined HCC with RT suggests a minimum BED10 of 6500 to 7900 cGy [22]. In series with large median tumor sizes, local control appears to be excellent with dose escalation18. However, despite this, HCC appears to be somewhat radiosensitive to high doses per fraction. Even doses as low as 30 Gy in 6 fractions (45 BED) or 35 Gy in 5 fractions [19] appear to have adequate local control [23]. This patient’s 6.2 x 6.2cm mass received a BED10 of 105 to the majority of the GTV. This was necessary to administer an adequate dose to the tumor, as the PTV could not include the whole tumor in areas that bordered the stomach. With this method, 95% of the GTV received a dose of 60 Gy, and 95% of the PTV received a dose of 50 Gy (Figure 2). The dose-volume histogram (DVH) demonstrates that the constraints met for this patient were within the recommended doses (Figure 5). It is imperative, as a principle with oligometastatic disease, to place more weight on the organ at risk over the tumor coverage, especially with a pathology that can be responsive to a lower total biological effective dose (BED).
Dose volume histogram of left adrenal gland treatment plan.Color glossary: Red- GTV; Orange- ITV; Green- PTV; Purple- stomach; Teal- Stomach PRV; Pink- kidneys.
This patient also never received any systemic therapy. While this is the standard of care for advanced/metastatic liver disease, a trial of total consolidation may be able to delay the time to systemic therapy. Systemic therapy has not only financial burdens to underserved patients, but also high rates of grade 3 toxicity.
Conclusions
HCC with solitary extrahepatic presentation is rare. Treatment with SBRT alone to an extrahepatic metastasis can yield excellent local and biochemical control, as expected based on the literature for primary SBRT to HCC lesions. This case underscores the importance of cautious attention to sparing of normal organs at risk, such as the stomach, since HCC tumors can respond to BED doses as low as 45 Gy. This contrasts with other tumors requiring considerably higher BED in the same region. High-dose SBRT has been used for this patient to definitively treat oligometastatic hepatocellular carcinoma with an unknown primary tumor, with a short-interval encouraging biochemical and radiological response. However, longer-term follow-up will be needed to assess local control, whether new metastases arise, and longer-term toxicity in this patient. Further study in a larger cohort of patients to investigate whether SBRT alone could be effectively used for local control and delays to initiating systemic therapy could prove beneficial.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hepatocellular carcinoma study 6 2025 2018 https://www.cancer.gov/ccg/research/genome-sequencing/tcga/studied-cancers/hepatocellular-carcinoma-study
- 2Epidemiology of hepatocellular carcinoma Hepatology Mc Glynn KA Petrick JL El-Serag HB 41373202110.1002/hep.31288 PMC 757794632319693 · doi ↗ · pubmed ↗
- 3United States cancer statistics: Data visualizations 6 2025 2023 https://gis.cdc.gov/Cancer/USCS/
- 4Surveillance, epidemiology, and end results program 6 2025 2018 https://seer.cancer.gov/
- 5Global epidemiology of hepatocellular carcinoma: An emphasis on demographic and regional variability Clin Liver Dis Mc Glynn KA Petrick JL London WT 2232381920152592166010.1016/j.cld.2015.01.001PMC 4712629 · doi ↗ · pubmed ↗
- 6Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis Br J Cancer Bagnardi V Rota M Botteri E 5805931122014 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 4453639/2542290910.1038/bjc.2014.579PMC 4453639 · doi ↗ · pubmed ↗
- 7The association between metabolic syndrome and hepatocellular carcinoma: Systemic review and meta-analysis J Clin Gastroenterol Jinjuvadia R Patel S Liangpunsakul S 1721774820142440212010.1097/MCG.0b 013e 3182 a 030c 4PMC 3887366 · doi ↗ · pubmed ↗
- 8Extrahepatic metastases of hepatocellular carcinoma Radiology Katyal S Oliver JH 3rd Peterson MS Ferris JV Carr BS Baron RL 6987032162000 https://pubs.rsna.org/doi/abs/10.1148/radiology.216.3.r 00se 246981096669710.1148/radiology.216.3.r 00se 24698 · doi ↗ · pubmed ↗