Intracerebral Hemorrhage Secondary to Solitary Fibrous Tumor: A Case Report
Ramón Castruita Meza, Mijail O Quintero Romero, Mauricio D Arteaga Parra, Christian Félix Montiel, Jorge A Cantu Hernandez, Luis F Manzano Romero, Jesus A Morales Gómez, Angel R Martínez Ponce de León

TL;DR
A rare brain tumor caused sudden bleeding in a patient's brain, leading to severe symptoms and requiring emergency surgery for diagnosis and treatment.
Contribution
This case report highlights the rare presentation of solitary fibrous tumors as a cause of intracerebral hemorrhage and acute neurological deterioration.
Findings
A 46-year-old woman presented with acute neurological symptoms due to a hemorrhage from a solitary fibrous tumor.
Complete tumor resection allowed for definitive diagnosis and improved clinical outcomes.
The case underscores the importance of considering rare neoplasms in cases of spontaneous intracerebral hemorrhage.
Abstract
Solitary fibrous tumors (SFTs) of the central nervous system are uncommon mesenchymal neoplasms that may remain clinically silent until they reach a significant size or produce neurological manifestations. Although these tumors are typically slow-growing, they can occasionally present with acute neurological deterioration when associated with intracerebral hemorrhage. Such presentations are uncommon and can make diagnosis and management particularly challenging. We report the case of a 46-year-old woman with no previous medical history who experienced sudden-onset severe headache, vomiting, and rapid neurological decline, ultimately requiring emergent airway protection. On arrival, she presented with a markedly depressed level of consciousness, anisocoria, absent pupillary responses, and severe hypertension. Brain computed tomography (CT) revealed a large left fronto-temporo-parietal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
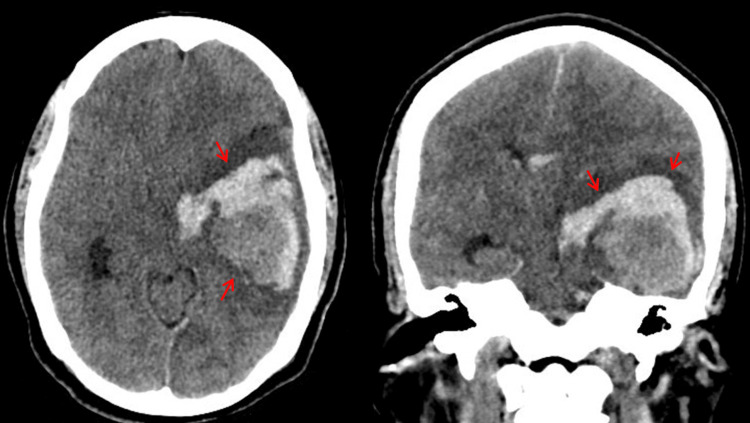 Figure 1
Figure 1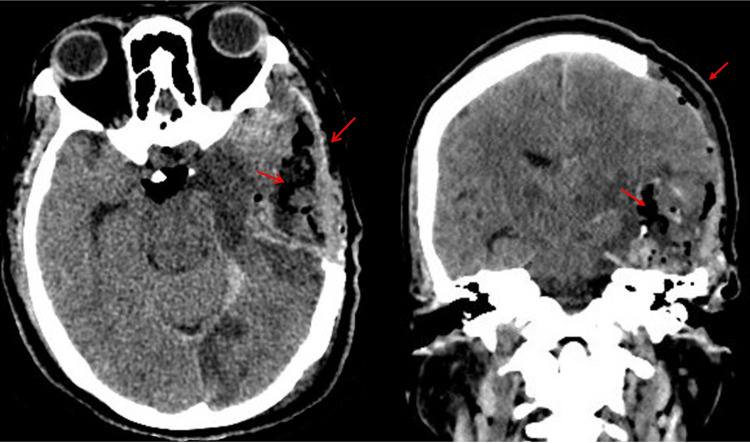 Figure 2
Figure 2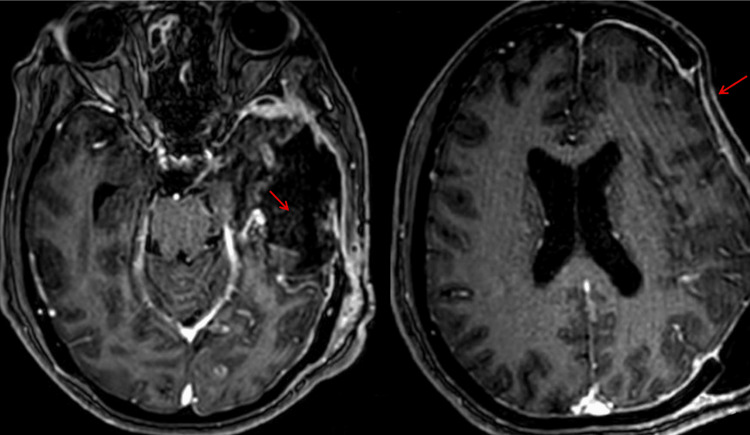 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumor case studies · IgG4-Related and Inflammatory Diseases · Spinal Hematomas and Complications
Introduction
Solitary fibrous tumor (SFT) (formerly known as solitary anaplastic fibrous tumor/hemangiopericytoma) is a rare mesenchymal neoplasm that typically arises from the dura mater and is defined by the NAB2-STAT6 gene fusion, which drives abnormal pericytic cell proliferation [1]. According to the current World Health Organization (WHO) brain tumor classification, these tumors are graded from 1 to 3 based on mitotic activity, cellularity, and necrosis [2], which correlate with biological behavior.
Intracranial SFTs represent less than 1% of primary central nervous system (CNS) tumors and may mimic meningiomas radiologically, making diagnosis challenging [3]. Nuclear STAT6 immunoreactivity is the diagnostic hallmark [1,2]. While many SFTs exhibit a slow-growing and relatively benign course, higher-grade lesions carry a greater risk of local recurrence and distant metastasis [2,4]. Complete surgical resection remains the cornerstone of treatment, and adjuvant radiotherapy is generally considered in cases with aggressive histology or subtotal resection [5,6].
In this report, we present a case of an intracranial SFT with an uncommon and rarely documented clinical presentation. We highlight its clinical, radiologic, and histopathologic features alongside management considerations.
Case presentation
A 46-year-old woman with no previous medical history was admitted with sudden-onset intense headache, right-sided significant muscular weakness, and three episodes of vomiting. The patient developed acute respiratory distress, needing airway management through orotracheal intubation, and had a Glasgow Coma Scale (GCS) score of 5, presenting a pupil size of 2 mm and 5 mm in the right and left sides, respectively, with a bilateral absent light reflex, generalized augmented tendon reflexes, and high blood pressure (190/100 mmHg).
A non-contrast skull computed tomography (CT) scan revealed an intracerebral hematoma within the left fronto-temporo-parietal region, causing a mass effect and midline shift (Figure 1).
Non-contrast skull computed tomography showing the presence of a left fronto-temporo-parietal parenchymal hematomaAxial and coronal non-contrast brain computed tomography demonstrating a left fronto-temporo-parietal intraparenchymal hematoma measuring approximately 41 cc in volume, with heterogeneous hyperdensity, surrounding hypodense edema, and mild mass effect on the adjacent cortical structures (red arrows).
An urgent decompressive craniectomy was performed, and the hematoma was evacuated. During the procedure, a tumoral mass was observed, which was resected and sent as a pathology sample (Figures 2-3).
Postoperative non-contrast skull computed tomography scan showing no residual injuryFollow-up axial and coronal non-contrast brain computed tomography showing postoperative changes in the left fronto-temporo-parietal region, with a surgical cavity, residual pneumocephalus, resolution of the previously noted midline shift, and no evidence of residual hematoma or acute intracranial hemorrhage (red arrows).
Follow-up brain magnetic resonance imaging (simple and contrast) showing postoperative changes with no residual injuryFollow-up axial brain magnetic resonance imaging demonstrating postoperative changes in the left fronto-temporo-parietal region, with a post-surgical cavity and mild linear peripheral enhancement, without evidence of residual lesion, recurrent hemorrhage, abnormal mass enhancement, or midline shift (red arrows).
Histopathological analysis of the tumor revealed a dense stromal pattern conformed by numerous hyalinized bands surrounding cellular nodules. No signs of necrosis or anaplasia/advanced dedifferentiation were found. Immunohistochemical staining revealed that cells were positive for STAT6. Histopathological diagnosis was established as an SFT (STAT6+) (Figure 4).
Pathological findings of solitary anaplastic fibrous tumor/hemangiopericytoma(A) Histological sections stained with H&E. Low-power view: The lesion is composed of a neoplasm with a hypocellular to moderately cellular pattern, consisting of a proliferation of spindle-shaped cells arranged in a disorganized pattern, with alternating hypocellular and hypercellular areas. The stroma is fibrous to collagenized, and numerous thin-walled vessels are identified. (B) Histological sections stained with H&E. High-power view: The tumor cells are spindle-shaped, with scant eosinophilic cytoplasm and oval to elongated nuclei, finely granular chromatin, and inconspicuous nucleoli. Scattered mitotic figures are identified (arrows), without marked nuclear atypia. No areas of tumor necrosis or significant pleomorphism are observed. (C) Immunohistochemistry: The neoplastic cells show strong and diffuse nuclear positivity for STAT6, consistent with NAB2-STAT6 gene rearrangement. This finding is highly specific for solitary fibrous tumor.H&E: hematoxylin and eosin
At the three-month follow-up, the patient showed clinical improvement, with a GCS score of 12, pupils at 3 mm, and improved muscle strength in the left side of the body with rigidity and paresthesia in the right side. Myotatic reflexes were increased, as were bilateral Hoffman's and Trömner's reflexes. The patient is scheduled for a follow-up brain magnetic resonance imaging (MRI), and a consultation with oncology is scheduled to assess treatment with radiotherapy.
Discussion
Intracerebral hemorrhage secondary to SFTs is rare and poses significant diagnostic and treatment challenges. The NAB2-STAT6 gene fusion, which stimulates major cellular proliferation, is associated with their pathogenesis [1]. Although it is rare, hemorrhage within these tumors can cause serious clinical symptoms [2], as in the current case, which required urgent surgical decompression and resection of the mass due to its hemorrhagic presentation.
Although SFTs are usually benign and slow-growing, some cases show increased mitotic activity associated with aggressive behavior and recurrence [3]. Rapid growth, vascular fragility, and abnormal tumor vasculature have been linked to hemorrhagic SFTs [4]. The patient presented with sudden-onset headache and neurological deterioration, consistent with previously reported hemorrhagic cases [5].
Surgical resection continues to be the standard treatment strategy, since it not only decreases the mass effect but also lowers the probability of recurrence [6]. However, adjuvant radiation may be necessary for certain patients to improve long-term outcomes; especially in cases with incomplete resection or high mitotic indexes, entire or subtotal resections are recommended [7]. Adjuvant post-surgical radiation is a procedure that has been associated with higher rates of survival in aggressive SFTs [8]. It is crucial to remember that the various reported cases have different treatment philosophies and there is ongoing discussion over the relevance of radiation therapy [9].
Prognosis is influenced by tumor grade, extent of resection, and presence of hemorrhage [10]. After surgery, some patients have a full recovery, but others suffer from long-lasting neurological impairments or tumor recurrence. Despite treatment, a substantial percentage of cases in our review had poor outcomes because of tumor growth or recurrence. The patient in the present case continued to have right-sided hemiparesis and motor aphasia despite showing no indications of tumor recurrence at follow-up, highlighting the necessity of ongoing neurological surveillance.
Conclusions
SFTs rarely present with spontaneous intracerebral hemorrhage, yet when they do, the clinical trajectory can be catastrophic. This case is notable due to the acute hemorrhagic presentation requiring emergent decompressive surgery. This emphasizes the significance of early detection, early surgical intervention, and ongoing surveillance. The primary therapeutic approach is surgical resection, and in cases with high proliferative activity, adjuvant radiotherapy is recommended. Heightened awareness of this presentation may shorten the time to diagnosis and intervention, resulting in better patient outcomes in these infrequent but clinically relevant tumors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intracranial solitary fibrous tumor: report of two cases Medicine (Baltimore) Sun LJ Dong J Gao F 098201910.1097/MD.0000000000015327 PMC 683122531027104 · doi ↗ · pubmed ↗
- 2A review of solitary fibrous tumor/hemangiopericytoma tumor and a comparison of risk factors for recurrence, metastases, and death among patients with spinal and intracranial tumors Neurosurg Rev Giordan E Marton E Wennberg AM Guerriero A Canova G 129913124420213255667910.1007/s 10143-020-01335-x · doi ↗ · pubmed ↗
- 3A comprehensive review on solitary fibrous tumor: new insights for new horizons Cancers (Basel) Martin-Broto J Mondaza-Hernandez JL Moura DS Hindi N 29131320213420092410.3390/cancers 13122913 PMC 8230482 · doi ↗ · pubmed ↗
- 4Intracranial solitary fibrous tumor/hemangiopericytomas: a clinical analysis of a series of 17 patients Br J Neurosurg Chenhui Z He G Wu Z 6176243820243433406610.1080/02688697.2021.1944980 · doi ↗ · pubmed ↗
- 5Hemangiopericytoma/solitary fibrous tumor of the cranial base: a case series and literature review BMC Surg Peng Z Wang Y Wang Y 2892220223589707110.1186/s 12893-022-01718-5PMC 9327149 · doi ↗ · pubmed ↗
- 6Intracranial solitary fibrous tumor/hemangiopericytoma: role and choice of postoperative radiotherapy techniques Front Oncol Gou Q Xie Y Ai P 9943351220223624902210.3389/fonc.2022.994335 PMC 9554559 · doi ↗ · pubmed ↗
- 7Intracranial solitary fibrous tumors: a heterogeneous entity with an uncertain clinical behavior World Neurosurg Gubian A Ganau M Cebula H 0126201910.1016/j.wneu.2019.01.14230716501 · doi ↗ · pubmed ↗
- 8Management of meningeal solitary fibrous tumors/hemangiopericytoma; surgery alone or surgery plus postoperative radiotherapy?Acta Oncol Haas RL Walraven I Lecointe-Artzner E 35416020213298826810.1080/0284186 X.2020.1826574 · doi ↗ · pubmed ↗