Effects of Sodium Glucose Cotransporter 2 (SGLT2) Inhibitors on Lipid Profiles in Type 2 Diabetes: A Systematic Review
Mushrega Abdalla, Mudathir Elyas Suleiman Khamees, Ahmed-Lamin Gehani, Abubaker Ibrahim Mohammed Ibrahim, Muntassir Y Yousif, Noor Kheir, Safa Mohammed Qasem Alqasem, Asim Ahmed

TL;DR
This paper reviews how SGLT2 inhibitors affect lipid levels in people with type 2 diabetes, finding mostly neutral to slightly positive effects on cholesterol and triglycerides.
Contribution
The study systematically evaluates the lipid effects of SGLT2 inhibitors, highlighting inconsistencies in advanced lipid measures and the need for standardized reporting.
Findings
SGLT2 inhibitors show a neutral effect on LDL cholesterol in type 2 diabetes patients.
They tend to favorably affect HDL cholesterol and triglycerides in some settings.
Results on advanced lipid markers remain inconsistent across studies.
Abstract
Sodium glucose cotransporter 2 (SGLT2) inhibitors provide cardiometabolic benefits in adults with type 2 diabetes mellitus, yet their effects on lipid metabolism are reported inconsistently across clinical trials and mechanistic studies and may vary with background statin therapy and differences in lipid measurement and reporting. We conducted a systematic review to evaluate the impact of SGLT2 inhibitors on conventional lipid parameters first and selected advanced lipid markers second in adults with type 2 diabetes. We searched multiple databases using predefined eligibility criteria and extracted data in duplicate. We assessed the risk of bias using design-appropriate tools and synthesized findings qualitatively because heterogeneity limited quantitative pooling. Overall, evidence across included studies suggests that SGLT2 inhibitors are essentially neutral with respect to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
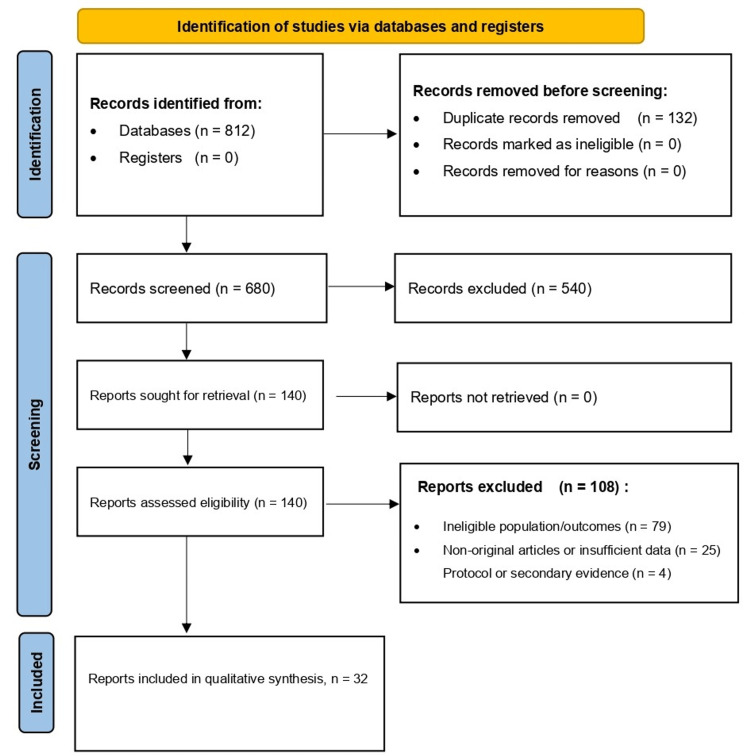 Figure 1
Figure 1| PICOS element | Definition in this review |
| Population (P) | Adults (≥18 years) with type 2 diabetes mellitus, with or without comorbid cardiovascular disease, heart failure, nephropathy, obesity, metabolic syndrome, or NAFLD/MASLD, provided lipid outcomes were reported. |
| Intervention (I) | Any SGLT2 inhibitor at any approved dose (e.g., empagliflozin, dapagliflozin, canagliflozin, ertugliflozin; others where eligible). |
| Comparator (C) | Placebo, usual care, or active non-SGLT2 glucose-lowering therapy (e.g., DPP-4 inhibitors, GLP-1 receptor agonists, insulin-based regimens). |
| Outcomes (O) – Primary | Changes in LDL-C, HDL-C, triglycerides, and total cholesterol (absolute change, % change from baseline, or between-group difference). |
| Outcomes (O) – Secondary | Body weight/anthropometrics; glycaemic markers (fasting plasma glucose, HbA1c); insulin resistance indices; advanced/mechanistic lipid outcomes where available (e.g., LDL subfractions, HDL subtypes, ANGPTL3, ApoB48). |
| Study design (S) | Randomized controlled trials and prospective/retrospective observational cohort studies with extractable quantitative lipid data pre/post SGLT2 inhibitor therapy. |
| Exclusions | Case reports/series, narrative reviews/editorials, nonhuman studies, and reports without extractable lipid outcomes; non-English; non-full text. |
| Timeframe | No date restrictions (database inception to August 2025). |
| Component | Details |
| Databases searched | MEDLINE (via PubMed), Embase, Web of Science, Cochrane Library |
| Coverage | From database inception to August 2025 |
| Core concepts combined | (1) SGLT2 inhibitors, (2) type 2 diabetes mellitus, (3) lipid outcomes |
| Keywords (examples reported) | “sodium glucose cotransporter 2”, “SGLT2 inhibitor”, empagliflozin, dapagliflozin, canagliflozin, ertugliflozin; “type 2 diabetes”; cholesterol, LDL, HDL, triglycerides, dyslipidaemia |
| Search fields | Titles/abstracts/keywords; controlled vocabulary where applicable |
| Other sources | Manual screening of reference lists of key RCTs and relevant systematic reviews; conference abstracts from major diabetes/cardiology meetings (2023–2025), used for context if quantitative data were insufficient |
| Record handling | Imported into reference management software; duplicates removed before screening |
| Authors (Year) | Study Design | Population | SGLT2 Intervention | Comparator | N | Duration | Key Lipid Changes (LDL-C, HDL-C, TG, TC) | Mechanistic or Key Findings to Cite | Country |
| Kahl et al. (2020) [ | Randomized, double-blind, placebo-controlled, phase 4 | Well-controlled type 2 diabetes mellitus | Empagliflozin | Placebo | Not reported | Not reported | Not primarily a lipid trial | Empagliflozin lowers liver fat content | Germany |
| Lauritsen et al. (2022) [ | Randomized, double blind, crossover | Type 2 diabetes mellitus on metformin | Empagliflozin 10 mg daily | Placebo | 13 | 4 weeks | Not extracted | Increased visceral adipose tissue free fatty acid uptake and reduced GLUT4 expression in abdominal subcutaneous adipose tissue | Denmark |
| Fadini et al. (2017) [ | Randomized, placebo controlled | Type 2 diabetes mellitus | Dapagliflozin 10 mg | Placebo | 33 randomized, 31 completed | 12 weeks | Not extracted | Focus on HDL function and cholesterol efflux capacity, no consistent changes after adjustment | Italy |
| Hayashi et al. (2017) [ | Randomized, prospective, single center | Type 2 diabetes mellitus on oral agents | Dapagliflozin | Sitagliptin | 80, 40 per group | 12 weeks | Reduced small dense LDL-C, increased HDL2 C, reduced TG, values not extracted | Shift in LDL particle profile and HDL subfractions with dapagliflozin compared with sitagliptin | Japan |
| Zinman et al. (2015) [ | Randomized controlled trial, cardiovascular outcome trial, EMPA REG OUTCOME | Type 2 diabetes mellitus at high cardiovascular risk | Empagliflozin 10 mg or 25 mg daily | Placebo | 7020 | Median 3.1 years | Small increases in LDL-C and HDL-C, values not extracted | Reduced cardiovascular events and mortality | Multinational |
| Bauer et al. (2025) [ | Randomized, double blind, placebo controlled, parallel group, phase 4 | Type 2 diabetes mellitus with heart failure phenotype, EmDia | Empagliflozin 10 mg daily | Placebo | 144 | 1 week and 12 weeks time points | Lipidomics primarily standardizes lipids, not primary | Distinct lipidome signatures after empagliflozin at 1 week and 12 weeks | Germany |
| Emanuelsson et al. (2025) [ | Post hoc analyses of two double blind, placebo controlled trials, Empire HF and SIMPLE | Heart failure with reduced ejection fraction cohort and type 2 diabetes mellitus cohort | Empagliflozin 10 mg or 25 mg | Placebo | 190 and 90 | 12 weeks | No material changes in lipids and lipoproteins versus placebo | Supports cardioprotection independent of lipid concentration changes | Multicenter |
| Bays et al. (2017) [ | Post-hoc pooled analysis of phase 3 placebo-controlled trials | Type 2 diabetes mellitus with and without high TG and low HDL phenotype | Dapagliflozin 10 mg | Placebo | Not reported | 24 weeks | Minor increases in LDL-C and HDL-C, TG variable, values not extracted | Lipid effects broadly similar across baseline lipid phenotype groups | Multinational |
| Dixon et al. (2021) [ | Post-hoc analysis of CANA HF randomized trial | Type 2 diabetes mellitus with heart failure with reduced ejection fraction | Canagliflozin 100 mg daily | Sitagliptin 100 mg daily | 36 enrolled, 35 analyzed | 12 weeks | No significant between-group differences in LDL-C, HDL-C, TG, TC | Canagliflozin did not increase LDL-C compared with sitagliptin in this cohort | United States |
| Liu et al. (2024) [ | Prospective interventional study | Type 2 diabetes mellitus | Canagliflozin, dose not reported | Metformin | Not reported | 12 weeks | HDL-C increased, LDL-C and TG trend lower, values not extracted | ANGPTL3 reduction proposed as a mechanism linked to HDL changes | China |
| Hiruma et al. (2021) [ | Randomized, open label, blinded endpoint, parallel group, ASSET | Early stage type 2 diabetes mellitus | Empagliflozin | Sitagliptin | 44 | 12 weeks | HDL-C increased, full lipid table not extracted | Ketone bodies increased and insulin resistance markers improved | Japan |
| Burggraaf et al. (2022) [ | Randomized, double blind, placebo controlled, proof of concept | Male type 2 diabetes mellitus on intensive insulin | Dapagliflozin 10 mg | Placebo | 14 | 12 weeks | No effect on fasting or postprandial cholesterol or triglycerides | Reduced chylomicron remnants and ApoB48, increased postprandial ketones and glucagon | Netherlands |
| Wazir et al. (2022) [ | Interventional clinical study | Type 2 diabetes mellitus | Empagliflozin 10 mg versus 25 mg | Dose comparison | 59 | 12 weeks | Not extracted | Lipid profile outcomes reported, details not extracted | Pakistan |
| Jojima et al. (2021) [ | Interventional clinical study | Adults with type 2 diabetes mellitus | Empagliflozin 10 mg daily | Control not reported | 51 | 12 weeks | Not extracted | Increased campesterol, a marker of cholesterol absorption | Japan |
| Najim et al. (2025) [ | Comparative clinical study | Type 2 diabetes mellitus with diabetic nephropathy | Dapagliflozin versus empagliflozin | Active comparator | 41 | 16 weeks | Not extracted | Nephropathy-focused, lipid outcomes used only if extractable | Palestine |
| Fukada et al. (2025) [ | Clinical study in metabolic dysfunction associated with steatotic liver disease with type 2 diabetes mellitus | Metabolic dysfunction associated with steatotic liver disease with type 2 diabetes mellitus | Dapagliflozin | Comparator not reported | Not reported | Not reported | Not extracted | Effectiveness and risks in metabolic dysfunction associated with steatotic liver disease population | Japan |
| Langslet et al. (2020) [ | Post hoc analysis of EMPA REG OUTCOME dataset | Type 2 diabetes mellitus with cardiovascular risk | Empagliflozin 10 mg or 25 mg daily | Placebo | 7020 | About 3.1 years | Not a lipid change analysis | Outcomes examined in relation to achieved LDL-C strata | Multinational |
| Moura et al. (2021) [ | Post hoc subgroup analysis of DECLARE TIMI 58, conference abstract | Type 2 diabetes mellitus with metabolic syndrome | Dapagliflozin 10 mg daily | Placebo | 17160 | Variable follow-up | Not extracted | Metabolic syndrome subgroup analysis | Multinational |
| Li et al. (2025) [ | Interventional study | Overweight or obese type 2 diabetes mellitus | Dapagliflozin plus probiotics | Dapagliflozin alone | 120 | 24 weeks | Not extracted | Gut microbiota and metabolic syndrome context | China |
| Kabir et al. (2023) [ | Randomized, placebo-controlled trial | Adults with type 2 diabetes mellitus and dyslipidaemia | Dapagliflozin 10 mg daily added to existing therapy | Placebo added to existing therapy | 26 | 12 weeks | LDL-C decreased, HDL-C increased, TG decreased, TC not reported | Primary outcome was the change in lipid profile after 12 weeks; secondary outcomes included improved HbA1c, fasting plasma glucose, weight, and systolic blood pressure | Pakistan |
| Nagao et al. (2024) [ | Randomized trial, SUCRE | Early-phase type 2 diabetes mellitus | Ipragliflozin 50 mg daily | Sitagliptin 50 mg daily | 160 | 6 months | Not extracted | Atherogenic lipoprotein profile changes | Japan |
| Rau et al. (2021) [ | Randomized, placebo-controlled | Type 2 diabetes mellitus | Empagliflozin | Placebo | Not reported | 12 weeks | Not extracted | Lipoprotein subfraction changes | Germany |
| Ejiri et al. (2022) [ | Randomized, open-label, controlled | Type 2 diabetes mellitus with heart failure | Luseogliflozin 2.5 mg daily | Voglibose | 173 | 12 weeks | Not extracted | High-risk lipid profiles and inflammatory markers | Japan |
| Authors (Year) | Study Design | Population | SGLT2 Intervention | Comparator | N | Duration | Key Lipid Changes (LDL-C, HDL-C, TG, TC) | Mechanistic Findings | Country |
| Kamijo et al. (2019) [ | Multicenter prospective study | Adults with type 2 diabetes mellitus | Canagliflozin 100 mg daily | None, single arm | 22 | 12 weeks | LDL-C not reported, HDL-C increased in very large and large HDL fractions, TG not reported, TC not reported | Increased cholesterol in specific HDL fractions, weight and blood pressure reduced | Japan |
| Doğanay et al. (2023) [ | Retrospective comparative study | Newly diagnosed hypertensive type 2 diabetes mellitus | Sodium glucose cotransporter 2 inhibitor users, agents compared, including canagliflozin subgroup | Non sodium glucose cotransporter 2 inhibitor controls | 236 | Not reported | LDL-C not reported, HDL-C not reported, TG not reported, TC not reported | Pre- and post-lipid changes assessed, subgroup analyses reported | Turkey |
| Ku et al. (2021) [ | Prospective observational study | Adults with type 2 diabetes mellitus on quadruple therapy | Empagliflozin versus dapagliflozin | Head to head groups | 362 | 3 years | Not extracted | Long term effectiveness and safety, lipid benefit noted | South Korea |
| Grubić Rotkvić et al. (2023) [ | Prospective nonrandomized observational study | Type 2 diabetes mellitus, myocardial dysfunction focus | Sodium glucose cotransporter 2 inhibitor, unspecified | Comparator group, nonrandomized | 64 | 6 months | Lipid profile changed significantly, direction not stated | Metabolic parameters and diastolic function markers improved | Croatia |
| Khanna et al.(2025) [ | Prospective open label parallel group study | Uncontrolled type 2 diabetes mellitus on metformin | Dapagliflozin | Vildagliptin | 383 enrolled, 248 completed | 24 weeks | LDL-C increased, HDL-C increased, TG no significant between group difference, TC decreased | Between group pattern reported for LDL-C, HDL-C, and TC, values not extracted | India |
| Lim et al.(2022) [ | Retrospective propensity score matched cohort | Type 2 diabetes mellitus without prior cardiovascular disease or chronic kidney disease | Dapagliflozin versus empagliflozin | Matched control cohort included | 3684 | Median 43.4 months | LDL-C increased, particularly with empagliflozin, HDL-C not reported, TG not reported, TC not reported | Comparative real world outcomes, lipid signal mainly LDL-C | South Korea |
| Pahlavan et al. (2025) [ | Prospective single center clinical trial | Type 2 diabetes mellitus with nonalcoholic fatty liver disease | Empagliflozin add on to metformin | None, single arm | 80 enrolled, 74 completed | 12 weeks | LDL-C decreased, HDL-C no significant change, TG decreased, TC decreased | Improved metabolic profile and liver enzymes, lipid improvements reported | Iran |
| Cokro et al. (2025) [ | Real world comparative cohort, paired data analysis | Adults with type 2 diabetes mellitus | Dapagliflozin 10 mg daily | Empagliflozin 10 mg daily | Up to 319, variable by outcome | 12 months | LDL-C decreased in both groups. HDL-C increased with dapagliflozin and no significant change with empagliflozin. TG decreased with dapagliflozin and no significant change with empagliflozin. TC decreased with empagliflozin and no significant change with dapagliflozin | Adjusted analyses showed broadly similar lipid patterns | Indonesia |
| Gogoleva et al. (2023) [ | Prospective controlled study | Type 2 diabetes mellitus, metabolic focus | Dapagliflozin 10 mg daily | Standard management control | 60 | 6 months | LDL-C decreased, HDL-C not reported, TG decreased, TC decreased | Improvements in fat and carbohydrate metabolism reported | Russia |
| Authors (Year) | Study Design | Population | SGLT2 Intervention | Comparator | N | Duration | Key Lipid Trends (LDL-C, HDL-C, TG, TC) | Key Notes | Country |
| Storgaard et al. (2016) [ | Systematic review (evidence synthesis) | Type 2 diabetes mellitus trials | Sodium glucose cotransporter 2 inhibitors | Various comparators | Not reported | Varied | Varied | Comprehensive synthesis of benefits and harms across multiple trials | Multinational |
| Chen et al. (2021) [ | Systematic review of randomized trials (evidence synthesis) | Adults with type 2 diabetes mellitus | Sodium glucose cotransporter 2 inhibitors (multiple agents) | Placebo or active control across trials | 36 randomized trials | 24 weeks | LDL-C slight increase, HDL-C increase, TG decrease, TC no significant change | Summary of lipid shifts and metabolic effects reported across trials | Multinational |
| Shigiyama et al. (2019) [ | Trial protocol (rationale and design): ASSET | Adults with type 2 diabetes mellitus | Empagliflozin 10 mg daily | Sitagliptin 100 mg daily | Planned 44 | Planned 12 weeks | Not applicable | Protocol focused on cardiac fat, cardiac function, and metabolic measures | Japan |
| Shigiyama et al. (2018) [ | Trial protocol (rationale and design): DIVERSITY-CVR | Adults with type 2 diabetes mellitus | Dapagliflozin 10 mg daily | Sitagliptin 100 mg daily | 340 | 24 weeks | Not applicable | Protocol designed to evaluate cardiovascular risk prevention endpoints | Japan |
| Tool/Study type | Overall category | Number of records |
| RoB 2 (RCTs) | Low risk | 12 |
| RoB 2 (RCTs) | Some concerns | 11 |
| ROBINS-I (Observational) | Moderate | 7 |
| ROBINS-I (Observational) | Serious | 2 |
| Not assessed | Not assessed (protocols and evidence syntheses) | 4 |
| Study (Reference) | Study Design | Tool Used | D1 | D2 | D3 | D4 | D5 | Overall Risk |
| Kahl et al. (2020) [ | Randomized, double-blind, placebo-controlled phase 4 trial | RoB 2 | Some concerns (randomization details insufficiently reported in extractable text) | Some concerns (insufficient reporting to judge deviations from intended interventions) | Some concerns (attrition/missing outcome handling not accessible) | Low | Some concerns | Some concerns |
| Lauritsen et al. (2022) [ | Randomized, double-blinded, placebo-controlled crossover (empagliflozin vs placebo) with washout | RoB 2 | Some concerns (sequence generation/allocation concealment not fully extractable) | Low (double-blind placebo cross-over described) | Some concerns | Low | Some concerns | Some concerns |
| Fadini et al. (2017) [ | Randomized placebo-controlled trial; single-blind; computer-generated sequence; endpoint evaluation by blinded assessors | RoB 2 | Some concerns | Some concerns (single-blind → potential performance bias, although outcomes are lab-based) | Some concerns (33 randomized/31 completed stated, but limited accessible detail on missingness handling) | Low (endpoint evaluation by blinded people; objective measures) | Low (trial registration reported) | Some concerns |
| Hayashi (2017) [ | Prospective randomized open-label trial (dapagliflozin vs sitagliptin add-on); trial registered (UMIN) | RoB 2 | Some concerns (randomization method/concealment not clearly extractable from accessible text) | Some concerns (open-label → possible deviations; although lipid endpoints are objective) | Some concerns (attrition/missing data handling not clearly stated in extractable text) | Low (objective lipid outcomes; measurement bias less likely) | Low (trial registration reported) | Some concerns |
| Zinman et al. (2015) [ | Randomized, double-blind, placebo-controlled cardiovascular outcomes trial | RoB 2 | Low (computer-generated random sequence; interactive voice/web response system; stratified randomization described in article text) | Low (double-blind placebo-controlled) | Low (high completion and vital status availability reported) | Low (events/deaths prospectively adjudicated by clinical-events committees) | Low ( | Low |
| Bauer et al. (2025) [ | Randomized, double-blind, placebo-controlled, parallel-group phase IV trial (lipidomics analysis of EmDia samples; | RoB 2 | Not yet extracted | Not yet extracted | Not yet extracted | Not yet extracted | Not yet extracted | Not yet extracted |
| Emanuelsson et al. (2025) [ | Post-hoc analyses of 2 randomized, double-blinded, placebo-controlled trials (Empire HF: 190 HF patients; SIMPLE: 90 T2D patients), 1:1 to empagliflozin vs placebo for 12 weeks | RoB 2 (randomized trials) | Some concerns (randomization process details not described beyond 1:1 randomization) | Low (double-blinded, placebo-controlled) | Low (reports trials completed as planned) | Low (objective lab outcomes measured using standard methods) | Some concerns (explicitly described as exploratory/post-hoc) | Some concerns |
| Bays et al. (2017) [ | Post hoc analysis of 10 phase 3, placebo-controlled studies (dapagliflozin 10 mg vs placebo; 24 weeks) | RoB 2 (not fully applicable to pooled post-hoc analysis) | Some concerns (not assessable from the pooled report) | Some concerns | Some concerns | Low (lab lipids) | High (post-hoc/selection risk) | High |
| Dixon et al. (2021) [ | Post-hoc analysis of CANA-HF; CANA-HF described as a prospective randomized controlled study (canagliflozin vs sitagliptin); 35/36 had baseline + 12-week lipids | RoB 2 | Some concerns (randomization details not in abstract) | Some concerns (blinding/deviations not stated in the abstract) | Low (35/36 complete lipid data) | Low (objective serum lipids) | Some concerns (explicit post-hoc analysis) | Some concerns |
| Hiruma et al. (2021) [ | Prospective randomized; open-label, blinded-endpoint; randomization via computer-based dynamic allocation | RoB 2 | Low | Some concerns (open-label) | Some concerns (exclusions/analysis set details suggest possible missingness impact) | Low (blinded endpoint stated) | Some concerns (protocol/analysis plan not fully checked here) | Some concerns |
| Burggraaf et al. (2022) [ | Placebo-controlled randomized proof-of-concept; randomly and double-blindly allocated to dapagliflozin vs placebo for 12 weeks (n=14 men) | RoB 2 | Some concerns (sequence/concealment not detailed in abstract) | Low (double blind) | Some concerns (missing data handling not described in the abstract) | Low (objective lab outcomes) | Some concerns (registration/analysis plan not assessed here) | Some concerns |
| Wazir et al. (2022) [ | Randomized, open-label clinical trial; 59 adults randomized 1:1 to empagliflozin 10 mg vs 25 mg add-on; fasting lipid profile measured at baseline and 12 weeks | RoB 2 | Some concerns (method of random sequence/concealment not described in accessible text) | Some concerns (open-label stated) | Some concerns (attrition/missing handling not clearly described in accessible text) | Low (objective lab measurement) | Some concerns (no protocol/registry details seen in accessible text) | Some concerns |
| Jojima et al. (2021) [ | Randomized, active-controlled, open-label trial; 51 patients allocated 2:1 to empagliflozin 10 mg/day vs standard therapy for 12 weeks | RoB 2 | Some concerns (randomization procedure details not provided in the abstract) | Some concerns (open-label stated) | Some concerns (missing-data handling not stated in the abstract) | Low (objective sterols + lipid labs) | Some concerns (analysis plan/registration not stated in abstract) | Some concerns |
| Najim et al. (2025) [ | Interventional open-label randomized clinical trial; 41 T2DN patients “divided…randomly” into DAPA 5 mg/day vs EMPA 10 mg/day for 16 weeks; lipids measured at baseline and week 16 | RoB 2 | Some concerns (randomization method/concealment not detailed) | Some concerns (open-label stated) | Some concerns (missing-data handling not clearly stated in the accessible section) | Low (objective lab outcomes; analyzer methods described) | Some concerns (no preregistered analysis plan seen in accessible section) | Some concerns |
| Fukada et al. (2025) [ | Randomized controlled trial of dapagliflozin in MASLD with T2D (as stated in the article PDF) | RoB 2 | Some concerns (randomization process details not clearly extractable from accessible text segments) | Some concerns (blinding/deviation-control not clearly described in accessible text segments) | Some concerns (missing-data handling not clearly described in accessible text segments) | Low (outcomes largely objective labs/imaging-based in RCT context, per trial report) | Some concerns (analysis plan/selection reporting not clearly verifiable from accessible text segments) | Some concerns |
| Langslet et al. (2020) [ | Post-hoc analysis of EMPA-REG OUTCOME: participants randomized to empagliflozin 10/25 or placebo; LDL-C subgroup cutoffs “established post-hoc”; modified ITT used; outcomes adjudicated by Clinical Events Committees | RoB 2 | Some concerns (subgroup comparisons not stratified by LDL-C; baseline subgroup imbalances possible) | Some concerns (deviations control/blinding not stated in accessible text) | Some concerns (baseline LDL-C missing for some participants; subgroup data availability issue) | Low (CV outcomes prospectively adjudicated) | High (explicit post-hoc subgroup cutoffs and post-hoc analysis) | High |
| Khanna (2025) [ | Prospective parallel-group open-label study; randomized (computer-generated block randomization) dapagliflozin vs vildagliptin; per-protocol analysis; 383 randomized, 248 completed | RoB 2 | Some concerns | High | High | Low | Some concerns | High. |
| Moura et al. (2021) [ | Sub-analysis of a randomized, double-blind, placebo-controlled trial | RoB 2 | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Li et al. (2025) [ | Prospective, single-center, randomized, open-label parallel trial | RoB 2 | Low | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| Kabir et al. (2023) [ | Placebo-controlled intervention study; group assignment by convenience sampling (not truly randomized) | RoB 2 | High | Some concerns | Some concerns | Low | Some concerns | High |
| Nagao et al. (2024) [ | Multicenter, randomized, open-label, active-controlled trial | RoB 2 | Low | Some concerns | Some concerns | Low | Some concerns | Some concerns |
| Rau et al. (2021) [ | Randomized, double-blind, placebo-controlled study (lipoprotein subfractions) | RoB 2 | Low | Low | Some concerns | Low | Some concerns | Some concerns |
| Ejiri et al. (2022) [ | Randomized controlled trial (UMIN-CTR registered); prespecified sub-analysis | RoB 2 | Low | Some concerns | Some concerns | Low | Low | Some concerns |
| Study (Reference) | Study Design | Tool Used | D1 | D2 | D3 | D4 | D5 | Overall Risk |
| Kamijo et al. (2019) [ | Multicenter prospective single-arm pre–post study (canagliflozin 100 mg for 12 weeks; n=22). | ROBINS-I | Serious | No info | No info | No info | No info | Serious (non-comparative pre–post → high confounding risk) |
| Doğanay et al. (2023) [ | Single-center retrospective study; SGLT2i vs propensity-matched control; fasting samples compared at baseline and week 12; excluded “missing clinical data”. | ROBINS-I | Moderate | Moderate | Moderate | Low | No info | Moderate |
| Ku et al. (2021) [ | 3-year open-label prospective observational study; empagliflozin vs dapagliflozin add-on (n=362); trial number listed ( | ROBINS-I | Serious | Moderate | No info | No info | Moderate | Serious |
| Grubić Rotkvić et al. (2023) [ | Prospective observational study; patients divided into planned SGLT2i vs DPP-4 inhibitor groups; baseline and 6-month follow-up (n=64). | ROBINS-I | Serious | Moderate | No info | No info | No info | Serious |
| Lim et al. (2022) [ | Retrospective study comparing dapagliflozin vs empagliflozin using propensity score matching. | ROBINS-I | Moderate | Moderate | No info | No info | No info | Moderate |
| Pahlavan et al. (2025) [ | 12-week prospective single-center clinical trial; empagliflozin added to metformin (80 enrolled; 74 completed); trial registration reported (IRCT trial/73164). | ROBINS-I | Serious | Moderate | Moderate | Low | Low | Serious |
| Cokro et al. (2025) [ | Real-world comparative study described as a retrospective cohort; reports handling missing data with imputation in methods. | ROBINS-I | Moderate | Moderate | Moderate | No info | No info | Moderate |
| Gogoleva et al. (2023) [ | “Open cohort controlled prospective study”; 60 patients; dapagliflozin 10 mg added to metformin; 6-month follow-up with lipid panel in dynamics. | ROBINS-I | Serious | Moderate | No info | Low | No info | Serious |
| Liu et al. (2024) [ | Single-center, open-label, nonrandomized, prospective (metformin vs canagliflozin; 12 weeks); baseline differences reported. | ROBINS-I | Serious/Critical (confounding likely: nonrandomized; baseline differences) | Serious | Low (interventions clearly defined) | Serious (open-label; treatment decisions not randomized) | Some concerns (missing data handling not clear in accessible excerpt) | Serious |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Diabetes, Cardiovascular Risks, and Lipoproteins · Lipoproteins and Cardiovascular Health
Introduction and background
Type 2 diabetes mellitus is a global epidemic affecting hundreds of millions of adults worldwide and is projected to rise substantially in the coming decades [1]. Beyond chronic hyperglycemia, this condition is associated with a high burden of cardiovascular and renal complications, highlighting the importance of comprehensive risk factor management [2]. A characteristic pattern of diabetic dyslipidemia includes elevated triglyceride levels, reduced high-density lipoprotein cholesterol (HDL-C) levels, and a predominance of small dense low-density lipoprotein (LDL) particles, which accelerates atherosclerosis and contributes to residual cardiovascular risk [3].
Sodium glucose cotransporter 2 (SGLT2) inhibitors, including empagliflozin, dapagliflozin, and canagliflozin, are oral therapies for type 2 diabetes mellitus that lower blood glucose by inhibiting renal tubular glucose reabsorption [4], and large cardiovascular outcome trials, including the CANVAS Program and DECLARE TIMI 58, demonstrated reductions in hospitalization for heart failure and favorable renal outcomes; CANVAS also reduced major adverse cardiovascular events, whereas DECLARE TIMI 58 met the noninferiority for major adverse cardiovascular events [5,6]. Collectively, these data contributed to positioning SGLT2 inhibitors as cardiometabolic therapies with benefits extending beyond glycemic control [2,4].
Given that many candidates for SGLT2 inhibitors also meet indications for statin therapy and other lipid-modifying strategies, and that background statin and other lipid-modifying therapies may mask or modify observed lipid changes, clarifying the drugs' effect on atherogenic lipid profiles is of direct clinical importance to support interpretation of trial lipid results [3,7]. Systematic reviews and meta-analyses of randomized trials have evaluated overall benefits and harms of SGLT2 inhibitors and reported associated changes in cardiometabolic parameters [8]. More lipid focused meta analyses have reported modest shifts in standard lipid measures, including low-density lipoprotein cholesterol (LDL-C) and HDL-C, following SGLT2 inhibitor initiation, but they variably capture advanced lipid markers, including apolipoprotein B (apoB), remnant cholesterol, lipoprotein subfractions, HDL function, and lipidomic or qualitative remodeling signals, raising questions about interpretation in already high-risk populations [9]. Mechanistic reviews propose several pathways that could underlie these lipid changes, including altered substrate utilization and downstream effects on hepatic lipoprotein production and clearance [10].
Given the central role of dyslipidemia in driving cardiovascular risk in type 2 diabetes mellitus and the mixed directionality of reported lipid changes, and the variable reporting of advanced lipid markers across studies, a focused synthesis is warranted [3,7]. This systematic review aimed to summarize the effects of SGLT2 inhibitors on LDL-C, HDL-C, triglycerides, and total cholesterol and to describe reported advanced lipid markers when available, in adults with type 2 diabetes mellitus.
Objectives
We conducted a systematic review to evaluate the effects of SGLT2 inhibitors on standard serum lipid outcomes, including LDL-C, HDL-C, triglycerides, and total cholesterol, in adults with type 2 diabetes mellitus. Secondary objectives were to compare lipid effects across individual SGLT2 agents and to summarize advanced lipid markers and mechanistic explanations proposed in the literature [10,11]. We hypothesized that SGLT2 inhibitors have neutral to modest effects on standard lipid parameters and that these changes would not negate established cardiovascular and renal benefits reported in major outcome trials [5,6,8], with additional supportive evidence from experimental studies on diabetes associated renal and hepatic fibrosis [11].
Review
Methods
This systematic review, reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [12], evaluated the effects of sodium glucose cotransporter 2 inhibitors on lipid metabolism in adults with type 2 diabetes mellitus using the PICOS framework.
Protocol and Registration
The protocol was developed using the PICOS framework and prospectively registered in PROSPERO (ID 1237510) on 21 November 2025, titled "The Effects of SGLT2 Inhibitors on Lipid Metabolism: A Systematic Review and Meta-Analysis." The protocol specified eligibility criteria, the search strategy, outcomes, and the planned approach to evidence synthesis. No formal sample size or power calculation was performed because the number of participants was determined by the available eligible studies.
Eligibility Criteria
The population of interest was adults aged 18 years or older with type 2 diabetes mellitus, with or without comorbid cardiovascular disease, heart failure, nephropathy, obesity, metabolic syndrome, or nonalcoholic fatty liver disease, provided that lipid outcomes were reported. Interventions included any sodium glucose cotransporter 2 inhibitor, for example, empagliflozin, dapagliflozin, canagliflozin, or ertugliflozin, at any approved dose. Comparators were placebo, usual care, or active non-sodium glucose cotransporter 2 glucose-lowering therapies, such as dipeptidyl peptidase 4 inhibitors, glucagon-like peptide 1 receptor agonists, or insulin-based regimens.
The primary outcomes were changes in conventional lipid parameters, including LDL-C, HDL-C, triglycerides, and total cholesterol, reported as absolute change, percentage change from baseline, or between-group difference. Secondary outcomes included changes in body weight and anthropometric indices, glycaemic markers including fasting plasma glucose and HbA1c, indices of insulin resistance, and mechanistic or lipidomic measures, for example, low-density lipoprotein subfractions, high-density lipoprotein subtypes, and angiopoietin-like protein 3, where available.
Eligible designs were randomized controlled trials and prospective or retrospective observational cohorts that provided extractable quantitative lipid data before and after sodium glucose cotransporter 2 inhibitor therapy. Case reports, case series, narrative reviews, editorials, nonhuman studies, and reports without extractable lipid outcomes were excluded. Only full-text articles in English were included, with no date restrictions. Eligibility criteria are summarized using the PICOS framework (see Table 1).
Information Sources and Search Strategy
We searched MEDLINE via PubMed, Embase, Web of Science, and the Cochrane Library from database inception to August 2025. The search combined controlled vocabulary and free text terms relating to SGLT2 inhibition, type 2 diabetes mellitus, and lipid outcomes (e.g., empagliflozin, cholesterol, triglycerides). Titles, abstracts, and keywords were searched, and reference lists of key randomized trials and relevant systematic reviews were screened manually to identify additional studies. No language limits were applied during the search, but eligibility was restricted to studies with full text available in English.
Conference abstracts from major diabetes and cardiology meetings from 2023 to 2025 were also screened. Where possible, corresponding full-text publications were retrieved. Abstracts without sufficient quantitative data were used only for contextualisation and were not included in the primary synthesis. All records were imported into reference management software, and duplicates were removed before screening. The full search strategy is presented in Table 2.
Study Selection
Study selection occurred in two stages. First, two reviewers independently screened titles and abstracts and excluded clearly irrelevant reports, including studies of nondiabetic populations, non-sodium glucose cotransporter 2 interventions, articles without lipid outcomes, and non-original research. Second, full-text articles of potentially eligible records were assessed against the predefined inclusion and exclusion criteria. Disagreements were resolved by discussion, with a third reviewer consulted when needed.
Data Extraction and Management
Two reviewers independently extracted data using a piloted, standardised form. For each study, we recorded author and year, country and clinical setting, study design, sample size, and baseline characteristics, including age, sex, duration of type 2 diabetes mellitus, and presence of cardiovascular disease, heart failure, nephropathy, or nonalcoholic fatty liver disease. We also extracted details of sodium glucose cotransporter 2 inhibitor type and dose, comparator regimen including placebo, usual care, or active non-sodium glucose cotransporter 2 therapy, and duration of follow-up.
For lipid outcomes, we extracted baseline and follow-up values for total cholesterol, LDL-C, HDL-C, and triglycerides, along with reported mean absolute changes, percentage changes, or between-group differences, and corresponding measures of variability, including standard deviation, standard error, or confidence interval, when available. All values were converted to milligrams per decilitre using standard factors. For total cholesterol, LDL-C, and HDL-C, mg per dL equals mmol per L multiplied by 38.67. For triglycerides, mg per dL equals mmol per L multiplied by 88.57.
Where reported, we also collected data on lipid subfractions, postprandial lipid responses, and mechanistic biomarkers such as angiopoietin-like protein 3 and ApoB48. When outcomes were available only as figures, we estimated numerical values from graphs where feasible. If key data were unclear or missing, we checked the main text and supplementary files and, where necessary, attempted to contact study authors.
Studies with insufficient data for a particular lipid parameter were included in the qualitative synthesis but omitted from outcome-specific analyses for that parameter. No statistical imputation of missing lipid values or measures of variability was performed.
Risk of Bias Assessment
Risk of bias was assessed using design-appropriate tools. Randomized and interventional studies were evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool (including the RoB 2 variant for crossover trials when applicable) [13]. Judgments were made across five domains: D1 randomization process, D2 deviations from intended interventions, D3 missing outcome data, D4 measurement of the outcome, and D5 selection of the reported result. Each domain was rated as low risk, some concerns, or high risk, and an overall RoB 2 judgment was derived from the domain-level ratings.
Nonrandomized comparative studies of interventions were assessed using the ROBINS I tool [14], which evaluates bias due to confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and selective reporting. Overall, ROBINS I judgments were categorized as low, moderate, serious, or critical risk of bias.
For uncontrolled single-arm pre-post studies without a concurrent comparator, we used an adapted domain-based assessment informed by ROBINS I signaling domains [14], with particular emphasis on confounding and time-varying cointerventions, and findings were interpreted cautiously because ROBINS I is primarily intended for nonrandomized comparative studies. Systematic reviews and meta-analyses were appraised separately using AMSTAR 2, and protocol and rationale papers were listed for transparency but were not eligible for outcome-level risk of bias assessment. Assessments were conducted independently by two reviewers, with disagreements resolved by consensus or by consultation with a third reviewer.
Data Synthesis
We synthesized findings qualitatively due to variability in study designs, comparators, follow-up durations, and outcome reporting across included studies. Where studies reported comparable outcomes, we summarized the direction and consistency of changes in total cholesterol, LDL-C, HDL-C, and triglycerides. We also summarized mechanistic and lipidomic outcomes narratively when reported.
Results
Study Selection and Characteristics
The systematic database search identified 812 records. After removal of duplicates (n = 132), 680 records were screened by title and abstract, and 540 were excluded. Full-text review was conducted for 140 reports, of which 104 were excluded due to ineligible population, intervention, or outcomes (n = 79), or because reports were non-original or had insufficient data (n = 25). Ultimately, 32 primary studies met the inclusion criteria and were included in the qualitative synthesis. Four additional records were evidence syntheses or protocol and design papers that were retained for context and transparency, but were not treated as included studies for outcome level synthesis (see Figure 1).
PRISMA flow diagram of study identification, screening, eligibility assessment, and inclusionRecords were identified through database searching; duplicates were removed before screening. Titles and abstracts were screened, and full texts of potentially eligible reports were assessed against predefined inclusion and exclusion criteria. Studies meeting eligibility criteria were included in the qualitative synthesis.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Records were identified through database searching; duplicates were removed before screening. Titles and abstracts were screened, and full texts of potentially eligible reports were assessed against predefined inclusion and exclusion criteria. Studies meeting eligibility criteria were included in the qualitative synthesis.
Of the 32 included primary studies, 23 were interventional studies [15-37], and nine were observational real-world nonrandomized studies [38-46]. Secondary evidence and protocol or design records were listed separately for transparency and context and were not included in outcome synthesis [8,47-49]. Collectively, these investigations enrolled more than 30,000 adults with type 2 diabetes mellitus. Follow-up ranged from short mechanistic investigations (~4 weeks) [16] to longer follow-up of approximately three years [19,40].
The most frequently evaluated SGLT2 inhibitors were empagliflozin, dapagliflozin, and canagliflozin, whereas ipragliflozin and luseogliflozin were examined less often. Comparators included placebo, standard of care, and active glucose-lowering therapies, most commonly DPP-4 inhibitors (see Table 3).
Key Lipid Profile Findings
Triglycerides and HDL-C, modest improvements with variable consistency: Across interventional studies, SGLT2 inhibitors showed small, heterogeneous effects on standard fasting lipids. In pooled dapagliflozin analyses, lipid changes were small and appeared to vary by baseline phenotype, and a post-hoc comparison found no significant between-group differences in conventional serum lipids for canagliflozin versus sitagliptin. Mechanistic and lipid-focused trials described qualitative lipoprotein shifts, including reductions in small dense LDL-C and changes in HDL subfractions, and lipidomic profiling suggested broader remodeling not fully captured by routine fasting lipid panels. Evidence syntheses likewise describe modest HDL-C increases and triglyceride reductions, with variability across trials [18,20,22,23,47].
These patterns were broadly echoed in nonrandomized settings, but interpretation is limited by confounding and changes in background therapy over follow-up (see Table 4).
LDL-C, heterogeneous patterns with mixed qualitative signals: The impact of sodium glucose cotransporter 2 inhibitors on LDL-C was heterogeneous across study designs and clinical contexts. In randomized and interventional studies, qualitative lipoprotein effects were not uniform. Some mechanistic evidence suggests reductions in small dense LDL-C and potentially favorable shifts in HDL subfractions [18]. In longer term outcome trials and related analyses, LDL-C generally remained unchanged or increased slightly, as reported in EMPA REG OUTCOME and associated analyses, and in DECLARE-related reporting within included sources [19,31,32]. Other studies reported no clear mean change in standard LDL measures [21] or increases in LDL-related markers without clear particle size improvement [36].
Across broader pooled evidence, meta-analyses have reported small increases in LDL-C alongside changes in HDL-C, with heterogeneity by dose, ethnicity, and drug type [8,9]. In real-world and pragmatic settings, LDL-C trajectories were variable and may reflect differences in baseline risk, weight change, glycaemic control, and background lipid therapy [43,45]. Comparative data also suggest that LDL-C direction can depend on the active comparator and therapeutic context; for instance, LDL-C increased with dapagliflozin relative to vildagliptin in an open-label comparative study [42].
Secondary findings and mechanistic insights: Several studies reported mechanistic signals that may underlie lipid modulation, and these findings are summarized here separately from the clinical lipid outcome synthesis. Changes in tissue-level lipid handling and transport were described in adipose-focused work [16]. Biomarker signals potentially relevant to lipid metabolism were reported, including angiopoietin-like protein 3 findings alongside HDL-related changes [24]. Altered cholesterol handling was suggested by changes in absorption markers [28]. In metabolic dysfunction-associated steatotic liver disease populations, dapagliflozin was associated with improvements in related parameters that may be relevant to lipid handling [30]. Clinical lipid outcomes are interpreted in the corresponding Results subsections, while this paragraph is limited to mechanistic observations. Secondary evidence, protocol, and design records are listed in Table 5.
Synthesis of Lipid Findings
Favorable and more consistent changes - triglycerides and HDL-C: Across study designs, the most consistent signals were modest triglyceride reductions and modest HDL-C increases, although effects were heterogeneous. Evidence syntheses of randomized trials generally describe small, directionally favorable triglyceride changes with variability by agent, dose, and population, and similarly report modest HDL-C increases. Large outcome trials and pooled clinical trial analyses typically showed minor absolute lipid changes, but the triglyceride direction was commonly favorable [19,22]. In mechanistic and lipoprotein subfraction studies, HDL-related changes included HDL2 increases and increases in large HDL fractions [18,38].
Mechanistic evidence supports a metabolic shift with SGLT2 inhibition that may influence lipid handling through increased fatty acid utilization and broader metabolic adaptations, and lipidomic studies suggest remodeling of circulating lipid species not fully captured by standard fasting lipid measurements [4,10,20]. In observational cohorts, lipid changes should be interpreted cautiously because trajectories may be influenced by concurrent weight change, glycaemic improvement, and background lipid therapy over follow-up [45].
LDL-C findings: discrepancies by study design and inconsistent qualitative effects: Effects on LDL-C were heterogeneous and context dependent. Evidence syntheses of randomized trials generally describe small mean LDL-C increases or neutrality, with variability across agents and populations. Large long-term outcome trials commonly showed no significant LDL-C change or slight increases, consistent with broader randomized trial evidence [5,6,19].
Evidence for a consistently improved LDL phenotype was mixed. Some mechanistic work demonstrated reductions in small dense LDL-C [18]. However, detailed subfraction studies have reported discordant findings, including LDL-related increases without clear particle size improvement, or no meaningful lipid or lipoprotein concentration differences versus placebo [21,36].
Implications and mechanistic insights: Because diabetic dyslipidaemia reflects not only LDL-C concentration but also the triglyceride and HDL axis and lipoprotein quality, the overall pattern of modest triglyceride reductions, modest HDL-C increases, and variable LDL-C suggests that SGLT2 inhibitors may improve selected components of the atherogenic dyslipidaemia profile even when LDL-C is unchanged or slightly increased [3,8,9]. Qualitative lipid remodeling is inconsistent: favorable changes, including reductions in small dense LDL-C and increases in HDL2, and measures of HDL function in randomized designs, have been reported in mechanistic settings, whereas other studies report minimal change or no improvement in LDL particle size [17,18,21,36].
Mechanistic studies also suggest effects beyond standard lipid panels, including possible regulation of HDL metabolism via angiopoietin-like protein-3-related pathways, metabolic improvements in MASLD populations treated with dapagliflozin, and tissue-level changes in lipid handling, such as altered adipose lipid transport [16,24,30].
Risk of Bias and Overall Quality
A summary of risk-of-bias categories across the included primary records is presented in Table 6.
Risk of bias in randomized and interventional studies is summarized in Table 7.
Risk of bias in observational and nonrandomized studies is summarized in Table 8.
Methodological quality of the included systematic reviews/meta-analyses was appraised using AMSTAR 2 and is summarized in the Appendix. Rationale/design protocol papers were listed for transparency and are presented in the Appendix. Outcome-level risk of bias not applicable.
Discussion
Liver-Adipose Pathways
Kahl et al. [15] show that empagliflozin reduces liver fat in a randomized, placebo-controlled trial. This matters because liver fat is closely linked to atherogenic dyslipidemia, and improving liver fat and metabolism can affect how the body makes and clears lipoproteins. Lauritsen et al. [16] also add that SGLT2 inhibitors can change how lipids move in fat tissue, suggesting that shifts in tissue lipid handling can influence blood lipids, but not always in a predictable way for LDL-C or triglycerides in every group.
“HDL Quantity” Versus “HDL Quality” and Subfraction Remodeling
One reason for mixed results in the literature is that some studies look at lipid concentrations (HDL-C, LDL-C, TG), while others focus on function or subfractions. Fadini et al. [17] address this by studying HDL particle features and cholesterol efflux with dapagliflozin, showing that changes in HDL-C do not always mean better HDL function. Hayashi et al. [18] find that dapagliflozin reduces small dense LDL-C and raises HDL2-C compared to sitagliptin, suggesting SGLT2 inhibitors may lead to a less atherogenic lipoprotein profile, even if standard lipid results seem minor. Overall, these studies suggest that benefits are clearer when looking at particle composition rather than just traditional lipid levels, but the results depend on which aspect of lipids is measured.
Outcome-trial context - benefits can be dissociated from lipid panel direction: Zinman et al. [19] gave strong clinical evidence that empagliflozin improves heart outcomes and survival, even though changes in lipid levels are small. This shows that changes in lipid panels are secondary markers, not the main reason for the benefits. Thus, small increases in LDL-C in some studies should not be seen as harmful if the overall outcomes are positive.
Deep phenotyping: lipidomics and “mixed-direction” remodeling: Bauer et al. [20] went beyond standard lipid panels and showed that empagliflozin changes the overall lipid profile. Lipidomics can detect changes in many types of lipids at once, some good, some possibly not, helping explain why regular lipid panels can look neutral or even conflicting. This suggests SGLT2 inhibitors affect lipids in complex ways, not always in a single positive direction.
Heart failure and high-risk contexts, neutral averages despite metabolic shifts: Emanuelsson et al. [21] find that in people with type 2 diabetes and heart failure, changes in blood lipids are small after adjusting for other factors, even though metabolism improves. This is different from studies showing subfraction improvements and highlights how patient factors, treatments, and other conditions can affect lipid results.
Phenotype stratification and comparator dependence in conventional lipid endpoints: Bays et al. [22] show that dapagliflozin's effects on lipids are small and depend on the patient's starting triglyceride and HDL levels. In a complex heart failure group, Dixon et al. [23] found no major differences in standard lipid measures between canagliflozin and sitagliptin, showing that the choice of comparison drug and other health issues can hide expected changes. Liu et al. [24] connect canagliflozin's lipid effects to ANGPTL3, suggesting a possible reason why triglyceride-rich lipoproteins change in some groups but not others. Hiruma et al. [25] focus on heart fat and metabolism, supporting the idea that metabolic changes can happen even if lipid panels show only small shifts.
Postprandial biology - what fasting lipids can miss: Burggraaf et al. [26] showed that even if fasting or post-meal cholesterol and triglycerides do not change much, remnant markers such as apoB48 can improve, suggesting better atherogenic pathways. In contrast, Wazir et al. [27] found little change in standard lipid measures with empagliflozin in practice, which could be due to small study size, short follow-up, or a real lack of effect.
Reconciling LDL variability - absorption markers and agent-specific patterns: Jojima et al. [28] suggest that LDL-C may rise in some settings alongside higher campesterol, which may reflect increased intestinal cholesterol absorption rather than direct proof of causation. This pattern is consistent with later studies in which LDL-C increases were observed as metabolic status improves, indicating that changes in absorption markers can accompany LDL-C changes. In diabetic kidney disease, Najimi et al. [29] reported differing lipid changes with dapagliflozin versus empagliflozin, suggesting that agent-specific effects and disease context may influence results, although attribution remains challenging because of study design and overlapping treatments.
Liver disease phenotypes and trade-offs: Fukada et al. [30] looked at dapagliflozin in metabolic liver disease and found that it works, but also point out possible risks, such as changes in body composition. This means lipid improvements should be considered along with overall metabolic safety. Langslet et al. [31] showed that empagliflozin's heart benefits are steady across different LDL-C levels, so small LDL-C changes do not seem to affect outcomes. Moura et al. [32] also placed lipid results in the wider context of metabolic syndrome, suggesting that lipid changes are just one part of broader body changes over time.
Longer follow-up and co-interventions - attribution becomes harder: Li et al. [33] pointed out that using other treatments such as probiotics with dapagliflozin makes it hard to know if lipid changes are due to SGLT2 inhibitors alone. Kabir et al. [34] saw clearer improvements in standard lipids with dapagliflozin, but these results should be viewed carefully, since big effects in one study can reflect differences in starting treatments, co-interventions, and longer follow-up where therapies may overlap, as well as natural changes over time or other unknown factors.
Atherogenic profiling and the strongest internal context-dependent signal: Nagao et al. [35] demonstrated that atherogenic lipoprotein profiles shift differently depending on the comparator, reinforcing the notion that treatment effects are often relative to the comparator's biology. One of the most directly contrasting findings emerges in Rau et al. [36], where empagliflozin increased LDL-C and apoB without clear improvement in LDL particle size, standing in tension with the subfraction improvements reported earlier by Hayashi et al. [18]. Rather than a contradiction, these findings support a comparator-sensitive and population-specific signal, and they underscore a practical conclusion that qualitative lipoprotein remodeling is not guaranteed. Even when outcome benefits appear preserved, metabolic nuance can remain, and in some contexts, LDL particle burden, including apoB-related burden, may rise as clinical benefits persist.
Heart failure again - neutral lipid signals in controlled comparisons: Ejiri et al. [37] found that, in patients with type 2 diabetes and heart failure, luseogliflozin did not clearly improve certain high-risk lipid profiles compared with voglibose, consistent with the trend that heart failure patients may have weaker or less pronounced lipid changes. Kamijo et al. [38] reported that canagliflozin increases large HDL fractions, suggesting that subfraction changes can occur even when standard lipid results are mixed.
Real-world and longer-term cohorts - direction depends on setting and adjustment: Doğanay et al. [39] saw better lipid results in people with high blood pressure and type 2 diabetes using SGLT2 inhibitors, but because the study looks back at records, other treatment changes could affect the results. Ku et al. [40] compared empagliflozin and dapagliflozin over three years and saw positive lipid trends, but changing medications and how well patients stick to treatment make it hard to be sure of the cause. Grubić Rotkvić et al. [41] added more detail about the heart and metabolism, but since their study is not randomized, it is still hard to draw firm conclusions.
Comparator effects made explicit in head-to-head glucose-lowering trials: Khanna et al. [42] showed that dapagliflozin versus vildagliptin yields different lipid trajectories, with findings that can make the SGLT2 arm appear better (e.g., HDL-C) or worse (e.g., LDL-C) depending on which endpoint is prioritized, highlighting comparator-driven interpretation. Lim et al. [43] reinforced that, in longer-term real-world follow-up, LDL-C can trend higher, particularly with empagliflozin, again consistent with earlier absorption-marker hypotheses, and emphasize that LDL direction may change with time horizon and setting.
NAFLD/MAFLD cohorts and real-world paired analyses: Pahlavan et al. [44] reported improvements in metabolic profile and liver function tests in MAFLD populations treated with empagliflozin, supporting the hypothesis that a hepatic phenotype can favor more consistent beneficial lipid effects. Cokro et al. [45] provided paired real-world comparative data showing broad cardiometabolic improvements with both dapagliflozin and empagliflozin while illustrating that apparent between-drug differences may attenuate after adjustment, an important methodological reminder. Gogoleva et al. [46] similarly reported favorable lipid and metabolic shifts in obese patients with type 2 diabetes, consistent with a model in which changes in body composition and adipose biology contribute meaningfully to lipid outcomes.
Chen et al. [47] helped explain conflicting study results by showing that, overall, there are usually small drops in triglycerides and rises in HDL, while LDL changes are small and can differ between studies. Shigiyama et al. [48,49] pointed out that some papers included are just study designs, not results, so it is important not to count them as outcome data when looking at lipid effects.
Summary
Overall, the studies show that SGLT2 inhibitors most often lower triglycerides a bit and raise HDL, sometimes with changes in lipoprotein subfractions or remnant markers. However, LDL-C results are mixed and depend on patient type, comparison drug, follow-up time, other lipid treatments, and how lipids are measured. This means SGLT2 inhibitors should mainly be seen as treatments for the heart, the kidney, and metabolism, with lipid changes as secondary effects to watch, especially if apoB or LDL-C goes up, rather than as the main reason for their benefit.
Conclusions
SGLT2 inhibitors have a largely neutral to mildly favorable lipid profile in type 2 diabetes mellitus. LDL-C and total cholesterol are generally unchanged, HDL-C increases modestly, and triglycerides tend to decrease, particularly in atherogenic dyslipidaemia. Overall, these findings support SGLT2 inhibitors as cardiometabolic therapies without a consistent adverse lipid penalty.
Future studies should prioritize longer follow-up randomized trials and standardized advanced lipid reporting, with apoB as the most clinically actionable marker of atherogenic particle burden, alongside remnant cholesterol and HDL functional measures. Head-to-head and real-world studies are also needed to clarify agent-specific effects and optimize combination strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045 Diabetes Res Clin Pract Sun H Saeedi P Karuranga S 10911918320223487997710.1016/j.diabres.2021.109119 PMC 11057359 · doi ↗ · pubmed ↗
- 2SGLT 2 inhibitors - the new standard of care for cardiovascular, renal and metabolic protection in type 2 diabetes: a narrative review Diabetes Ther Seidu S Alabraba V Davies S 109911241520243857839710.1007/s 13300-024-01550-5PMC 11043288 · doi ↗ · pubmed ↗
- 3Diabetic dyslipidemia: causes and consequences J Clin Endocrinol Metab Goldberg IJ 9659718620011123847010.1210/jcem.86.3.7304 · doi ↗ · pubmed ↗
- 4SGLT 2 inhibition in diabetes mellitus: rationale and clinical prospects Nat Rev Endocrinol Ferrannini E Solini A 495502820122231084910.1038/nrendo.2011.243 · doi ↗ · pubmed ↗
- 5Canagliflozin and cardiovascular and renal events in type 2 diabetes N Engl J Med Neal B Perkovic V Mahaffey KW 64465737720172916623210.1056/NEJ Mc 1712572 · doi ↗ · pubmed ↗
- 6Dapagliflozin and cardiovascular outcomes in type 2 diabetes N Engl J Med Wiviott SD Raz I Bonaca MP 34735738020193041560210.1056/NEJ Moa 1812389 · doi ↗ · pubmed ↗
- 7Management of dyslipidemia in diabetes Cardiol Rev Solano MP Goldberg RB 1251351420061662802110.1097/01.crd.0000188034.76283.5e · doi ↗ · pubmed ↗
- 8Benefits and harms of sodium-glucose co-transporter 2 inhibitors in patients with type 2 diabetes: a systematic review and meta-analysis P Lo S One Storgaard H Gluud LL Bennett C Grøndahl MF Christensen MB Knop FK Vilsbøll T 011201610.1371/journal.pone.0166125 PMC 510600027835680 · doi ↗ · pubmed ↗