Lead Toxicity Masquerading as Autoimmune Haemolytic Anaemia: A Diagnostic Pitfall in Unexplained Anaemia
John Ee Chew, Nathan Klose

TL;DR
A case of lead poisoning mistaken for autoimmune anemia shows the importance of checking for toxic exposure in unexplained blood disorders.
Contribution
Highlights lead toxicity as an under-recognized cause of unexplained anemia mimicking autoimmune haemolytic anaemia.
Findings
Lead toxicity can mimic autoimmune haemolytic anaemia with similar hematological features.
Peripheral blood morphology and exposure history are crucial for accurate diagnosis.
Chelation therapy improved clinical and hematological outcomes in this case.
Abstract
Lead toxicity is an uncommon but clinically important cause of unexplained anaemia. Its heterogeneous haematological manifestations can mimic autoimmune haemolytic anaemia, resulting in diagnostic uncertainty and delayed recognition. A 49-year-old woman presented with a three-week history of worsening abdominal pain and lethargy. She had a background of inclusion body myositis treated with long-term intravenous immunoglobulin and recent initiation of mycophenolate mofetil. Initial investigations demonstrated severe anaemia with reticulocytosis but minimal biochemical evidence of haemolysis. A weakly positive direct antiglobulin test (IgG 1+, C3d negative) raised suspicion for autoimmune haemolysis. The initial peripheral blood film was reported as showing marked red cell agglutination without additional abnormalities. Progressive anaemia prompted extensive investigations, including…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
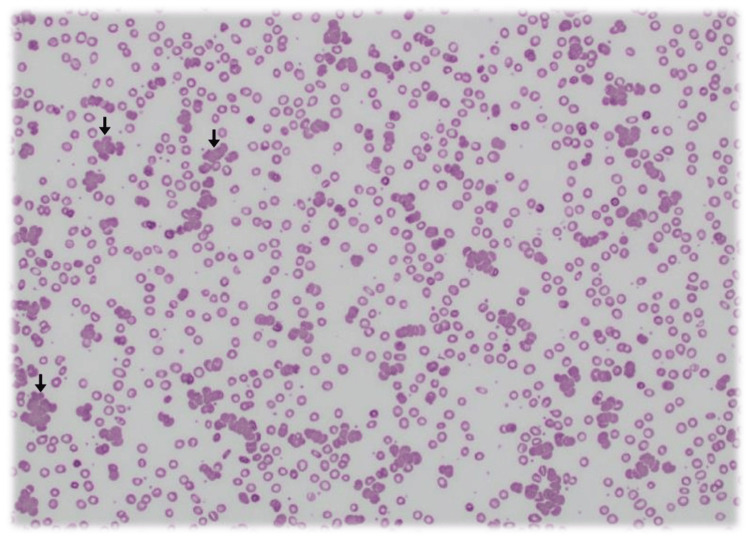 Figure 1
Figure 1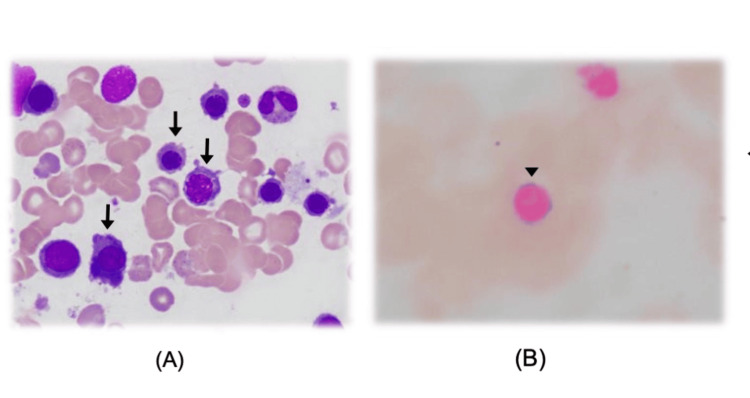 Figure 2
Figure 2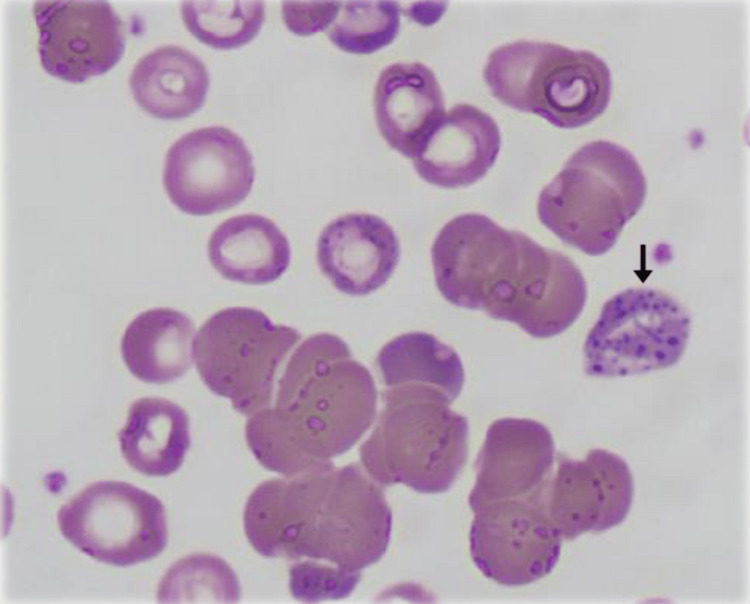 Figure 3
Figure 3| Parameter | 04/04/22 | 13/07/22 (Admission) | Reference Range | Units |
| Haemoglobin | 127 | 72 ↓ | 115–165 | g/L |
| Haematocrit | 0.38 | 0.22 ↓ | 0.35–0.47 | - |
| Red Cell Count (RCC) | 4.1 | 2.4 ↓ | 3.9–5.6 | 10¹²/L |
| Reticulocytes | - | 190 ↑ | 25–120 | 10⁹/L |
| Mean Cell Volume (MCV) | 93 | 93 | 80–100 | fL |
| White Cell Count (WCC) | 4.5 | 4.9 | 3.5–12.0 | 10⁹/L |
| Platelets | 183 | 214 | 150–400 | 10⁹/L |
| Test Name | Result | Units | Reference Interval |
| Iron | 24 | umol/L | 5 - 30 |
| Transferrin | 1.8 L | g/L | 1.9 - 3.1 |
| TIBC | 45 L | umol/L | 47 - 77 |
| Saturation | 53 H | % | 20 - 45 |
| Ferritin | 165 | ug/L | 30 - 300 |
| CRP | <0.4 | mg/L | <5 |
| Vitamin B12 | 375 | pmol/L | >150 |
| Active B12 | >128 | pmol/L | >35 |
| Folate (Serum) | 39 | nmol/L | >7.0 |
| Bilirubin | 29 H | umol/L | <16 |
| Alk Phos | 42 | U/L | 20 - 105 |
| AST | 56 H | U/L | 10 - 35 |
| ALT | 68 H | U/L | 5 - 30 |
| Gamma GT | 13 | U/L | 5 - 35 |
| LDH | 339 H | U/L | 120 - 250 |
| Cholesterol | 4.5 | mmol/L | <5.6 |
| CK | 481 H | U/L | 30 - 150 |
| Magnesium | 0.82 | mmol/L | 0.70 - 1.10 |
| Haemolysis Index | 4 | <40 | |
| Haptoglobin | 0.20 | g/L | 0.16 - 2.00 |
| Direct Coombs Test | Positive | ||
| Anti-IgG | 1+ | (Scale 1 to 4) | |
| Anti-C3d | Non Reactive | (Scale 1 to 4) | |
| Antibody Screen | Negative | ||
| Blood Group | A Rh(D) Positive |
| Test | Result | Units | Reference Interval |
| Albumin | 40 | g/L | 33 - 46 |
| Alpha 1 | 2 | g/L | 2 - 4 |
| Alpha 2 | 4 | g/L | 4 - 9 |
| Beta 1 | 3 | g/L | 2 - 6 |
| Beta 2 | 1.5 | g/L | 2 - 6 |
| Gamma | 15 | g/L | 6 - 15 |
| Total Protein | 67 | g/L | 64 - 81 |
| Immunofixation | No Monoclonal Immunoglobulin Detected | ||
| Immunoglobulin G (IgG) | 14.90 | g/L | 5.76 - 15.36 |
| Immunoglobulin A (IgA) | 1.12 L | g/L | 1.24 - 4.16 |
| Immunoglobulin M (IgM) | 1.79 | g/L | 0.48 - 3.1 |
| Kappa Free Light Chains | 30 H | mg/L | 7 - 22 |
| Lambda Free Light Chains | 37 H | mg/L | 8 - 27 |
| K/L Ratio | 0.81 | 0.31 - 1.56 |
| Test | 14/07/22 | 15/07/22 | 16/07/22 | 17/07/22 | 18/07/22 | 19/07/22 | Reference | Units |
| Haemoglobin | 72 L | 77 L | 72 L | 64 L | 75 L | 66 L | (115 - 165) | g/L |
| Haematocrit | 0.21 L | 0.23 L | 0.22 L | 0.20 L | 0.23 L | 0.20 L | (0.35 - 0.47) | L/L |
| RCC | 2.3 L | 2.5 L | 2.4 L | 2.1 L | 2.5 L | 2.1 L | (3.9 - 5.6) | 10^12/L |
| Reticulocytes | 193 H | 234 H | 202 H | 286 H | (25 - 120) | 10^9/L | ||
| MCV | 91 | 93 | 92 | 94 | 94 | 93 | (80 - 100) | fL |
| WCC | 5.0 | 5.2 | 6.2 | 5.2 | 5.6 | 7.1 | (3.5 - 12.0) | 10^9/L |
| Neutrophils | 3.06 | 2.86 | 3.71 | 2.68 | 3.44 | 4.59 | (1.5 - 8.0) | 10^9/L |
| Lymphocytes | 1.39 | 1.79 | 1.87 | 1.97 | 1.71 | 1.74 | (1.0 - 4.0) | 10^9/L |
| Monocytes | 0.50 | 0.40 | 0.48 | 0.43 | 0.38 | 0.67 | (0.0 - 0.9) | 10^9/L |
| Eosinophils | 0.05 | 0.10 | 0.13 | 0.09 | 0.10 | 0.13 | (0.0 - 0.6) | 10^9/L |
| Basophils | 0.00 | 0.00 | 0.01 | 0.01 | 0.01 | 0.01 | (0.0 - 0.15) | 10^9/L |
| NRBC | 1.0 H | (0) | 10^9/L | |||||
| Platelets | 200 | 246 | 217 | 201 | 205 | (150 - 400) | 10^9/L | |
| T Bilirubin | 27 H | 32 H | 25 H | 19 H | 17 H | 12 | (<16) | umol/L |
| ALP | 39 | 44 | 41 | 34 | 41 | 36 | (20 - 105) | U/L |
| AST | 45 H | 46 H | 47 H | 41 H | 52 H | 48 H | (10 - 35) | U/L |
| ALT | 58 H | 55 H | 54 H | 47 H | 60 H | 55 H | (5 - 30) | U/L |
| GGT | 13 | 15 | 16 | 13 | 15 | 15 | (5 - 35) | U/L |
| LDH | 273 H | 337 H | 302 H | 243 | 284 H | 258 H | (120 - 250) | U/L |
| Test | Result | Units | Reference Range |
| Lead-blood | 3.76 H | umol/L | 0 - 0.24 |
| Lead-blood | 77.8 H | ug/dL | 0 - 5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeavy Metal Exposure and Toxicity · Blood groups and transfusion · Trace Elements in Health
Introduction
Lead poisoning remains a rare but serious condition and can originate from traditional remedies, including Ayurvedic medicine. These supplements sometimes contain toxic heavy metals, intentionally or via contamination, posing risks of haematologic, renal, and neurologic toxicity [1,2]. Among its haematological manifestations, lead toxicity may present with anaemia, reticulocytosis, and basophilic stippling and can mimic haemolytic disorders, particularly autoimmune haemolytic anaemia (AIHA), resulting in diagnostic confusion [2-4].
Mechanistically, lead interferes with key enzymes in the haem biosynthesis pathway, including δ-aminolevulinic acid dehydratase and ferrochelatase, resulting in impaired haem production, ineffective erythropoiesis, and characteristic morphological findings such as coarse basophilic stippling and sideroblastic features [4,5]. Inhibition of pyrimidine-5′-nucleotidase further contributes to the accumulation of ribosomal RNA in red cells, producing the stippling seen on peripheral blood smears [6]. These changes, along with red cell destruction and marrow erythroid hyperplasia, can closely resemble immune-mediated haemolysis.
Diagnostic challenges arise when partial or misleading findings, such as a weakly positive direct antiglobulin test or red cell agglutination, suggest AIHA, particularly in patients receiving immunosuppressive therapy. For example, intravenous immunoglobulin (IVIG) has been associated with false-positive Coombs tests, further complicating interpretation [7]. Without prominent biochemical markers of haemolysis, clinicians may pursue extensive immunologic and haematologic evaluations while overlooking toxic or environmental causes.
Here, we report a diagnostically challenging case of lead toxicity masquerading as autoimmune haemolytic anaemia in a patient receiving long-term immunosuppressive therapy. This case underscores the importance of thorough exposure history, including use of unregulated supplements, and careful peripheral blood smear review in evaluating unexplained anaemia. Although lead toxicity from traditional remedies has been reported, its presentation as an AIHA mimic remains under-recognised [3,4,8]. Our case highlights a key diagnostic pitfall and reinforces the need for a structured and vigilant approach in similar clinical scenarios.
Case presentation
A 49-year-old woman presented with a three-week history of worsening abdominal pain and progressive lethargy. Her medical history included inclusion body myositis managed with long-term intravenous immunoglobulin (IVIG) and recent initiation of mycophenolate mofetil. There was no recent infection, gastrointestinal bleeding, or known toxin exposure reported initially.
Admission laboratory results revealed marked normocytic anaemia with haemoglobin of 72 g/L and reticulocytosis of 190 × 10⁹/L (Table 1), suggestive of an appropriate marrow response (Appendix). However, markers of biochemical haemolysis were only modestly abnormal (Table 2): total bilirubin was 29 µmol/L (reference <16 µmol/L), lactate dehydrogenase (LDH) was mildly elevated at 339 U/L (reference 120-250 U/L), and haptoglobin was low-normal at 0.20 g/L (reference 0.16-2.00 g/L). A direct antiglobulin test (DAT) was weakly positive for IgG (1+) but negative for C3d, raising initial suspicion for warm autoimmune haemolytic anaemia (AIHA). The initial peripheral blood film reported by the laboratory haematologist described marked red cell agglutination without other abnormalities (Figure 1).
Peripheral blood smear at initial presentation Marked red blood cell agglutination (arrows), which led to a presumptive diagnosis of autoimmune haemolytic anaemia. This morphological finding, in conjunction with a weakly positive direct antiglobulin test, supported the initial working diagnosis.
Given the diagnostic uncertainty, an extensive workup was undertaken, including viral serologies (EBV, Mycoplasma), autoimmune screens, cold agglutinin titres, and urinary haemosiderin, all of which were unremarkable (Table 3). Despite these investigations, the patient’s haemoglobin continued to decline, prompting a bone marrow aspirate. This revealed dyserythropoietic features and coarse basophilic stippling (Figure 2), which are characteristic of lead poisoning.
Bone marrow aspirate filmA) Peripheral blood smear (May-Grünwald-Giemsa stain) demonstrating dyserythropoietic features, including coarse basophilic stippling (arrows), within erythrocytes. Basophilic stippling represents precipitated ribosomal RNA caused by pyrimidine-5′-nucleotidase inhibition—a hallmark of lead toxicity.(B) Iron stain (Prussian Blue) highlighting a ring sideroblast (arrowhead), indicative of mitochondrial iron loading due to impaired heme synthesis. This finding reflects ineffective erythropoiesis, consistent with lead-induced disruption of ferrochelatase activity in the heme biosynthetic pathway. The combination of basophilic stippling and ring sideroblasts provided key morphological evidence supporting the diagnosis of lead poisoning, which had initially been overlooked.
In view of the bone marrow findings, a re-examination of the initial peripheral smear was performed. On closer inspection, previously overlooked features, basophilic stippling, were identified (Figure 3), raising strong suspicion for heavy metal toxicity, particularly lead [3,4]. At this point, a targeted exposure history was revisited, during which the patient disclosed recent ingestion of an unlabelled herbal supplement provided by a friend.
Re-examination of the initial peripheral blood filmCoarse basophilic stippling (arrow) within erythrocytes. These features—initially overlooked—are classic morphological clues of lead toxicity and prompted confirmatory toxicology testing.
Toxicology testing confirmed markedly elevated blood lead levels. The patient was promptly commenced on oral chelation therapy with succimer after consultation with a toxicology specialist. This led to progressive haematological recovery and symptomatic improvement (Tables 4, 5). The case was reported to public health authorities, who confirmed the supplement as the source of lead, arsenic, and mercury contamination and coordinated community-level mitigation.
**Table 5: Blood lead levels and interpretation guidelinesGuidelines for blood lead interpretation:1. No workplace exposure:
- Blood lead > 5 µg/dL (0.24 µmol/L): the source of exposure should be investigated and removed.
- Chelation therapy (adults) is considered if blood lead is > 69.9 µg/dL (3.33 µmol/L) or if symptoms of high exposure are present.**
Discussion
Lead poisoning remains an uncommon but clinically important cause of unexplained anaemia and abdominal pain, and it can masquerade as autoimmune or microangiopathic haemolytic processes [2-4]. Lead interferes with several enzymes in the haem biosynthesis pathway (notably δ-aminolevulinic acid dehydratase and ferrochelatase), producing impaired haem synthesis, accumulation of erythroid precursors, and characteristic morphological changes such as coarse basophilic stippling and sideroblastic features [4,5].
Basophilic stippling, coarse, blue granular inclusions within erythrocytes on a Wright/Giemsa stain, results from the precipitation of ribosomal RNA caused by inhibition of pyrimidine-5′-nucleotidase and is a classic morphologic clue to lead [6]. Because basophilic stippling may be focal or subtle, it can be overlooked when more prominent or competing smear findings (for example, marked agglutination or numerous nucleated red cells) are present; careful review by an experienced haematologist or repeat slide review is therefore often decisive.
Traditional and herbal medicines, including some Ayurvedic preparations, are a well-documented source of lead and other heavy-metal exposures worldwide [1,5,7]. Surveys and case series have repeatedly identified products containing lead, mercury, or arsenic, and individual case reports describe lead toxicity temporally associated with ingestion of such preparations [1,5,7]. This exposure pathway is an especially important diagnostic consideration when patients report use of complementary or alternative medicines and when routine environmental or occupational risks are absent.
Clinically, lead-related presentations are protean: vague constitutional complaints, abdominal pain (historically “saturnine colic”), constipation, neuropsychiatric symptoms, and haematologic abnormalities may all occur depending on dose and chronicity [2,3]. Because lead-induced anaemia can clinically and biochemically mimic autoimmune haemolysis or microangiopathic haemolytic anaemia (MAHA), a structured approach is required. Basic investigations should include a peripheral blood smear (with attention to stippling and schistocytes), a full haemolysis panel (reticulocyte count, LDH, bilirubin fractionation, haptoglobin), a direct antiglobulin test (to exclude immune haemolysis), and iron studies/B12/folate as indicated. In the setting of anaemia with basophilic stippling or suggestive exposure history, measurement of a venous blood lead level (BLL) is the diagnostic test of choice [8].
Management priorities are removal from exposure, supportive care, and consideration of chelation for symptomatic or sufficiently high BLLs. International and national guidance outline thresholds and clinical context for chelation; oral dimercaptosuccinic acid (succimer; DMSA) is commonly used for moderate toxicity and has established dosing regimens, whereas parenteral chelators (e.g., EDTA ± dimercaprol) are reserved for severe or encephalopathic cases and should be managed with toxicology input [8,9]. Chelation reduces circulating lead and ameliorates many acute manifestations, but clinical recovery also depends on elimination of the exposure source and supportive measures [8-10].
This case highlights three practical points for clinicians. First, an exhaustive medication and supplement history, including traditional, imported, or over-the-counter preparations, is essential when evaluating unexplained anaemia or abdominal pain [1,5]. Second, the peripheral smear remains a high-yield diagnostic tool: basophilic stippling, when present, should trigger urgent consideration of toxic exposures and directed testing [6]. Third, liaison with local toxicology/poisons services and public-health authorities is important both for individual patient management (chelation decisions, follow-up BLL monitoring) and for community risk mitigation when contaminated products are implicated [8,9].
Conclusions
This case highlights the diagnostic complexity of lead toxicity, particularly when it presents with features suggestive of alternative aetiologies such as autoimmune haemolytic anaemia. While lead poisoning was ultimately identified, the diagnosis was delayed in part due to missed early clues, namely, basophilic stippling and ring sideroblasts, which were recognised only in retrospective review. This underscores not only the diagnostic value of peripheral smear examination and exposure history but also the potential for initial oversight. Rather than suggesting these elements are routinely sufficient for early diagnosis, this case illustrates the need for heightened clinical suspicion and systematic re-evaluation in cases of unexplained anaemia. Overall, this case offers valuable insight into the pitfalls and learning points surrounding the diagnostic journey in lead toxicity and emphasises the importance of considering environmental exposures even when initial findings are ambiguous.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lead, mercury, and arsenic in US- and Indian-manufactured Ayurvedic medicines sold via the Internet JAMA Saper RB Phillips RS Sehgal A 91592330020081872826510.1001/jama.300.8.915PMC 2755247 · doi ↗ · pubmed ↗
- 2Lead toxicity: a review Interdiscip Toxicol Wani AL Ara A Usmani JA 5564820152748636110.1515/intox-2015-0009 PMC 4961898 · doi ↗ · pubmed ↗
- 3Chronic lead poisoning induced abdominal pain and anemia: a case report and review of the literature BMC Gastroenterol Yang Y Li S Wang H 335202020 https://pubmed.ncbi.nlm.nih.gov/33054779/3305477910.1186/s 12876-020-01482-x PMC 7557016 · doi ↗ · pubmed ↗
- 4Toxicity of lead: A review with recent updates Interdiscip Toxicol Flora G Gupta D Tiwari A 4758520122311858710.2478/v 10102-012-0009-2PMC 3485653 · doi ↗ · pubmed ↗
- 5A case of chronic lead poisoning with herbal-based medication BMJ Case Rep Jain S Gupta A Ray A Vikram NK 12201910.1136/bcr-2018-227954 PMC 645326330940669 · doi ↗ · pubmed ↗
- 6Non-occupational lead poisoning associated with traditional Chinese medicine: a case report Front Public Health Ma H Wu LM Zou Y Li XA 9381861020223617651410.3389/fpubh.2022.938186 PMC 9513390 · doi ↗ · pubmed ↗
- 7Heavy metal content of ayurvedic herbal medicine products JAMA Saper RB Kales SN Paquin J 2868287329220041559891810.1001/jama.292.23.2868 · doi ↗ · pubmed ↗
- 8Recommendations for medical management of adult lead exposure Environ Health Perspect Kosnett MJ Wedeen RP Rothenberg SJ 4634711152006 https://pmc.ncbi.nlm.nih.gov/articles/PMC 1849937/1743150010.1289/ehp.9784 PMC 1849937 · doi ↗ · pubmed ↗