Association of severe stress with the onset of chronic kidney disease after the Great East Japan Earthquake: the Fukushima Health Management Survey
Sakumi Kazama, Fumikazu Hayashi, Kenichi Tanaka, Shiho Sato, Yuka Ueda, Kanako Okazaki, Tetsuya Ohira, Akira Sakai, Masaharu Maeda, Hirooki Yabe, Mitsuaki Hosoya, Atsushi Takahashi, Hironori Nakano, Masanori Nagao, Michio Shimabukuro, Hitoshi Ohto, Seiji Yasumura

TL;DR
This study found that severe stress after a natural disaster was linked to the development of chronic kidney disease in residents of the Fukushima area.
Contribution
The study identifies severe psychological stress as a novel risk factor for CKD onset following a major disaster.
Findings
Severe stress, measured by K6 score, was significantly associated with CKD onset.
Common risk factors like age, BMI, and hypertension also contributed to CKD development.
Stress management could be a new strategy for CKD prevention and treatment.
Abstract
In 2011, the Great East Japan Earthquake hit the Futaba District on the northeast coast of Japan, followed by a tsunami and a nuclear power plant accident. In this study, we investigated the impact of post‐earthquake life on the onset of chronic kidney disease (CKD) among the residents of the Futaba District. Data on 17,859 residents of the Futaba District (7333 men, 10,526 women; mean age: 61.0 ± 10.2 years; mean follow-up period: 3.42 ± 1.51 years) who underwent health checkups and completed self-administered questionnaires in the Fukushima Mental Health and Lifestyle Survey were analyzed. These residents were confirmed to be CKD-free in 2012. Hence, they were assessed for the onset of CKD from 2013 to 2017. Univariate analysis results showed significant differences between residents with and without CKD. Differences in age, diabetes mellitus, body mass index (BMI), dyslipidemia,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
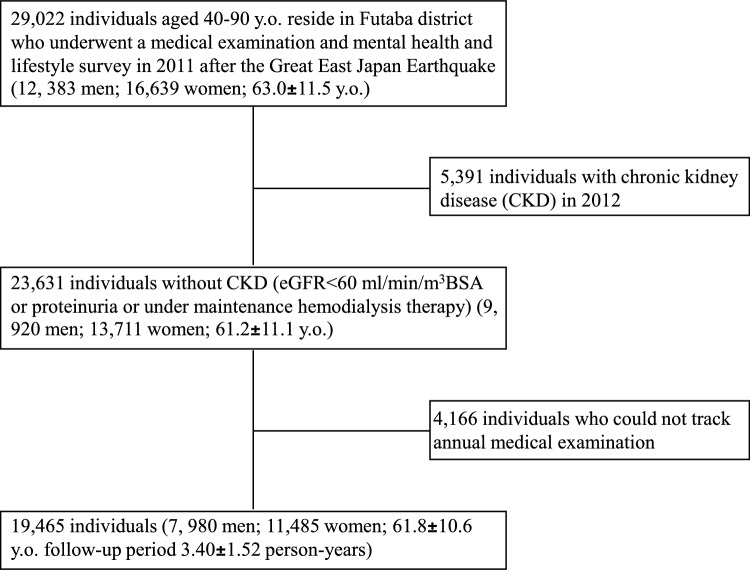 Figure 1
Figure 1- —The National Health Fund for Children and Adults Affected by the Nuclear Incident
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMuscle and Compartmental Disorders · Effects of Radiation Exposure · Disaster Response and Management
Introduction
On March 11, 2011, the eastern region of Japan was hit by a massive earthquake of magnitude 9.1, later designated the Great East Japan Earthquake. This earthquake triggered a tsunami immediately after, causing a level-7 major accident at the Fukushima Daiichi Nuclear Power Plant, which forced the evacuation of many of the residents around the plant [1, 2]. Disasters and the corresponding evacuation processes impose not only a direct physical impact but also a significant psychological burden.
Chronic kidney disease (CKD) is a clinical concept characterized by persistent reduction in glomerular filtration rate and/or sustained proteinuria, irrespective of the underlying etiology. In Japan, it has been estimated that approximately one in eight adults has CKD (3); however, more recent expert opinion suggests that the prevalence may have increased to as high as one in five. Although various factors are involved in CKD progression, no cohorts for clinical studies on the effects of psychological factors have been studied.
We conducted longitudinal analyses of data from the health checkups of the residents of the Futaba District [3]. This study comprised a cohort of individuals who share an experience with considerable psychological and social impacts. This study aimed to elucidate the impact of post-earthquake life on the onset of CKD, with a focus on the psychological impacts of the earthquake.
Materials and methods
Participants
Among the residents of the 13 municipalities who were evacuated during the disaster, 26,619 residents aged 40–90 years participated in the study. These individuals had undergone the Comprehensive Health Check [4] included in the scope of the Fukushima Health Management Survey [5] and completed the self-administered questionnaires in the Mental Health and Lifestyle Survey [6] (valid response count: 73,569 residents; response rate: 40.7%) in 2012. Among them, 17,898 residents who were confirmed to have no CKD in 2012 were assessed for CKD onset from 2013 to 2017. The questionnaires were distributed each February; therefore, the baseline data were obtained from the first survey conducted in February 2012, approximately 11 months after the disaster. We excluded 39 residents lost to follow-up before 2017. Thus, the present study included 17,859 residents in the analysis of the risk factors associated with the onset of CKD (Fig. 1).Fig. 1. Flowchart of participant inclusion in the analysis
Definition of CKD
eGFR was calculated for each sex based on serum creatinine levels and age using the following formulas recommended by the Japanese Society of Nephrology [7]. In this study, individuals were defined as having CKD if they met any of the following criteria: an eGFR < 60 mL/min/1.73 m^2^; a proteinuria level of ≥ 1 +; or a self-reported history of receiving treatment for chronic renal failure (including maintenance hemodialysis) on the questionnaire.
Definition of lifestyle diseases
Obesity: body mass index (BMI) ≥ 25 kg/m^2^; hypertension: systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, or individuals taking antihypertensives; diabetes mellitus: fasting blood glucose level ≥ 126 mg/dL, hemoglobin A1c (HbA1c) level ≥ 6.5%, or individuals taking hypoglycemics; dyslipidemia: high-density lipoprotein cholesterol level < 40 mg/dL, low-density lipoprotein cholesterol level ≥ 140 mg/dL, fasting triglyceride level ≥ 150 mg/dL, or individuals taking antihyperlipidemic; abnormal hepatic function: aspartate aminotransferase level ≥ 31 U/L, alanine aminotransferase level ≥ 31 U/L, or gamma-glutamyl transferase level ≥ 51 U/L; and hyperuricemia: uric acid level ≥ 7.9 mg/dL and ≥ 5.6 mg/dL for men and women, respectively.
Definition of psychological distress
The Kessler 6 Psychological Distress Scale (K6) score [8] was adopted to assess psychological distress. The reliability of the Japanese version of the K6 score has been verified [9]. Based on previous studies [10], a K6 score of ≥ 13 was determined to indicate psychological distress.
Definition of lifestyle
Smoking habit was defined as follows: never smoked, former smoker, or current smoker. Alcohol drinking habits were defined as never drank, former drinker, or current drinker. Sleep satisfaction was classified as satisfied, slightly unsatisfied, unsatisfied, or dissatisfied. Exercise habits were classified as daily, 2 to 4 times a week, once a week, or never.
Definition of socioeconomic factors
We questioned residents on whether they changed or lost their jobs after the earthquake.
Definition of evacuation experience
Regarding questions on residence after the earthquake, the residents of the municipalities that were partially designated as evacuation zones were divided into two groups. They included a non-evacuee group comprising residents who stayed in places other than temporary housing or shelters in 2011 and an evacuee group comprising other residents.
Statistical methods
SAS 9.4 software (SAS Institute Inc., Cary, NC) was employed for statistical analyses. Data were expressed as numbers, mean and standard deviation, or percentage. To identify the risk factors for CKD, hazard ratios and 95% confidence intervals for the association between each factor and the incidence of CKD were obtained from crude, age- and sex-adjusted, and multivariate Cox regression analyses. A p value of < 0.05 for a two-tailed test was considered to indicate a significant difference.
Results
During the follow-up, 4,294 residents (1,782 men and 2,512 women) newly met the criteria for CKD onset. The eGFR levels decreased to < 60 mL/min/1.73 m^2^ in 1,562 men and 2,360 women, and proteinuria was detected in 324 men and 204 women. The clinical features of these residents are shown in Table 1. Table 1. Clinical features of the study participants at the beginning of the observationAllIncident CKDNo CKDN = 17,859N = 4,294N = 13,565Follow-up period (years)3.4(1.5)2.2(1.3)3.8(1.3)Age (years)61(10.2)65.1(9.2)59.7(10.1)Height (cm)157.4(8.7)156.3(8.7)157.7(8.7)Weight (kg)59(10.9)59.2(10.9)58.9(10.9)BMI (kg/m^2^)23.7(3.4)24.1(3.4)23.6(3.4)eGFR (mL/min/1.73 m^2^)76(11)67.6(7.1)78.6(10.6)FGLU (mg/dL)101.4(21)102.9(22.3)101(20.5)HbA1c (NGSP)(%)5.5(0.7)5.6(0.7)5.5(0.7)HDL-chol (mg/dL)60.8(15.2)59(14.9)61.3(15.2)LDL-chol (mg/dL)127.1(32)126.5(32)127.3(32)TG (mg/dL)113.5(74.6)119.2(71.3)111.6(75.6)AST (U/L)24.9(14.4)25.7(11.3)24.6(15.2)ALT (U/L)23.2(19.8)23.3(17)23.2(20.6)γ-GT (U/L)36.2(47.7)35.6(46.6)36.4(48)UA (mg/dL)4.9(1.3)5.1(1.3)4.8(1.3)SBP (mmHg)130.9(15.9)133.6(15.6)130.1(15.9)DBP (mmHg)78.7(10.1)79.3(10)78.5(10.2)Data are shown as mean (SD)SD standard deviation, CKD chronic kidney disease, BMI body mass index, eGFR estimated glomerular filtration rate, FGLU fasting plasma glucose, HbA1c hemoglobin A1c, NGSP National Glycohemoglobin Standardization Program, HDL-chol high-density lipoprotein cholesterol, LDL-chol low-density lipoprotein cholesterol, TG triglyceride, AST aspartate aminotransferase, ALT alanine transaminase, γ-GT γ-glutamyl transferase, UA uric acid, SBP systolic blood pressure, DBP diastolic blood pressure
Univariate analyses performed with the CKD onset as the objective variable showed significant differences between residents with and without CKD. These differences were observed in age at enrollment, diabetes mellitus, BMI, dyslipidemia, hypertension, hyperuricemia, K6 score, smoking history, alcohol drinking history, exercise habit, history of job change, history of job loss, and evacuation experience (Table 2). Table 2. Univariate analyses comparing factors in residents who were affected and unaffected by CKDFactorAll (%)Incident CKD (%)No CKD(%)p valueAge < 6511,342(63.5)2014(46.9)9328(68.8) < 0.0001 ≥ 656517(36.5)2280(53.1)4237(31.2)SexMen7333(41.1)1782(41.5)5551(40.9)0.502Women10,526(58.9)2512(58.5)8014(59.1)Diabetes mellitusNo15,893(89.2)3740(87.2)12,153(89.8) < 0.0001Yes1922(10.8)549(12.8)1373(10.2)ObesityBMI < 25.012,058(67.6)2714(63.2)9344(68.9) < 0.0001BMI ≥ 25.05791(32.4)1578(36.8)4213(31.1)DyslipidemiaNo6650(39.4)1437(35.1)5213(40.8) < 0.0001Yes10,211(60.6)2654(64.9)7557(59.2)Hepatic disorderNo12,523(70.1)2986(69.5)9537(70.3)0.339Yes5336(29.9)1308(30.5)4028(29.7)HypertensionNo8888(49.8)1683(39.3)7205(53.2) < 0.0001Yes8948(50.2)2604(60.7)6344(46.8)HyperuricemiaNo16,730(93.7)3904(90.9)12,826(94.6) < 0.0001Yes1129(6.3)390(9.1)739(5.4)K6 score < 1314,227(85.1)3283(83.5)10,944(85.6)0.001 ≥ 132485(14.9)648(16.5)1837(14.4)Smoking habitNever10,779(62.2)2631(63.6)8148(61.8) < 0.0001Former4027(23.2)1052(25.4)2975(22.6)Current2519(14.5)454(11)2065(15.7)Alcohol drinking habitsNever8805(50.3)2226(53.2)6579(49.3) < 0.0001Former448(2.6)134(3.2)314(2.4)Current8266(47.2)1825(43.6)6441(48.3)Level of sleep satisfactionSatisfied4882(33.4)1147(33)3735(33.6)0.553Slightly unsatisfied6754(46.3)1616(46.5)5138(46.2)Unsatisfied2304(15.8)540(15.5)1764(15.9)Dissatisfied656(4.5)170(4.9)486(4.4)Exercise habitDaily2966(17)810(19.4)2156(16.2) < 0.00012 to 4 times a week4286(24.6)1263(30.3)3023(22.7)Once a week2652(15.2)663(15.9)1989(15)Never7553(43.3)1432(34.4)6121(46.1)Job changeNo17,366(97.2)4213(98.1)13,153(97) < 0.0001Yes493(2.8)81(1.9)412(3)Loss of jobNo13,501(75.6)3314(77.2)10,187(75.1)0.006Yes4358(24.4)980(22.8)3378(24.9)Evacuation experienceNo7874(44.3)1809(42.3)6065(44.9)0.002Yes9906(55.7)2472(57.7)7434(55.1)Data are shown as numbers (percentages). Differences between the no CKD and incident CKD groups were analyzed using Chi-squared testCKD chronic kidney disease, BMI body mass index
The age‐ and sex‐adjusted Cox regression analysis identified age, BMI, diabetes mellitus, dyslipidemia, hypertension, hyperuricemia, K6 score, smoking history, alcohol drinking history, and exercise habit as significant factors. The multivariate analysis identified age, BMI, dyslipidemia, hypertension, hyperuricemia, and K6 score as significant factors. In addition, alcohol drinking history and exercise habits were identified as significant inhibitory factors (Table 3). Table 3. Cox regression multivariate analysis to identify factors associated with the onset of CKDFactorAge‐ and sex‐adjusted HR (95%CI)^a^Multivariable‐adjusted HR (95%CI)^b^Older age (ref. AGE < 65)2.29(2.16–2.43)1.96(1.84–2.10)Male sex (Ref. Female)0.96(0.91–1.02)1.02(0.94–1.12)Diabetes mellitus (Ref. No)1.18(1.08–1.29)1.09(0.99–1.19)Obesity (Ref. BMI < 25.0)1.26(1.19–1.35)1.12(1.05–1.20)Dyslipidemia (Ref. No)1.20(1.12–1.28)1.11(1.04–1.19)Hypertension (Ref. No)1.40(1.31–1.49)1.30(1.22–1.39)Hyperuricemia (Ref. No)1.68(1.51–1.86)1.56(1.40–1.73)K6 score (Ref. < 13)1.14(1.05–1.24)1.13(1.04–1.23)Smoking habit (Ref. Never)Former1.09(0.99–1.19)1.09(1.00–1.20)Current0.87(0.78–0.97)0.91(0.81–1.02)Alcohol drinking habit (Ref. Never)Former1.09(0.91–1.31)1.03(0.86–1.23)Current0.87(0.81–0.93)0.85(0.79–0.92)Exercise habit (Ref. Daily)2 to 4 times a week1.11(1.02–1.21)1.09(1.00–1.19)Once a week1.01(0.91–1.12)1.00(0.90–1.11)Never0.89(0.82–0.98)0.89(0.82–0.98)Job change (Ref. No)0.90(0.72–1.13)0.98(0.78–1.22)Loss of job (Ref. No)1.00(0.93–1.08)0.98(0.91–1.06)Evacuation experience (Ref. No)1.05(0.99–1.12)1.03(0.97–1.10)^a^Analysis adjusted by age and sex^b^Analysis adjusted by age, sex, diabetes mellitus, obesity, dyslipidemia, hypertension, hyperuricemia, K6 score, smoking habit, alcohol drinking habit, exercise habit, job change, loss of job, and evacuation experienceCox proportional hazard model, p < 0.05 was considered statistically significant95% CI 95% confidence interval, HR hazard ratio, Ref reference, CKD chronic kidney disease, BMI body mass index, K6 Kessler psychological distress scale
When the objective variable was set to a new decrease characterized by an eGFR level < 60 mL/min/1.73 m^2^, the multivariate analysis identified age, BMI, dyslipidemia, hypertension, hyperuricemia, and K6 score as significant promotional factors. Further, smoking habit, alcohol drinking habit, and exercise habit were identified as significant inhibitory factors (Table 4). Table 4. Cox regression multivariate analysis to identify factors associated with the onset of CKD indicated by eGFR < 60 mL/min/1.73m^3^FactorAge‐ and sex‐adjusted HR (95%CI)^a^Multivariable‐adjusted HR (95%CI)^b^Older age (Ref. AGE < 65)2.47(2.32–2.63)2.08(1.94–2.23)Male sex (Ref. Female)0.90(0.84–0.96)0.96(0.88–1.05)Diabetes mellitus (Ref. No)1.08(0.99–1.19)0.99(0.90–1.09)Obesity (Ref. BMI < 25.0)1.25(1.17–1.33)1.11(1.04–1.19)Dyslipidemia (Ref. No)1.18(1.10–1.26)1.10(1.03–1.18)Hypertension (Ref. No)1.41(1.32–1.51)1.33(1.24–1.42)Hyperuricemia (Ref. No)1.69(1.52–1.88)1.57(1.41–1.75)K6 score (Ref. < 13)1.12(1.02–1.22)1.12(1.02–1.22)Smoking habit (Ref. Never)Former1.09(0.99–1.20)1.10(1.00–1.20)Current0.79(0.70–0.89)0.83(0.74–0.93)Alcohol drinking habit (Ref. Never)Former1.19(0.99–1.43)1.13(0.94–1.35)Current0.87(0.81–0.94)0.86(0.80–0.93)Exercise habit (Ref. Daily)2 to 4 times a week1.09(1.00–1.20)1.08(0.98–1.18)Once a week1.01(0.91–1.12)1.00(0.90–1.11)Never0.87(0.79–0.95)0.87(0.79–0.96)Job change (Ref. No)0.84(0.66–1.07)0.92(0.72–1.17)Loss of job (Ref. No)0.98(0.91–1.06)0.97(0.90–1.05)Evacuation experience (Ref. No)1.02(0.96–1.09)1.01(0.95–1.08)^a^Analysis adjusted by age and sex^b^Analysis adjusted by age, sex, diabetes mellitus, obesity, dyslipidemia, hypertension, hyperuricemia, K6 score, smoking habit, alcohol drinking habit, exercise habit, job change, loss of job, and evacuation experienceCox proportional hazard model, p < 0.05 was considered statistically significant95% CI 95% confidence interval, HR hazard ratio, Ref reference, eGFR estimated glomerular filtration rate, BMI Body mass index, K6 Kessler psychological distress scale
Finally, when the objective variable was set to the onset of proteinuria, the multivariate analysis identified age, sex, diabetes mellitus, BMI, hypertension, hyperuricemia, and smoking habit as significant promotional factors (Table 5). Table 5. Cox regression multivariate analysis to identify factors associated with the onset of proteinuriaFactorAge‐ and sex‐adjusted HR (95%CI)^a^Multivariable‐adjusted HR (95%CI)^b^Older age (Ref. AGE < 65)1.66(1.44–1.92)1.50(1.27–1.76)Male sex (Ref. Female)2.32(2.00–2.69)1.81(1.47–2.23)Diabetes mellitus (Ref. No)2.55(2.17–3.01)2.28(1.93–2.69)Obesity (Ref. BMI < 25.0)1.64(1.42–1.89)1.37(1.18–1.59)Dyslipidemia (Ref. No)1.27(1.08–1.48)1.07(0.91–1.26)Hypertension (Ref. No)1.89(1.61–2.23)1.62(1.37–1.92)Hyperuricemia (Ref. No)1.60(1.27–2.01)1.37(1.09–1.73)K6 score (Ref. < 13)1.16(0.94–1.43)1.11(0.90–1.37)Smoking habit (Ref. Never)Former1.34(1.09–1.64)1.30(1.06–1.59)Current1.74(1.39–2.18)1.83(1.45–2.30)Alcohol drinking habit (Ref. Never)Former1.02(0.69–1.49)0.93(0.64–1.37)Current0.93(0.79–1.10)0.89(0.75–1.05)Exercise habit (Ref. Daily)2 to 4 times a week1.23(1.00–1.52)1.19(0.96–1.46)Once a week0.96(0.74–1.24)0.94(0.72–1.21)Never1.08(0.88–1.34)1.04(0.84–1.29)Job change (Ref. No)0.96(0.57–1.60)1.03(0.61–1.72)Loss of job (Ref. No)1.20(1.02–1.42)1.12(0.94–1.33)Evacuation experience (Ref. No)1.17(1.01–1.35)1.08(0.93–1.26)^a^Analysis adjusted by age and sex^b^Analysis adjusted by age, sex, diabetes mellitus, obesity, dyslipidemia, hypertension, hyperuricemia, K6 score, smoking habit, alcohol drinking habit, exercise habit, job change, loss of job, and evacuation experienceCox proportional hazard model, p < 0.05 was considered statistically significant95% CI 95% confidence interval, HR hazard ratio, Ref Reference, BMI body mass index, K6 Kessler psychological distress scale
To clarify the impact of psychological stress on the onset of chronic CKD, participants were divided into two groups based on their K6 scores: ≥ 13 and < 13. There were no significant differences in baseline characteristics that might influence CKD development between these groups (Table 6). Furthermore, the group with a K6 score ≥ 13 showed a significantly greater annual decline in eGFR—defined as (baseline eGFR–most recent eGFR) divided by the follow-up period—compared to the group with a K6 score < 13, even after adjustment for multiple confounding variables (Table 7). Table 6. Baseline characteristics of participants according to K6 score categoryK6 < 13 ≥ 13p valueN = 14,227N = 2,485Follow-up period (years)Age (years)60.6 (10.1)60.6(10.0)0.893Height (cm)157.9 (8.6)156.2 (8.4) < 0.0001Weight (kg)59.4 (10.9)57.8 (11.0) < 0.0001BMI (kg/m^2^)23.7 (3.4)23.6 (3.6)0.086eGFR (mL/min/1.73 m^2^)76.1 (11.1)76.0 (10.6)0.609FGLU (mg/dL)101.5 (20.8)100.6 (22.0)0.081HbA1c (NGSP)(%)5.5 (0.7)5.5 (0.7)0.571HDL-chol (mg/dL)60.8 (15.2)61.1 (15.2)0.365LDL-chol (mg/dL)127.4 (31.8)126.5 (32.8)0.239TG (mg/dL)113.5 (75.0)114.1 (78.5)0.723AST (U/L)24.9 (13.9)24.6 (17.6)0.512ALT (U/L)23.4 (20.3)22.9 (18.4)0.216γ-GT (U/L)37.0 (48.7)33.7 (45.7)0.001UA (mg/dL)4.9 (1.3)4.7 (1.2) < 0.0001SBP (mmHg)130.9 (15.9)129.9 (16.0)0.003DBP (mmHg)78.8 (10.2)78.0 (10.2)0.0006Data are shown as mean (SD)SD standard deviation, CKD chronic kidney disease, BMI body mass index, eGFR estimated glomerular filtration rate, FGLU fasting plasma glucose, HbA1c hemoglobin A1c, NGSP National Glycohemoglobin Standardization Program, HDL-chol high-density lipoprotein cholesterol, LDL-chol low-density lipoprotein cholesterol, TG triglyceride, AST aspartate aminotransferase, ALT alanine transaminase, γ-GT γ-glutamyl transferase, UA uric acid, SBP systolic blood pressure, DBP diastolic blood pressureTable 7Comparison of eGFR decline between high and low K6 score groupsFactorParameter estimate95%CIPr >|t|K6 score (Ref. < 13)3.6811.234 to 6.1280.003Analysis adjusted by age, sex, diabetes mellitus, obesity, dyslipidemia, hypertension, hyperuricemia, smoking habit, alcohol drinking habit, exercise habit, job change, loss of job, and evacuation experience. Multiple regression analysis, p < 0.05 was considered statistically significant95% CI 95% confidence interval
Discussion
This study included 17,859 residents of the Futaba District, of whom 4644 or approximately 24% developed CKD within 5 years. This incidence rate is slightly higher than that in a previous study involving a cohort of residents with stable living conditions in Japan [11].
Hypertension, diabetes mellitus, smoking habit [12–14], metabolic syndrome [15], and hyperuricemia [16] show positive associations with the onset and progression of CKD, and high alcohol consumption promote CKD [17]. The data in this study were generally consistent with these conclusions. However, the prevalence of hypertension [18], diabetes mellitus [19], and metabolic syndrome [20] is reportedly associated with the evacuation after the Great East Japan Earthquake and the nuclear power plant accident. Thus, they may be indirectly associated with the earthquake disaster. The prevalence of dyslipidemia [21] was confirmed to have increased after the disaster, which may be associated with CKD progression [22]. It is assumed that hepatic dysfunction may be associated with renal disease [23] or that both may have resulted from metabolic syndrome.
This study shows that a high K6 score promotes the onset and progression of CKD. The K6 score is a tool developed for screening mental disorders, and it is widely employed in public surveys as an index for the degree of any mental problem, including psychological stress [8]. Earthquakes induce severe psychological stress in disaster victims [24], as evidenced by the generally high K6 scores observed in the present cohort. In particular, a K6 score ≥ 13 points, considered to reflect mood-disorder levels that cause social dysfunction, was found, for the first time, to be significantly associated with a decrease in eGFR to < 60 mL/min/1.73 m^2^.
A high incidence of depression has been noted in patients with CKD at the pre-dialysis stage [25]. Studies have reported that depression detected by screening with the Beck Depression Inventory is associated with a secondary outcome of an eGFR-level-related decrease in patients with CKD at the pre-dialysis stage [26]. Furthermore, studies on patients with CKD at the pre-dialysis stage [27] or dialysis stage [28] have revealed that depression is associated with a poor prognosis. However, because patients with established CKD were the subjects of these studies, it could not be concluded whether emotional disturbance was a cause or a result of the worse clinical outcome. We examined residents without CKD and derived an association between depression and decreased eGFR levels. To the best of our knowledge, this is the first report of this finding, attributable to the highly specific nature of the cohort (i.e., a public cohort with shared experiences of potentially stressful situations).
A depressive state has been associated with glomerular hyperfiltration [29], possibly providing an important pathophysiological explanation for the association between a high K6 score and decreased eGFR levels. Hypertension has been reported to increase not only after the Great East Japan Earthquake [30] but also after many natural disasters [31]. This type of hypertension, designated disaster hypertension, is considered to mainly arise through the stress-dependent hyperactivation of the sympathetic nervous system [32]. This condition is another possible mediator of renal damage through the contraction of the glomerular afferent artery and the subsequent activation of the renin–angiotensin–aldosterone system that causes glomerular hyperfiltration. Indeed, it has been suggested that at least part of the effect of stress on renal function may be mediated through its influence on blood pressure and glucose metabolism [33]. In addition to its potential direct effects on the kidneys, stress may also contribute to the onset and progression of CKD by altering behavioral patterns, including dietary habits and healthcare-seeking behaviors.
Although many of the residents in the Futaba District were evacuated to avoid radiation exposure, the exposure levels were low not only in the evacuees but also in the residents who did not evacuate [34, 35]. Radiation-induced renal injury, when it occurs, is typically delayed in onset, with hematopoietic, gastrointestinal, and cutaneous toxicities expected to manifest earlier [36]. However, surveys have not identified such radiation-related conditions among residents of the Futaba region. Thus, we consider that radiation is unlikely to have directly affected the changes in renal function in the present study. Thus, we did not consider radiation exposure as a direct cause of CKD in this study. We do not negate the possibility of radiation‐derived health injuries in the future. However, from a scientific standpoint, it is inappropriate to conclude that all ailments afflicting the residents of the Futaba District must be related to radiation exposure.
This study has several limitations. Under standard diagnostic criteria, confirmation of chronic kidney disease (CKD) requires evidence that reduced eGFR or proteinuria persists for at least 3 months. However, in this study, data were available only once annually, and therefore CKD was defined based on a single observation of reduced eGFR or proteinuria. This operational decision was unavoidable given the nature of this cohort, and the same criterion has been used in prior studies utilizing this dataset. Nonetheless, we acknowledge that this approach does not allow exclusion of transient abnormalities and represents a clear limitation of the study. One of the common pathways for CKD progression is glomerular hyperfiltration. In this case, the eGFR level increases transiently and subsequently decreases. This may also be true in individuals suffering from depression [29], as discussed above. Even when some factors adversely affect the kidney through hyperfiltration, a cohort will likely include individuals with both increased and decreased eGFR levels during a longitudinal observation study. Thus, the impact of psychological stress on the kidney may be considerably more severe than that revealed in the present study. A similar bias may also apply to smoking. Nicotine is known to induce glomerular hyperfiltration through the upregulation of COX-2 expression [37], and this hyperfiltration is understood to contribute to long-term renal damage. In fact, some observational studies with short follow-up periods have reported that smoking was associated with the onset of proteinuria, while paradoxically showing higher GFR values in many cases [38]. In the present study as well, smoking appeared to be associated with an increased incidence of proteinuria but a seemingly attenuated decline in renal function. However, this should be interpreted as a consequence of glomerular hyperfiltration, and not as evidence against the nephrotoxic effects of smoking.
This cohort was established after the Great East Japan Earthquake, and therefore lacks pre-disaster data. It is generally recognized that acute elevations in blood pressure frequently occur following natural disasters [32], and particularly after the Great East Japan Earthquake, a pronounced increase in blood pressure was reported among patients with chronic kidney disease [18]. However, this study could not distinguish between individuals with disaster-related acute hypertension and those with preexisting essential hypertension. Similarly, it was not possible to differentiate participants with elevated K6 scores that developed after the earthquake from those who had high scores prior to the disaster. Although the renal consequences may differ between these subgroups, our inability to disentangle them constitutes a limitation of this study.
Other limitations of this study include the use of the dipstick method for proteinuria assessment, which is less reliable than quantitative measurements; the fact that both proteinuria and eGFR were measured only once annually; the fact that information on lifestyle habits was obtained through self-administered questionnaires with unverified accuracy; and that many of the evaluated factors, including the K6 score, were assessed only at baseline. Furthermore, as the response rate to the questionnaire was limited to 40.7%, it is possible that the results do not fully reflect the overall population trends. Another limitation of this study is the absence of data on treatment status for hyperuricemia and liver dysfunction.
However, the present study is still targeted a highly specific cohort within the public that shared an experience with potentially stressful situations. The sample size was sufficiently large. The results revealed that severe stress is associated with decreased eGFR levels. This finding is sufficiently reliable and may contribute to future clinical practices and studies.
In conclusion, a longitudinal analysis of data obtained from the health checkups of the residents of the Futaba District who were severely affected by the disaster was conducted. The results revealed that CKD onset, particularly characterized by a decrease in the eGFR level, is associated with severe stress, in addition to known associated factors. Even more than a decade after the disaster, residents of the Futaba region continue to experience stressful lives due to persistent stigma and discrimination. Evaluating whether stress management can suppress the onset and progression of CKD represents the next challenge to be addressed. If the mechanism by which stress induces renal impairment involves the induction of glomerular hyperfiltration, then stress management may at least have the potential to delay CKD progression. Fortunately, a comprehensive health screening system has been established in the Futaba area following the nuclear accident, enabling continuous monitoring of residents’ health status. In parallel, the regional medical service infrastructure has also been reinforced. Should active stress interventions prove effective, they may offer a novel therapeutic option in the management of CKD.