Isolated Oculomotor Nerve Palsy in a Young Adult: An Unexpected Diagnosis of HIV
Soukaina Rachidi, Imane Abourachida, Mohamed Chraa, Nissrine Louhab

TL;DR
A young man with an isolated oculomotor nerve palsy was found to have undiagnosed early-stage HIV, showing that this neurological symptom can be an early sign of HIV.
Contribution
This case report identifies isolated oculomotor nerve palsy as a rare early neurological manifestation of HIV in a young adult.
Findings
Isolated oculomotor nerve palsy with pupillary involvement was found in a 31-year-old man with undiagnosed HIV.
Antiretroviral therapy led to complete neurological recovery within three months.
CSF analysis showed an inflammatory profile, and no compressive or vascular causes were identified.
Abstract
Neurological manifestations of human immunodeficiency virus (HIV) infection are diverse and may occasionally present in the initial manifestation of the disease. Isolated cranial nerve palsies are uncommon and can pose a diagnostic challenge, particularly in young adults without known immunodeficiency. We report the case of a 31-year-old man who presented with headache, left eyelid ptosis, and binocular diplopia. Examination revealed an isolated left oculomotor nerve palsy with pupillary involvement. Neuroimaging excluded compressive and vascular causes, and cerebrospinal fluid (CSF) analysis demonstrated an inflammatory profile. An extensive diagnostic workup was otherwise negative, and further evaluation revealed previously undiagnosed early-stage HIV infection. Antiretroviral therapy was initiated, leading to complete neurological recovery at three-month follow-up. This case…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
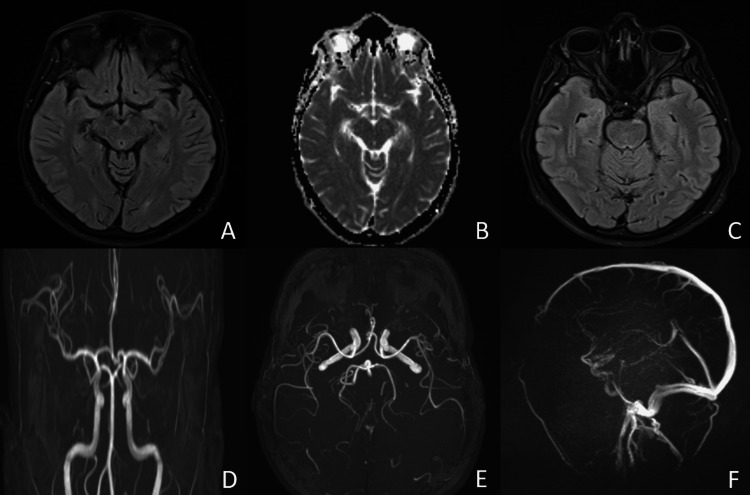 Figure 1
Figure 1| Parameters | Patient values | Reference ranges |
| CSF white blood cells (cells/mm³) | 356 | 0–5 |
| CSF mononuclear cells (%) | 98 | 60–100 |
| CSF neutrophils (%) | 2 | 0–6 |
| CSF protein (g/L) | 1.31 | 0.15–0.45 |
| CSF glucose (g/L) | 0.50 | 0.45–0.80 |
| HIV-1 plasma viral load (copies/mL) | 54,300 | <40 |
| CD4 T lymphocyte count (cells/mm³) | 396 | 500–1,500 |
| C-reactive protein (mg/L) | <1 | 0–5 |
| Serum creatinine (mg/L) | 9.98 | 6–13 |
| Serum urea (g/L) | 0.25 | 0.15–0.45 |
| Serum glucose (g/L) | 0.83 | 0.70–1.10 |
| ALT (U/L) | 17 | 7–40 |
| AST (U/L) | 23 | 10–40 |
| Total cholesterol (g/L) | 1.54 | 1.20–2.00 |
| Triglycerides (g/L) | 0.78 | <1.50 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Nerve Paralysis Treatment and Research · Cytomegalovirus and herpesvirus research · Bacterial Infections and Vaccines
Introduction
Human immunodeficiency virus (HIV) infection is associated with a wide spectrum of neurological manifestations involving both the central and peripheral nervous systems. These complications may occur at any stage of the disease and, in some cases, precede the diagnosis of HIV infection, posing a diagnostic challenge for clinicians [1,2]. Neurological involvement can result from direct viral effects, immune-mediated mechanisms, or secondary infections, and its presentation is often heterogeneous [3].
Cranial nerve palsies represent an uncommon neurological manifestation of HIV infection and may occur in isolation or in association with other neurological signs [4]. Their clinical presentation can mimic more frequent etiologies such as vascular, compressive, or inflammatory conditions, often prompting extensive diagnostic evaluation [5]. Among cranial neuropathies, involvement of the oculomotor nerve is less frequently reported and may raise concern for life-threatening causes, including aneurysmal compression [6].
Isolated oculomotor nerve palsy itself represents a relatively frequent neuro-ophthalmological condition with a broad etiological spectrum. Population-based studies have shown that microvascular ischemia is the most common cause, followed by compressive, inflammatory, infectious, and neoplastic etiologies, particularly in older patients and those with vascular risk factors [7]. Consequently, identifying less common underlying causes may be challenging, especially in younger individuals without typical risk profiles.
Recognizing HIV infection as a potential underlying etiology in patients presenting with unexplained cranial nerve palsies is essential, particularly in young adults without known immunodeficiency or advanced disease. This report describes a case of isolated oculomotor nerve palsy leading to the diagnosis of HIV infection, highlighting the importance of systematic evaluation and early consideration of HIV testing in the diagnostic workup of focal neurological deficits.
Case presentation
A 31-year-old man presented with a two-week history of progressive headache associated with left eyelid ptosis and binocular diplopia. The diagnostic workup was conducted over a one-week period and included early neuroimaging, followed by laboratory investigations and cerebrospinal fluid (CSF) analysis. His symptoms subsequently evolved to include anorexia and low-grade fever without documented temperatures exceeding 38 °C. There was no history of trauma, diabetes mellitus, hypertension, or vascular disease. He was not taking any regular medications and had no known drug allergies, with no previously diagnosed sexually transmitted infections. His family history was unremarkable.
On neurological examination, the patient was alert and oriented. Cranial nerve examination revealed a left oculomotor nerve palsy characterized by complete ptosis, impaired adduction, elevation, and depression of the left eye, with preserved abduction. Pupillary examination showed a dilated left pupil with reduced reactivity to light. The remaining cranial nerves were intact. Motor, sensory, cerebellar, and gait examinations were normal, and no signs of meningeal irritation were observed.
Initial laboratory investigations, including standard laboratory tests and angiotensin-converting enzyme levels, were within normal limits. A broad serologic evaluation for infectious etiologies was performed and was negative, covering testing for syphilis, hepatitis B virus, hepatitis C virus, cytomegalovirus, Lyme disease, and toxoplasmosis. Autoimmune screening, including antinuclear antibodies (ANA), extractable nuclear antigens (ENA), anti-double-stranded DNA antibodies (anti-dsDNA), and antiphospholipid antibodies, was also negative. CSF analysis revealed lymphocytic pleocytosis with a white blood cell count of 356 cells/mm³, elevated protein concentration of 1.31 g/L, and normal glucose level of 0.50 g/L, indicating an inflammatory profile. CSF infectious testing, including polymerase chain reaction and serologic analyses for syphilis, cytomegalovirus, herpes simplex virus, varicella-zoster virus, Lyme disease, Epstein-Barr virus, and Mycobacterium tuberculosis, was negative. Laboratory findings are summarized in Table 1.
Magnetic resonance imaging of the brain showed no evidence of aneurysm, mass lesion, hydrocephalus, leptomeningeal enhancement, or parenchymal abnormalities (Figure 1).
Cerebral MRI with arterial and venous angiographic sequences(A) Axial FLAIR image showing no parenchymal abnormalities; (B) Diffusion-weighted imaging showing no restricted diffusion; (C) Axial high-resolution T2-weighted image focused on the oculomotor nerve, showing no abnormality of its intracanalicular segment; (D) Time-of-flight MR angiography demonstrating normal intracranial arterial anatomy; (E) Maximum intensity projection of TOF MRA showing no aneurysm of the posterior communicating arteries; (F) Sagittal angiographic reconstruction showing no vascular abnormalityFLAIR: fluid-attenuated inversion recovery; TOF: time of flight; MRA: magnetic resonance angiography
Given the inflammatory CSF findings and the patient’s risk profile, further etiological investigation was pursued. Serologic testing for HIV was positive and confirmed by Western blot analysis, revealing a CD4 lymphocyte count of 396 cells/mm³ and an HIV viral load of 54,300 copies/mL.
Antiretroviral therapy was initiated following completion of the diagnostic workup. The patient demonstrated progressive neurological improvement over the subsequent weeks. At the three-month follow-up, neurological examination showed complete resolution of ptosis, normalization of pupillary reactivity, and full recovery of extraocular movements, with no residual cranial nerve deficits.
Discussion
Isolated cranial nerve palsy is an infrequent neurological presentation of HIV infection and may constitute an early neurological manifestation preceding diagnosis [1-3]. Although neurological involvement in HIV is well recognized, focal cranial neuropathies occurring in isolation remain less commonly reported and are often underrecognized in early infection.
The pathophysiology of cranial nerve involvement in HIV is likely multifactorial, involving direct viral neurotropism, immune-mediated inflammatory mechanisms, and para-infectious processes [4,5]. In the present case, the inflammatory CSF profile, absence of opportunistic infections, and normal neuroimaging findings argue against compressive, ischemic, or neoplastic causes and are suggestive of a presumed HIV-associated inflammatory cranial neuropathy. Microvascular ischemic palsy was unlikely given the patient’s age and absence of vascular risk factors. Tolosa-Hunt syndrome and neurosarcoidosis were considered but were not supported by imaging, laboratory findings, or clinical course. Notably, the preserved CD4 lymphocyte count supports previous observations that focal neurological manifestations may occur early in the course of HIV infection, independent of advanced immunosuppression [3,5].
Cranial nerve palsies related to HIV infection have been described in the literature, either as isolated findings or in conjunction with other neurological manifestations [6,8]. However, many reported cases occurred in the setting of advanced disease or opportunistic infections. In contrast, our patient presented with isolated oculomotor nerve palsy as the initial neurological manifestation leading to the diagnosis of HIV infection and achieved complete recovery following initiation of only antiretroviral therapy. This favorable outcome supports the hypothesis of a potentially reversible inflammatory cranial neuropathy temporally associated with early HIV infection.
Oculomotor nerve palsy warrants particular attention because of its association with potentially life-threatening etiologies, especially intracranial aneurysmal compression. Population-based studies have demonstrated that aneurysms, neoplasms, and inflammatory conditions represent significant causes of acquired third cranial nerve palsy and must be promptly excluded, particularly in cases with pupillary involvement. In this context, comprehensive neuroimaging and targeted CSF evaluation remain essential components of the diagnostic workup [9].
Conclusions
This case illustrates that isolated oculomotor nerve palsy can represent an initial neurological manifestation of HIV infection, even in the absence of advanced immunosuppression or known risk factors. It emphasizes the importance of a thorough and systematic diagnostic approach, including detailed neuroimaging and CSF analysis, to exclude compressive, vascular, inflammatory, and infectious causes. The favorable clinical outcome observed after initiation of antiretroviral therapy suggests that early recognition of HIV-related neurological involvement may allow for complete neurological recovery in selected cases. As this report describes a single clinical observation, these findings should be interpreted with caution and may not be generalizable. Clinicians should therefore consider HIV testing in young patients presenting with unexplained isolated cranial nerve palsies to avoid diagnostic delay and ensure appropriate management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Neurological manifestations of the acquired immunodeficiency syndrome (AIDS): experience at UCSF and review of the literature J Neurosurg Levy RM Bredesen DE Rosenblum ML 475495621985 https://thejns.org/view/journals/j-neurosurg/62/4/article-p 475.xml 298305110.3171/jns.1985.62.4.0475 · doi ↗ · pubmed ↗
- 2Neurological complications of acquired immune deficiency syndrome: analysis of 50 patients Ann Neurol Snider WD Simpson DM Nielsen S Gold JW Metroka CE Posner JB 403418141983 https://pubmed.ncbi.nlm.nih.gov/6314874/631487410.1002/ana.410140404 · doi ↗ · pubmed ↗
- 3Global HIV neurology: a comprehensive review AIDS Thakur KT Boubour A Saylor D Das M Bearden DR Birbeck GL 163184332019 https://pmc.ncbi.nlm.nih.gov/articles/PMC 6139090/2954744010.1097/QAD.0000000000001796 PMC 6139090 · doi ↗ · pubmed ↗
- 4Multiple cranial nerve palsy in an HIV-positive patient Indian J Ophthalmol Karna S Biswas J Kumarasamy N Sharma P Solomon S 118120492001 https://journals.lww.com/ijo/fulltext/2001/49020/multiple_cranial_nerve_palsy_in_an_hiv_positive.10.aspx 15884518 · pubmed ↗
- 5Neurologic complications of human immunodeficiency virus infection Continuum (Minneap Minn) Saylor D 13971421242018 https://pmc.ncbi.nlm.nih.gov/articles/PMC 8006925/3027324510.1212/CON.0000000000000647 PMC 8006925 · doi ↗ · pubmed ↗
- 6Incidence and etiologies of acquired third nerve palsy using a population-based method JAMA Ophthalmol Fang C Leavitt JA Hodge DO Holmes JM Mohney BG Chen JJ 23281352017 https://jamanetwork.com/journals/jamaophthalmology/fullarticle/25851242789300210.1001/jamaophthalmol.2016.4456 PMC 5462106 · doi ↗ · pubmed ↗
- 7Etiological distribution of isolated oculomotor nerve palsy: analysis of 633 patients and literature review Eur J Neurol Kim HJ Kim HJ Choi JY Yang HK Hwang JM Kim JS 0312024 https://pubmed.ncbi.nlm.nih.gov/38411317/10.1111/ene.16261 PMC 1123580038411317 · doi ↗ · pubmed ↗
- 8Neurological complications of HIV infection Lancet Neurol Mc Arthur JC Brew BJ Nath A 54355542005 https://pubmed.ncbi.nlm.nih.gov/16109361/1610936110.1016/S 1474-4422(05)70165-4 · doi ↗ · pubmed ↗