Quercetin and Its Nano‐Based Formulations Against Skin Cancer: A Narrative Review
Mahtab Khanyabzadeh, Alireza Emamifar, Nikoo Emtiazi, Amir Nazari, Masoumeh Shekarriz, Amin Karami, Fateme Hashem Beik Mahallati, Rahineh Nomani Lafmejani, Atieh Dariush, Seyed Mohammad Mahdi Rohani, Elaheh Mohseni Vadeghani, Negin Khoshnood, Hamid Reza Ojaghi

TL;DR
This review explores how quercetin, a natural compound, and its nano-based formulations may offer new treatment options for skin cancer by improving its effectiveness and delivery.
Contribution
The novelty lies in integrating natural compound therapy with nanotechnology to address limitations in skin cancer treatment.
Findings
Quercetin modulates pathways like apoptosis and DNA repair to inhibit skin cancer cell growth.
Nano-based delivery systems enhance quercetin's stability, permeability, and bioavailability.
Preclinical studies show improved therapeutic effects with nano-formulated quercetin.
Abstract
Skin cancer is one of the most prevalent malignancies worldwide, characterized by the abnormal growth of skin cells and significant clinical challenges. Conventional treatments—including surgery, chemotherapy, and radiotherapy—often suffer from limitations such as adverse side effects, tumor resistance, and inadequate efficacy. In this context, natural compounds have garnered attention as alternative therapeutic agents. Quercetin, a flavonoid widely distributed in fruits and vegetables, is recognized for its anti‐cancer, anti‐inflammatory, and antioxidant properties. However, its clinical application is hindered by poor solubility, low bioavailability, and limited skin permeation. Recent advances in nanotechnology have led to the development of nano‐based formulations that can enhance the pharmacological performance of quercetin, offering promising avenues for skin cancer management.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
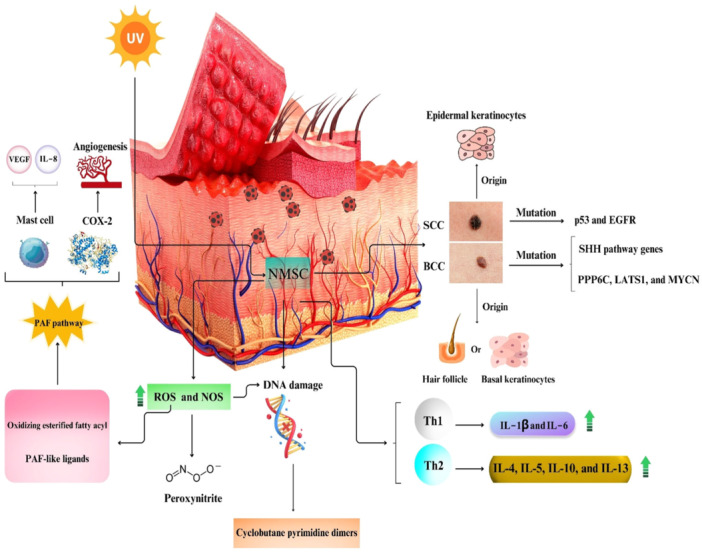 Figure 1
Figure 1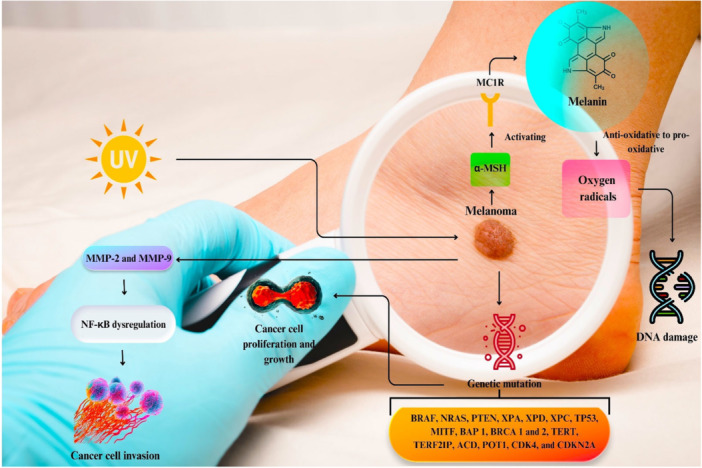 Figure 2
Figure 2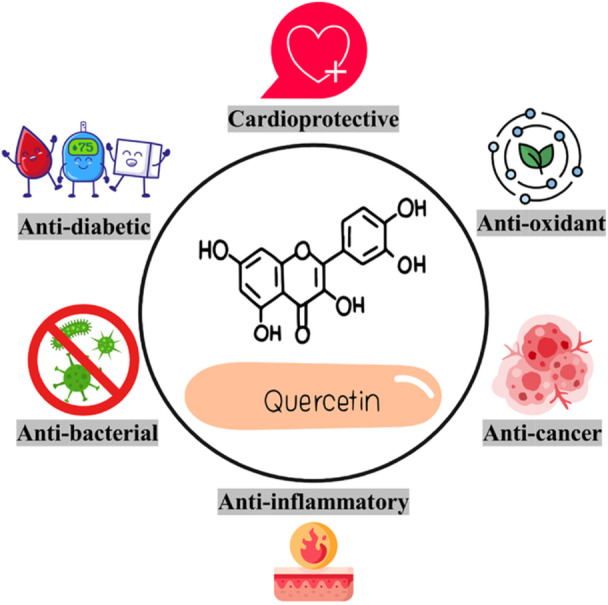 Figure 3
Figure 3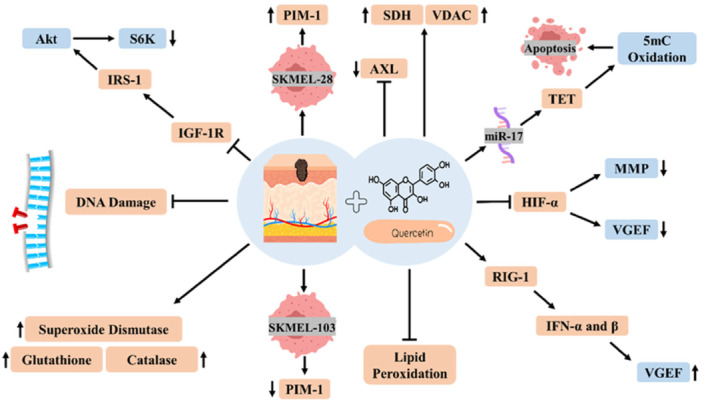 Figure 4
Figure 4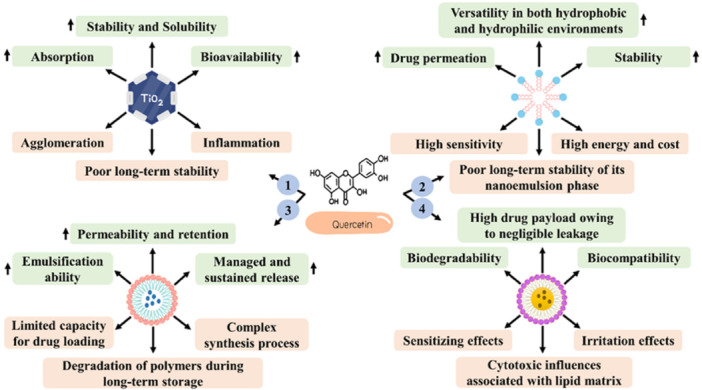 Figure 5
Figure 5| Study type | Number | Key focus | Examples |
|---|---|---|---|
| In vitro | 13 | Apoptosis, proliferation inhibition in melanoma/SCC/BCC cells | B16, A375, SK‐MEL‐28 |
| In vivo | 1 | Tumor reduction in mouse models (DMBA/croton oil) | Papilloma incidence delay |
| In vitro and in vivo | 4 | Inflammation and cell viability | IFN‐α, IFN‐β, STAT3 |
| Nanoformulations (preclinical) | 7 | TiO2 NPs, nanoemulgels, PLGA‐TPGS enhancing bioavailability/efficacy | A431, B16‐F10 cells |
| Reviews/Mechanistic | 5 | Pathways (e.g., P53, STAT, IGF‐1, HIF‐1), ROS modulation | Comprehensive overviews |
| Dose/concentration (s) | Target (s) | Effect/mechanism (s) | Major finding (s) | In vivo/In vitro | Species | Cell line (s) | Reference |
|---|---|---|---|---|---|---|---|
| 100 mg/kg and 50 and 100 μM | TET1 and miR‐17 | Stimulating apoptosis and repressing cell migration and invasion |
Quercetin induces TET1‐caused apoptosis Quercetin elevates the expression of TET1 (a target gene of microRNA‐17) | In vivo and in vitro | Nude mice | B16, SK‐MEL‐1, and OCM‐1 | [ |
| 50 and 100 µM | SDH, VDAC, PIM‐1, AXL, HIF‐1α, Akt, HSP90, and HSP70 | Attenuating the expression of tyrosine kinase receptors, elevating the expression of mitochondrial proteins, and decreasing cell viability |
Quercetin decreases the cell viability of SKMEL‐103 cells without affecting SKMEL‐28 cells The anti‐cancer effects of quercetin against SKMEL‐103 cells are stronger than kinase inhibitors (e.g., Erlotinib, Temsirolimus, and Imatinib) | In vitro | — | SKMEL‐28 and SKMEL‐103 | [ |
| 0–50 µM | Caspase 3, Nrf2, NF‐κB, and MAPK | Promoting or attenuating ROS production and cell growth dose dependently |
Quercetin at high concentrations decreases the growth of melanoma cells. In contrast, at low concentrations, it has the inverse impact on metastatic melanoma spheroids but not on the non‐metastatic cell line High quercetin concentrations (> 12.5 µM) reduce cell viability, while low concentrations (< 6.3 µM) promote cell proliferation and spheroid size | In vitro | — | MCM DLN, MCM 1G, and 1205Lu | [ |
| 0.1–100 mg/mL | — | Stimulating apoptosis, repressing cell proliferation, and decreasing cell viability |
Quercetin therapy leads to a 75% decrease in the viability of B16 melanoma cells The decrease in cancer cell viability was similar to or greater than that observed with etoposide, a well‐known chemotherapeutic agent | In vitro | — | B16 | [ |
| 3, 15, 75 mg/kg and 0.1–10 µM | IFN‐α, IFN‐β, and RIG‐I | Repressing tumor growth, inducing apoptosis, and inhibiting cell proliferation |
Quercetin serves as a RIG‐I agonist Quercetin enhances the expression of IFN‐α and IFN‐β by triggering the RIG‐I promoter in B16 cells | In vivo and in vitro | Wild‐type C57BL/6J male mice | A375 and B16 | [ |
| 50 and 100 mg/kg and 0–200 µM | Phospho‐JNK, Bax, phospho‐ERK1/2, phospho‐p38, Bcl‐2, and cleaved poly‐ADP ribose polymerase | Stimulating apoptosis, attenuating cell viability and proliferation, and repressing tumor growth |
Quercetin considerably reduces the proliferation and viability of A375SM cells in a concentration‐dependent way without affecting A375P cells | In vivo and in vitro | Female BALB/c nude mice | A375P and A375SM | [ |
| 25–150 µM | — | Regulating mitochondrial and glycolytic mechanisms for ATP generation by reducing indices related to oxygen consumption rate and extracellular acidification rate |
Seventy‐two hours of therapy with quercetin reduces all oxygen consumption rate‐related indicators (i.e., proton leak, basal respiration, maximal respiration, reserve capacity, and ATP turnover) | In vitro | — | B164A5 | [ |
| 25 and 50 µM | DR4, DR5, and FLIP | Inducing apoptosis |
Quercetin serves by elevating the expression of rhTRAIL‐binding receptors DR4 and DR5 on cancer cells and by enhancing the proteasome‐associated degradation of the anti‐apoptotic protein FLIP | In vitro | — | WM164 and MeWo | [ |
| 5–40 μM | PARP‐1, caspase‐3, and caspase‐8 | Inducing apoptosis, decreasing cell viability, repressing cell growth, arresting cell cycle |
Quercetin enhances cell death in B16F10 cells exposed to UVB by increasing reactive oxygen species (ROS) production, depolarizing the mitochondrial membrane potential (ΔΨM), regulating the antioxidant defense response, and influencing calcium homeostasis | In vitro | — | B16F10 | [ |
| 20–80 μM | c‐Met, HGF, Gab1 (GRB2‐associated‐binding protein 1), PAK (p21‐activated kinases), and FAK (Focal Adhesion Kinase) | Repressing cell migration and invasion |
Quercetin inhibits melanoma cell migration and invasion dose‐dependently once induced by HGF PAK or FAK upregulation dramatically decreases the suppressive influence of quercetin on melanoma cell migration | In vitro | — | A375, A2058, sk‐mel‐2, and MeWo | [ |
| 200 and 400 mg/kg | — | Decreasing tumor size, DNA damage, the number of papillomas, the serum levels of bilirubin, glutamate pyruvate transaminase, alkaline phosphatase, and glutamate oxalate transaminase, elevating the levels of catalase, superoxide dismutase, and glutathione, and repressing the level of lipid peroxides |
Quercetin significantly reduces DNA damage in treated mice in comparison with mice treated with croton oil and 7, 12‐dimethyl benz (a) anthracene (DMBA) | In vivo | Swiss albino mice | — | [ |
| 100 mg/kg and 0–60 µM | STAT3, VEGF, MMP‐2, MMP‐9, and Mcl‐1 | Stimulating apoptosis, decreasing cell viability, repressing cell proliferation, migration, and invasion, and tumor growth |
Quercetin represses the STAT3 signaling pathway by regulating STAT3 phosphorylation and decreasing STAT3 nuclear localization As a result, transcription activity of the STAT3 is suppressed, and STAT3 targeted genes, including VEGF, Mcl‐1, MMP‐2, and MMP‐9, are downregulated | In vivo and in vitro | Male nu/nu BALB/c mice | A2058 and A375 | [ |
| 0–100 µM | DNApk and ΔNp73 | Inducing apoptosis |
Quercetin combined with Temozolomide eliminates drug insensitivity and considerably promotes apoptosis compared to either treatment separately Quercetin therapy confers ΔNp73 redistribution into the cytoplasm and nucleus, which is linked with elevated p53 transcriptional function | In vitro | — | SK Mel 5, SK Mel 28, and DB‐1 | [ |
| 5–75 µM | P53 and Bax | Increasing ROS levels, decreasing GSH levels, and inducing apoptosis |
In tyrosinase clones, quercetin reduces bioreduction potential and elevates ROS formation more significantly compared to control cells The stimulation of apoptosis confered by quercetin therapy was mediated by the p53/Bax pathway | In vitro | — | DB‐1 | [ |
| 20, 50, and 100 µM | — | Repressing DNA damage and scavenging free radicals |
DNA protective capacity of quercetin at the concentrations of 20 and 100 μM against free radicals in human melanoma cells (HMB‐2) is 40% and 80%, respectively | In vitro | — | HMB‐2 | [ |
| 0.5–20 µM | Tyrosinase | Promoting melanogenesis |
Quercetin therapy (1 or 20 μM) for 7 days increases melatonin amount compared with controls Cycloheximide or actinomycin‐D can block Tyrosinase activation conferred by quercetin | In vitro | — | HMVII | [ |
| 3.3 × 10−1 mM | PKC and MMP‐2 and ‐9 | Repressing cell invasion |
Quercetin reduces the gelatinolytic function of pro‐MMP‐9 in a dose‐dependent manner Quercetin shows a dose‐dependent ability to antagonize the increases in gelatinolytic function of pro‐MMP‐9 conferred by free fatty acids and phorbol‐12,13‐dibutyrate (PDB) | In vitro | — | B16‐BL6 | [ |
| 10−6–10−4 g/mL | Bcl‐2 | Repressing cell mobility and invasion, arresting cell cycle, attenuating cell proliferation and migration, and inducing apoptosis |
Quercetin retards the cell cycle in the S and G2–M stages of the cell cycle in a dose‐dependent manner Quercetin significantly suppresses the expression of Bcl‐2 (anti‐apoptotic protein) without a marked effect on Bcl‐XL (another anti‐apoptotic protein) | In vitro | — | B16‐BL6 | [ |
| Type of nanoformulation | Dose/concentration (s) | Effect/mechanism (s) | In vivo/In vitro/Ex vivo | Species | Cell line | Reference |
|---|---|---|---|---|---|---|
| Quercetin loaded with titanium dioxide NPs | 6.25–100 μg/mL | Decreasing cell viability, inducing ROS formation and cell death, and attenuating inflammation | In vitro | — | A375 | [ |
| Transliposomal gel loaded with quercetin | 2.5–50 µM | Exerting cytotoxic effects on cancer cells | In vitro | — | B16F10 | [ |
| Quercetin and curcumin loaded with optimized Mesoporous Silica NPs | 0–200 µM | Exerting cytotoxic effects on cancer cells | In vitro | — | A375 | [ |
| Nanoemulsion loaded with quercetin | 7.80–1000 μg/mL | Exerting cytotoxic effects on cancer cells | In vivo and in vitro | Male Wistar rats | A431 | [ |
| Nanosized emulsion comprising quercetin | 5 mg kg | Decreasing cell viability and tumor growth | In vivo and in vitro | C57BL/6 mice | B16‐F10 | [ |
| Nanoformulated lipid carrier gel of quercetin and resveratrol | 12.5–200 µM | Exerting cytotoxic effects on cancer cells dose dependently | In vitro and ex vivo | — | A431 | [ |
| Nanogel of quercetin and titanium dioxide | Qu (0.12%) + TiO2 (5%) nanogel | Decreasing tumor volume, cell proliferation, and inflammation | In vivo | SKH‐1 mice | — | [ |
| ID number | Used quercetin | Cancer/Malignancy | Phase | Dose | Country |
|---|---|---|---|---|---|
| Isoquercetin (a glycosylated form of quercetin) | Colorectal cancer, non‐small cell lung cancer, and pancreatic cancer | Phases 2 and 3 | 500 and 1000 mg/daily for 28 days | United States | |
| Quercetin capsule | Blood malignancy | Phases 1 and 2 | 250 mg/daily for 21 days | Iran | |
| Quercetin and green tea extract | Prostate cancer | Phase 1 | — | United States | |
| Quercetin, curcumin, sulindac, and rutin | Colon cancer | — | — | United States |
| Type of formulation | Patent number | Intervention | Model | Year | Inventors |
|---|---|---|---|---|---|
| Polymeric nanoparticle (DSPE‑PEG)/Photo‑thermal agent | WO2022134862A1 | Organic conjugated polymer photo‑thermal agent for the treatment of malignant melanoma | In vitro | 2022 | Lei et al. |
| Palladium nanoparticle/Gold nanoparticle/Platinum nanoparticle/Bimetallic gold‑platinum nanoparticle/Bimetallic gold–palladium nanoparticle | US2022218741A1 | Synthesis of noble metal oxide nanoparticles by cell‐mediated processes and their biomedical applications | In vitro | 2022 | Medina et al. |
| Liposome/Trabectedin, Doxorubicin | WO2022115075A1 | Targeted nanoparticles that deliver dual drugs for melanoma therapy | In vitro | 2022 | Güliz et al. |
| Liposome/Veirofenib (Vemurafenib), Dacarbazine | CN113244174A | Melanoma chemotherapy drug‐loaded nano‐liposome and its preparation method | In vitro | 2021 | Qianqian et al. |
| Polymeric micelle/Acetogenin | ES2826205A1 | An approach for constructing a pharmaceutical composition using acetogenins combined with supramolecular polymeric micelles for skin cancer therapy | In vitro | 2021 | Teresa et al. |
| Liposome/anti‑PDL1, Catalase | CN110974957A | Utilization of catalase‐entrapped liposomes linked with PD‐L1 antibodies for the development of tumor treatment drugs | In vitro | 2020 | Shichen et al. |
| Polymeric nanoparticle (DSPE‑PEG2000)/Temozolomide | CN111481526A | Thermosensitive nanoparticles loaded with a cell‑penetrating peptide‐modified drug and their resistance to melanoma | In vitro | 2020 | Guan et al. |
| Carbonyl iron‑sulfur cluster nanoparticle | CN111281858A | Utilization of carbonyl iron‑sulfur clustercompound nanoparticles in drug synthesis | In vivo | 2020 | Hong et al. |
| Silver prussian blue nanoparticle | US10231996B2 | Silver prussian blue nanoparticles (SPB‑NPs: Ag3[Fe(CN) 6]) coated with a biocampatible polymer | In vivo | 2019 | Sudip et al. |
| Gold nanoparticle | US2019142980A1 | Cells loaded with gold nanoparticles for the treatment/diagnosis of melanoma | In vivo | 2019 | Angela et al. |
| Carbon nanotube | WO2018008825A1 | X‑ray brachytherapy system for the treatment of skin cancer and keloid by a carbon nanotube‑based X‑ray tube | — | 2018 | Oh et al. |
| Niosome/Doxorubicin | RU2600164C2 | A pharmacological gel based on Doxorubicin and organosilicon nanoparticles‑niosomes for skin cancer therapy | — | 2016 | Aleksandrovich et al. |
| Organometallic complex (iron‑based) | US2010119608A1 | Obtaining pH‑sensitive, acid‑stable metal‑binding nanoparticles | In vivo | 2010 | Fred et al. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhytochemicals and Antioxidant Activities · Curcumin's Biomedical Applications · Plant-Derived Bioactive Compounds
Introduction
1
Skin cancer is considered one of the most common cancers, with a mounting incidence that imposes remarkable pressure on healthcare systems [1]. This malignancy is related to the atypical growth of skin cells and is mainly developed in the areas subjected to ultraviolet (UV) rays [2]. In addition to UV light, several risk factors for skin cancer have been identified, such as impaired immune function, family history, arsenic compound exposure, and hereditary susceptibility [3, 4, 5]. Skin cancer can be categorized into two malignant types, comprising melanoma and non‐melanoma (squamous cell carcinoma [SCC] and basal cell carcinoma [BCC]). Conventional treatments like surgery, chemotherapy, and radiotherapy face limitations including side effects, resistance, and poor efficacy. Ergo, finding an alternative way to treat skin cancer with high efficiency and low challenge has been in the spotlight of scientists [6]. In the present era, natural compound‐based therapy is one of the popular therapeutic strategies to improve multiple human diseases, for instance, cancer, diabetes, neurodegenerative impairments, and cardiovascular diseases [7]. Natural compounds, particularly flavonoids, are chemical compounds with a natural origin obtainable from plants, fruits, fungi, etc., that possess a broad range of pharmacological benefits, such as anti‐inflammatory, antimicrobial, and anti‐cancer effects [8]. In this line, some popular natural compounds, particularly quercetin, a flavonoid compound extracted from onion, broccoli, and grapes, have been offered in skin cancer treatment in experimental studies [9, 10, 11]. Quercetin (C_15_H_10_O_7_), visible as a yellow powder, is one of the lipophilic natural agents with different pharmacological capacities, including anti‐inflammatory and antioxidative potentials, which have an indispensable role in making protection against skin damage induced by UV radiation [12]. Despite quercetin's potential to target skin cancer pathways, for instance, by inducing apoptosis and cell cycle arrest), challenges like low solubility and bioavailability necessitate harnessing alternative approaches, especially nano‐formulations [13]. Nowadays, several nano‐based drug delivery systems have been suggested for these natural compounds, like liposomes, nanoparticles (NPs), nanogels, polymers, and micelles, which effectually promote water solubility and bioavailability, therefore potentiating the efficacy while attenuating the toxic effects on normal cells [14]. Hence, studies regarding nano‐based herbal medicine against skin cancer are being conducted more and more. By this token, this narrative literature review aims to discuss the anti‐cancer potential of quercetin and its nano‐based formulations mechanistically in preclinical models as well as obstacles for clinical translation.
Method
2
In this narrative review, related documents with the status of “In press” and “Published” in the English language were evaluated qualitatively. Databases searched included Google Scholar, Scopus, PubMed, Web of Science, and Scientific Information Databases using keywords: “Skin cancer,” “Melanoma,” “Basal cell carcinoma,” “Squamous cell carcinoma,” “Quercetin,” “Nanotechnology,” and “Nano” until March 1, 2025. Initial searches retrieved 1247 records after duplicates were removed (total initial hits: 2156). Two independent investigators (MK and AE) screened titles and abstracts, excluding 1089 irrelevant records, followed by a full‐text review of 158 articles. Ultimately, 30 studies met the inclusion criteria: original and review articles focusing on quercetin and its nano‐based formulations in skin cancer (melanoma, BCC, SCC) across preclinical (in vitro/in vivo) or clinical settings; peer‐reviewed with adequate data. Exclusions comprised non‐relevant topics, insufficient information, or non‐peer‐reviewed sources. Disputes were resolved by a third reviewer (FRT). A summary of the included studies is given in Table 1.
Skin Cancer Pathogenesis
3
SCC and BCC
3.1
SCC stems from epidermal keratinocytes with malignant proliferation properties [15]; however, BCC may originate from the hair follicle or basal keratinocytes of the interfollicular epidermis [16]. Environmental (especially UVB radiation) and genetic agents have a substantial role in the pathogenesis of non‐melanoma skin cancers (NMSCs) [17]. DNA damage resulting from UVB radiation leads to DNA structural changes, like cyclobutane pyrimidine dimers, causing a failure in DNA repair and alterations in the transcription and replication processes [18]. Besides DNA damage, UV can form reactive nitrogen and reactive oxygen species (ROS), leading to DNA oxidative damage. UV also raises cutaneous nitric oxide (NO) levels by stimulating NO synthase. Accordingly, increased ROS and NO levels lead to the production of peroxynitrite, an endogenous oxidant with high toxicity to DNA [19, 20]. Increased ROS production can oxidize esterified fatty acyl remnants and provide platelet‐activating factor‐like (PAF‐like) ligands. These events induce the PAF pathway, forming cyclooxygenase (COX) 2 and activating mast cells [21]. Elevated COX2 expression in NMSCs has been related to the promotion of angiogenesis and cancer cell invasion [22, 23, 24]. BCC incidence is accompanied by the overexpression of Th2 cytokines (e.g., IL‐4, IL‐5, and IL‐10) (Figure 1) [25, 26]. Other reports showed that the levels of Th1 cytokines, like IL‐1β and IL‐6, in BCC are higher than in SCC [26]. Following these occurrences, the upregulation of oncogenes, like glioma‐associated oncogene (GLI1), neuroblastoma RAS (NRAS), and Kirsten RAS (KRAS), and downregulation of tumor suppressor genes, such as neurogenic locus notch homolog protein 1 (Notch 1), have also been detected [18]. Sonic hedgehog (SHH) pathway is another key player in the pathophysiology of BCC [27, 28]. In this pathway, the binding of an SHH ligand to a transmembrane protein receptor (PTCH) suppresses the SMO, a proto‐oncogene, triggering transcription factors of the GLI [27]. In BCC, the lack of PTCH1 receptor activity is related to activation of the G protein‐coupled receptor SMO and Hedgehog signaling pathway [29]. Reportedly, about 85% of sporadic BCCs harbor mutations in SHH pathway genes, especially loss‐of‐function (LOF) mutations in PTCH. Moreover, BCC can carry mutations in other cancer‐associated genes, like PPP6C, LATS1, and RAS family members [30]. In SCC, p53 mutation and inactivation are considered key events of disease pathogenesis [29]. SCC development is regulated through a sophisticated interaction between different genes, comprising epidermal growth factor receptor (EGFR), cyclin‐dependent kinase inhibitor 2A (CDKN2A), TP53, and Notch 1, as well as the phosphoinositide 3‐kinase (PI3K)/Akt/mammalian target of rapamycin (mTOR) signaling pathways [31]. Besides, it has been confirmed that matrix metalloproteinase (MMP)−2 protein expression in SCC cases is higher than in BCC, addressing the vital role of MMP‐2 in the invasive behavior of skin tumors [32].
A summary of pathogenic mechanisms in non‐melanoma skin cancers (NMSCs).
Melanoma
3.2
Subjection to UV rays results in the secretion of α‐melanocyte‐stimulating hormone (α‐MSH), activating the melanocortin 1 receptor (MC1R) to produce melanin by melanogenesis [33]. Melanin has a compilation of pro‐oxidant and anti‐oxidant features. Under the influence of different etiological agents, like UV radiation, herbicides, and heavy metals, melanin can be converted from an anti‐oxidative to a pro‐oxidative element (Figure 2) [34, 35]. This phenomenon is the earliest pathogenic occurrence that activates carcinogenic processes. When melanin acts as a pro‐antioxidant agent, DNA damage is expected due to the elevation of intracellular oxygen radicals. The change in DNA sequence triggers diverse signaling pathways that finally cause unmanaged cell proliferation, immortalization, and dedifferentiation of particular cells [36]. Investigations have revealed that approximately 40%–50% of all melanoma patients represent an activated mutation in the BRAF proto‐oncogene encoding a serine/threonine protein kinase as a subset of the RAS/RAF/MEK/ERK kinase pathway, which potentiates cell proliferation and growth [37]. Mutations in the NRAS oncogene are also detected in 15%–20% of melanoma cases [38]. Alterations in the DNA sequence of other genes, for example, PTEN, XPA, and XPD, can indicate inherited melanoma [39]. Besides these processes, MMPs, especially MMP‐2 and ‐9, which have an inducer role in degrading extracellular matrix components, aid tumor cell infiltration and expansion. The upregulation of these proteins is linked with genetic changes and nuclear factor kappa B (NF‐κB) signaling pathway dysregulation [40]. According to reports, NF‐κB stimulates MMP‐9 overexpression by instigating osteopontin (OPN) as a protein associated with tumor microenvironment [41]. Also, the intragenic methylation process causes MMP‐9 overexpression in melanoma [42].
A summary of pathogenic mechanisms in melanoma.
Overview of Quercetin
4
Origin and Source
4.1
Quercetin originates from the Latin term “quercetum,” meaning oak forest, and is one of the main flavonoids found in a broad range of plants and fruits. As a substantial component of the human diet, quercetin frequently exists chiefly as glycosylated derivatives in fruits (e.g., cherries, berries, apples, red grapes, and tomatoes), vegetables (garlic, onions, shallots, kale, and broccoli), and herb‐based beverages (red wine and herbal teas) [43, 44].
Physicochemical Properties
4.2
Quercetin is classified into a flavonoid class named 3‐hydroxyflavones. The molecular formula and weight of quercetin are C_15_H_10_O_7_ and 302.24 g/mol, respectively. Its chemical structure (Figure 3) consists of hydroxyl groups at locations of C‐3′ and C‐4′ of the B‐ring, C‐5 and C‐7 of the A‐ring, and C‐3 of the C‐ring, which has a defining role in the number of derivatives and pharmacological capacities [45]. Several derivatives of quercetin exist, including glycosides and methylated derivatives, as well as the less common prenyl and sulfate substituents [46]. Quercetin is commonly conjugated with rutinose and glucose in glycosidic forms, and the hydroxyl group at C‐3 is the most common glycosylation site [47]. Generally, quercetin is known as a lipophilic agent with low bioavailability and solubility and a 3.5 h‐half‐life [43]. Its estimated aqueous solubility is 1 μg/mL, while it is 28.9 μg/mL in intestinal fluid and 5.5 μg/mL in gastric fluid [48]. It is worth mentioning that quercetin solubility is different among its derivatives and indeed attributable to the kind of substituents. For example, glycosylated forms of quercetin are capable of elevating its hydrophilicity [49]. The primary site for absorbing this flavonol is the small intestine, though it can also be absorbed in the stomach. The absorption is mediated by passive diffusion for the aglycone or the sodium‐glucose cotransporter‐1 (SGLT1) for glycosides [50]. One of the main pharmacological challenges of quercetin is its poor bioavailability in light of its absorption profile, chemical stability, and low water solubility [51]. It is stated that only 20% of the orally prescribed dose of quercetin is absorbable. The bioavailability of quercetin is remarkably limited by intestinal metabolism [52]. In the first stage, it is metabolized by cytochrome P450 enzymes. In the second stage, conjugation occurs in the small intestine through glucuronidation, methylation, and sulfation [53]. Subsequently, the metabolites are released into the lymphatic circulation and bloodstream. When quercetin is taken orally, it is excreted through feces and urine; however, some metabolites are also excreted via the gallbladder [54].
Quercetin and its biological benefits.
Pharmacological and Biological Capacities
4.3
Quercetin is known as a safe flavonoid with a broad range of pharmacological and biological features [55]. These beneficial features include anti‐cancer [56], anti‐inflammatory [57], antioxidant [58], and immunomodulatory [59] influences. Moreover, numerous studies have indicated its anti‐fungal [55], anti‐viral [47], anti‐bacterial [60], anti‐diabetic [61], hepatoprotective [62], cardioprotective [63], neuroprotective [64], and renoprotective [65] capacities by triggering different signaling pathways. This evidence highlights the health benefits of quercetin in the current medical era and encourages researchers to seek other pharmacological aspects.
Quercetin and Pharmacological Concerns
4.4
Although numerous studies have shown that quercetin possesses a tremendous therapeutic potential for treating health‐threatening diseases, some concerns need to be considered. Low bioavailability, poor permeability, poor water solubility, instability, poor absorption, and retention in cells are among the main pharmacological challenges of quercetin therapy [66, 67]. Moreover, poor tumor‐targeting biodistribution, short half‐life, rapid systemic elimination, rapid metabolism, poor absorption, and limited skin permeation are other pharmacological problems that limit its extensive use in the clinic for cancer therapy via oral or topical routes [68, 69]. Alongside these concerns, the presence of some side effects and drug interactions motivates scientists to find alternative approaches to cancer treatment [70]. A number of toxicity‐related studies have demonstrated organ toxicity following high‐dose quercetin administration in animal models, particularly liver toxicity and nephrotoxicity [70, 71]. Routinely, oral consumption of quercetin in humans appears to be safe and well‐tolerated. Many clinical trials have confirmed the safety of quercetin with doses up to 1 g/day [72]. The emergence of non‐serious side effects, like headache, mild tingling of the extremities, and mild stomach discomfort, has been reported after quercetin intake with doses up to 5 g daily [73]. On the other hand, some animal studies have reported adverse effects, for example, decreased body weights, the appearance of non‐neoplastic hyperplastic polyps of the cecum, and the existence of calcium oxalate crystals in the urine, following a high‐dose quercetin administration (1900 and 2100 mg/kg). Furthermore, yellow‐brown pigmentation in the small intestine and glandular stomach following quercetin therapy in high doses was observed, which may be caused by the yellow color of quercetin or by one of its metabolites [74, 75, 76]. Animal and human investigations have also displayed that quercetin can change the bioavailability of diverse drugs, leading to an increased likelihood of adverse drug effects. Some animal projects have divulged that quercetin is able to elevate the drug bioavailability of several anti‐cancer drugs (e.g., doxorubicin, paclitaxel, and irinotecan), ranolazine (an anti‐anginal drug), tamoxifen (an antiestrogen drug), valsartan (an anti‐hypertensive drug), and digoxin (a drug against heart failure) [77, 78, 79, 80, 81, 82, 83]. In human studies, drug bioavailabilities were decreased in talinolol (antihypertensive drug) and midazolam (sedative) and increased in fexofenadine (antihistamine drug) and pravastatin (cholesterol‐lowering drug) [84, 85, 86, 87]. Moreover, one study has stated that quercetin (25–100 mg/kg orally) decreases dose‐dependent catalepsy caused by intraperitoneal application of reserpine, α‐methyl‐p‐tyrosine, or perphenazine in rats [88]. Considering these pharmacological concerns, an alternative method should be applied that addresses these issues and enhances its efficacy against malignancies, like skin cancer.
Quercetin Against Skin Cancer
5
Several preclinical studies have underscored the anti‐cancer potential of quercetin for skin cancer through different mechanisms and signaling pathways (Table 2). To shed more light on this subject, an in vitro study claimed that the anti‐melanoma effects of quercetin are thanks to inhibiting tyrosine kinase receptors (PIM‐1 and AXL) and elevating the expression of mitochondrial proteins (SDH and VDAC). In this investigation, quercetin could suppress AXL in two cell lines of SKMEL‐28 and SKMEL‐103; however, PIM‐1 expression was increased in SKMEL‐28 cells and decreased in SKMEL‐103 cells following the treatment. Also, a decrease in hypoxia‐inducible factor‐1α (HIF‐1α) expression was observed in both cell lines [89]. HIF‐1α has tumor‐enhancing impacts in melanoma by potentiating VEGF secretion and inducing MMPs [90]. One of the interesting outcomes of this work was that quercetin is more efficient than kinase suppressors like erlotinib, imatinib, U0126, and temsirolimus [89]. Another in vitro work scrutinized the anti‐carcinoma effects of this plant‐derived flavonoid on B16 murine melanoma cells and showed a 75% decrease in cell viability of B16 cells 6–48 h after quercetin therapy (50 μg/mL) [11]. The rate of cell viability reduction in quercetin‐treated cells was more than in cells exposed to etoposide, a chemotherapy drug. This flavonoid could also decrease the proliferative capacity of B16 cells more efficiently than etoposide. Moreover, quercetin decreased the number of cells in the stages of S and G2/M of the cell cycle. This happening can be justified by apoptosis induction, as evidenced by a flow cytometry test of Annexin V+ cells, a key protein binding to phosphatidylserine (PS), usable to detect apoptotic cells [11]. Ali et al. [61] inspected the chemopreventive capacity of quercetin in a mouse model of skin carcinoma established by topical administration of croton oil and 7, 12‐dimethyl Benz (a) anthracene (DMBA). Following disease establishment, quercetin (200 and 400 mg/kg for 16 weeks, orally) was prescribed [91]. The application of croton oil and DMBA in mice results in papilloma formation as well as liver damage, as evidenced by an increase in the levels of bilirubin, alkaline phosphatase (ALP), serum glutamic pyruvic transaminase (SGPT), and serum glutamic oxaloacetic transaminase (SGOT) [92]. The results of this experimental work pointed out the capability of this flavonoid to reduce papilloma numbers and the mentioned liver biochemical parameters. This natural product could also elevate the antioxidant defense system by elevating the levels of antioxidant enzymes (glutathione, catalase, and superoxide dismutase), attenuating lipid peroxidation, and diminishing DNA damage in animal models of skin carcinoma [91]. Jung et al. [93] investigated quercetin's influence on suppression of the insulin‐like growth factor 1 (IGF‐1) signaling pathway in transgenic mice, whose IGF‐1 expression level in their skin epidermis is considerably high [93]. They found that administration of a diet rich in quercetin (0.02% wt) postpones skin tumor incidence by 14 days and reduces the multiplicity of skin tumors by 35% in comparison with the control group treated with tetradecanoyl phorbol‐13‐acetate (TPA), a carcinogenic agent for mouse skin. Quercetin supplementation was also able to reduce TPA‐conferred skin hyperplasia in transgenic mice. To deliberate the action mechanisms of quercetin in suppressing skin tumor development in teratogenic mice, the phosphorylation of proteins related to the IGF‐1 signaling pathway in the MT1/2 cells (a papilloma cell line) was monitored after quercetin treatment (10–50 µM). In the end, quercetin repressed IGF‐1‐ caused phosphorylation of the IGF‐1 receptor (IGF‐1R), S6K, Akt, and insulin receptor substrate (IRS)−1 dose‐dependently, indicating IGF‐1 signaling suppression [93]. Lately, ten‐eleven translocation (TET) protein expression was investigated in an in vitro and in vivo study (2023) to examine the suppressive effects of quercetin on uveal melanoma cells [94]. TET protein catalyzes 5‐methylcytosine (5mC) oxidation and mediates apoptosis induction in some malignancies [95, 96]. The authors observed increased TET1 expression after quercetin therapy in melanoma cells, including B16, SK‐MEL‐1, and OCM‐1. Bioinformatic analyses also demonstrated that TET1 is the miR‐17 target gene. Consequently, this research team inferred that miR‐17 affects cell growth and apoptosis in malignant cells by regulating TET1 expression (Figure 4). These reports were consistent with the in vivo part of this study in which nude mice harboring OCM‐1 cells were treated with 100 mg/kg quercetin (for 21 days). In animal models of melanoma, quercetin repressed tumor growth compared with the untreated group [94]. Another preclinical study indicated the suppression of cell proliferation and induction of apoptosis as a result of quercetin therapy in A375 (1–60 μM) and B16 cells (0.1–50 μM). Molecular analyses confirmed that the utilization of this natural compound leads to the overexpression of interferon (IFN)‐α and ‐β by triggering retinoic acid inducible gene‐I (RIG‐I) promoter in melanoma cells (B16 cells). RIG‐I is a cytosolic PRR that identifies 5′‑triphosphate RNA produced by viral RNA polymerases and possibly promotes anti‐cancer impacts by triggering signal transduction and activator of transcription 1 (STAT1) in paracrine and autocrine signaling pathways. In vivo results of this preclinical work unveiled the attenuation of mouse melanoma growth, as shown by decreasing tumor volume, weight, and growth curve, in mice harboring B16 cells following intragastric application of quercetin (75 mg/kg/day) [97]. Other anti‐cancer capacities of quercetin in skin cancer have been summarized in Table 2.
Quercetin can target skin cancer through diverse cellular and molecular mechanisms.
Quercetin exhibits biphasic effects, acting as an antioxidant at low concentrations (< 40 μM) to protect cells but switching to pro‐oxidant at higher doses (40–100 μM), generating ROS, o‐quinone adducts, and depleting glutathione (GSH), which selectively induces apoptosis in cancer cells like melanoma while sparing normal cells. In skin cancer models, this pro‐oxidant activity enhances cytotoxicity in UVB‐irradiated B16F10 melanoma cells but may potentiate UV‐induced signaling like c‐Fos in some contexts. These dose‐dependent effects necessitate careful optimization to avoid unintended toxicity, such as organ damage observed in high‐dose animal studies [111].
Nano‐Based Formulations of Quercetin and Skin Cancer
6
Titanium Dioxide NPs
6.1
Recently, titanium dioxide (TiO_2_) (Figure 5) has been known as a favorable mineral in various fields thanks to its unique chemical and physical features. Currently, there are two crystal structures of TiO_2_, including anatase, with highly photocatalytic, and rutile; the second form (rutile) is less photocatalytic and more stable, and chemically is assumed inert [112]. Morphologically, TiO_2_ can be synthesized in the form of spherical particles, nanotubes, and nanowires/nanorods [113]. TiO_2_ possesses diverse advantages, such as being non‐toxic, safe, chemically and thermally stable, biocompatible, having outstanding optical properties, antimicrobial features, and the capability to absorb and scatter UV radiation, making it an interesting element in diverse daily products, such as skin care creams, toothpaste, and food colorants [114]. However, there are some limitations regarding these NPs. The possible toxicity of TiO_2_ NPs, especially once ingested or inhaled, has been one of the main concerns of these NPs because their application may give rise to inflammation and oxidative stress [115]. Other problems related to TiO_2_ NPs comprise poor photocatalytic performance under visible light, the tendency to agglomerate, causing reduced surface area and weak functionality in drug delivery‐related purposes, and high cost for synthesizing high‐quality TiO_2_ NPs [116, 117, 118].
Nano‐based formulations of quercetin can potentiate the therapeutic effectiveness of quercetin in the fight against skin cancer. 1, Titanium dioxide nanoparticles; 2, Nanoemulsion; 3, Nanostructured Lipid carrier; 4, PLGA‐TPGS nanoparticles.
It has been addressed that TiO_2_ NPs are one of the suitable choices to encapsulate quercetin in order to elevate its stability and solubility in aqueous media, leading to its bioavailability and absorption enhancement [119]. Also, these NPs are capable of safeguarding quercetin from enzymatic degradation and some environmental factors, for example, pH and light, aiding in its stability in the time of reaching the desired region [120, 121]. Moreover, these metallic NPs can overcome the pharmacological limitation of quercetin by minimizing systemic toxicity, reducing the need for high‐dose quercetin, and releasing it in a sustained and controlled manner [122, 123, 124].
Having considered the anti‐cancer capacity of quercetin against skin cancer, which was discussed above, and the biochemical benefits of these NPS, the anti‐skin cancer effects of TiO_2_NPs loaded with quercetin have been investigated [125]. In this line, Chahardoli et al. [125] have fabricated and characterized TiO_2_NPs loaded with quercetin (TiO_2_NPs‐Que) and assessed their biological features, such as cytotoxicity, anti‐inflammatory, and anti‐hemolytic influences, against melanoma cell lines (A375) in vitro. The characterization methods, including Transmission/Field‐Emission Scanning Electron Microscopy (TEM/FE‐SEM) and X‐ray diffraction (XRD), indicated that the designed TiO_2_NPs‐Que had a spherical shape, belonged to the rutile phase, and had a size range of 7.3–39 nm. TiO_2_NPs‐Que did not display hemolytic influences. They demonstrated 95.3% stabilization activity of red blood cell (RBC) membranes and 82.6% suppression of bovine serum albumin (BSA) denaturation, like a standard drug, validating their anti‐inflammatory impacts. Cytotoxicity‐related data indicated the toxicity of the synthesized nano‐based formulation of quercetin on A375 without considerable effects on normal skin fibroblast cells [125]. The reason behind this result can be related to its potential to increase ROS formation, causing cancer cell death [125, 126]. Ergo, it is suggested that TiO_2_NPs‐Que can exert anti‐cancer effects against skin cancer by reducing cell viability and inflammatory reactions and increasing ROS production, resulting in cell death. Nevertheless, additional experimental evidence is needed to support this theory.
Nano‐based systems like TiO_2_ NPs and nanoemulgels improve quercetin's delivery but introduce NP‐specific risks, including inflammation, oxidative stress, agglomeration, poor long‐term stability, and potential organ accumulation, particularly with TiO_2_ inhalation or ingestion. Contradictory preclinical data highlight variable efficacy across formulations, with some showing selective cancer cell toxicity but others raising concerns over skin irritation from surfactants or scalability issues. Balanced assessment reveals that while nano‐quercetin enhances bioavailability, unresolved safety profiles limit clinical readiness [127].
Nanoemulgel
6.2
Structurally, nanoemulgels are known as hybrid colloidal systems established by nanoscale oil droplets distributed in a gel‐based aqueous matrix, putting together the features of both hydrogels and nanoemulsions [128]. A nanoemulsion is also a liquid formulation with a high stability pharmacokinetically, featuring droplet diameters ranging from 10 to 100 nanometers [129]. These formulations have several superiorities over traditional options, comprising enhanced penetration to deeper skin layers, promoted drug solubility, and a reduced dosage, resulting in minimized dose‐associated side effects [129].
Thanks to nanoemulgel, the easy incorporation of lipophilic drugs, as well as the potentiation of permeability of the combined drugs, is conceivable owing to disseminated droplets related to the nanoemulsion phase. Accordingly, the pharmacodynamic and pharmacokinetic parameters of lipophilic drugs are considerably enhanced [130].
Overall, the current evidence suggests that nanoemulgel offers a variety of benefits. These include enhanced drug permeation, improved stability, and versatility in both hydrophobic and hydrophilic environments [131, 132, 133]. Additionally, nanoemulgel aids in the targeted delivery of drugs, provides controlled release, and typically causes fewer side effects than traditional formulations, making it less irritating to the skin [134].
Despite these, some challenges are limiting the wide utilization of nanogel‐based drug delivery systems. One of these issues is related to the stability of the gel phase. Most of the gelling agents have a high sensitivity to temperature and pH changes [130]. Other problems comprise the need for high energy and cost to nanoemulsion preparation, the restricted long‐term stability of its nanoemulsion phase, and the possibility of incidence of dermatitis and skin irritation following its application due to a high amount of surfactant [135, 136, 137].
One of the nano‐based strategies for improving pharmacological challenges and enhancing the anti‐cancer effects of quercetin against skin cancer has been developed based on nanoemulgel [69]. Nanoemulgel can overcome the restriction of quercetin in cancer therapy by promoting stability and bioavailability, improving release capacity, decreasing quercetin therapy‐related side effects, and boosting skin penetration for topical applications [69, 138].
In this regard, Chitkara and colleagues designed a stable quercetin nanoemulgel by adding Carbopol 940 (a gelling agent) through an ultrasonication emulsification technique and appraised its toxicity in vivo and effectiveness on human skin cancer cells (A431) in vitro. The characterization of the fabricated nanoemulgel was carried out using SEM, Fourier Transform‐Infrared (FT‐IR) spectroscopy, assessment of zeta potential and entrapment efficiency (%EE), and particle size analysis. Moreover, the designed quercetin‐loaded nanoemulgel was characterized by determining pH and viscosity and evaluating the texture profile. The nanoemulgel had a nanosize (173.1 ± 1.2 nm) along with decreased polydispersity index (0.353 ± 0.13), zeta potential (−36.1 ± 5.9 mV), and suitable %EE (90.26%). The toxicity assessments showed that the nanoemulgel is well‐tolerated and safe, given that no organ toxicity or skin irritation was observed in Wistar rats. Moreover, the nanoformulation was safe for topical utilization. In vitro reports indicated that quercetin nanoemulsion had a higher releasing capacity compared with the pure suspension of quercetin (85% vs. 26%) in vitro in light of its small globular size, giving rise to large surface area for promoting hydrophobic drug solubility and elevating diffusion rate. The outcomes also revealed that the nanoemulgel form of quercetin had higher cytotoxicity to A431 cells than the pure quercetin, likely because of the usage of olive oil in this nanoformulation, which possesses anti‐cancer effects on skin carcinomas [69]. The anti‐cancer potential of olive oil has been addressed through different mechanisms, such as apoptosis induction and its effect on tumor proliferation and metabolism [139]. Another experimental study examined the impacts of oral application of a nanosized emulsion comprising quercetin on the cytotoxicity of melanoma in vitro (B16‐F10 cells) and in vivo (mice bearing B16‐F1O cells) (Table 3) [140]. The nanosized emulsion was designed through hot solvent diffusion related to the phase inversion temperature techniques. In vitro outcomes implicated a decrease in cell survival dose‐dependently for pure quercetin and nanoemulsion of quercetin. In in vivo assessments, quercetin was administered either as a pure drug or in a colloidal dispersion at a dose of 5 mg/kg two times per week for 17 days orally. Results pointed out that both pure quercetin and quercetin nanoemulsion reduced tumor growth; however, the effect was more significant in animals treated with quercetin nanoemulsion. In addition, there was no evidence showing hepatic or renal toxicities following the administration of quercetin in either its pure or nanoformulated forms [140]. These reports highlighted that the oral bioavailability of quercetin improved once the compound was incorporated into the oily phase of a nanosized emulsion, offering a potential application in skin cancer treatment. Moreover, the anti‐skin cancer effects of quercetin nanoemulgel were emphasized by addressing its role in attenuating cell viability and tumor growth.
Poly (d,l‐Lactide Co‐Glycolide) (PLGA) NPs Emulsified With TPGS
6.3
Nowadays, NPs obtained by biodegradable copolymers like Tocopheryl polyethylene glycol 1000 succinate (TPGS)‐conjugated Poly (d,L‐lactide co‐glycolide) (PLGA) (PLGA‐TPGS) hold promise in drug delivery systems [145]. Poly (d,L‐lactide co‐glycolide) (PLGA) is a biodegradable polymer approved by the Food and Drug Administration (FDA) with acceptable biodegradability and biocompatibility; thus, the PLGA‐based NPs can be a good choice for carrying hydrophobic or hydrophilic drugs [146, 147]. PLGA‐TPGS NPs are composed of three main subsets, including PLGA Core, TPGS Shell, and drug payload (a drug encapsulated in the PLGA core) [148]. The core of these NPs is made from PLGA, which is a copolymer of glycolic acid and lactic acid [149]. TPGS, a natural vitamin E derivative soluble in water, acts as a shell around the PLGA and is extensively applied as a bioavailability, solubilizer, and emulsifier of hydrophobic drugs [150].
PLGA‐TPGS NPs possess wide applications due to their improved cellular uptake, high emulsification ability, enhanced biocompatibility and biodegradability, safety, stability, managed and sustained release, and enhanced permeability and retention (EPR) influence [150, 151, 152]. On the contrary, complex synthesis process, limited capacity for drug loading, and degradation of polymers during long‐term storage are the main challenges related to PLGA‐TPGS NPs.
Interestingly, PLGA‐TPGS NPs loaded with quercetin have been recommended by Zhu and co‐workers to combat skin damage arising from UVB [153]. In this study, PLGA‐TPGS NPs were synthesized via the nanoprecipitation method. The NPs had a core‐shell structure, with hydrophobic PLGA providing the core encapsulating the water‐insoluble quercetin and a TPGS segment serving as the hydrophilic stabilization shell. The encapsulation efficiency and drug content of quercetin‐loaded PLGA‐TPGS NPs were almost 81.7% and 8.62%, respectively, revealing a good performance for a suitable drug delivery system. This research team found that quercetin encapsulated with PLGA‐TPGS NPs (100–300 μL/mL) can solve the problem related to the poor hydrophilicity of quercetin and exert anti‐UVB impacts by suppressing inflammatory mediators (NF‐kB and COX‐2) and mitigating histopathological features caused by UVB irradiation in human keratinocyte cell lines (Hacat cell line). Thanks to this nanocarrier, quercetin was considerably more sustainable in the dermis/epidermis than in the stratum corneum, indicating the potential ability of LGA‐TPGS NPs for skin delivery of quercetin. The histopathological analyses of this work manifested that quercetin‐loaded NPs attenuated the UVB‐conferred erratic arrangement of collagen fiber, reduced the thickness of dermal collagen fiber, and increased epidermal thickness [153]. Thus, PLGA‐TPGS NPs loaded with quercetin can, on the one hand, surmount the pharmacological obstacles of quercetin, mainly by enhancing its aqueous solubility, sustained and controlled release, and targeted delivery to selected regions. On the other hand, they can have a protective role against skin damage arising from UVB radiation, mainly by modulating histopathological, immunological, and inflammatory factors.
Nanoformulated Lipid Carrier
6.4
Nanoformulated lipid carriers are new drug delivery systems that contain physiological and biodegradable solid and liquid lipids, which have been inspected for targeted transportation of drugs to the skin [154]. These structures are second‐generation lipid nano‐transporters that are fabricated by a solid lipid matrix combined with liquid lipids [155]. This type of carrier, unlike emulsions, can efficiently immobilize drugs and prevent particle coalescence due to the solid matrix [155]. Nanoformulated lipid carriers have attractive biomaterial characterizations, such as small size, biodegradability, and biocompatibility, EPR impact, the existence of a disordered crystal structure, stability, and high drug payload owing to negligible leakage, and the feasibility of formulating over liposomes and solid lipid nanoparticles (SLN) [156, 157]. The small size of these nanoformulations ensures close contact with the skin, increasing the amount of drug that penetrates the skin [158]. The usage of nanoformulated lipid carrier gel topically provides a lipid film on the skin that limits trans‐epidermal water loss (TEWL), promotes skin moisture, and keeps it hydrated [159, 160]. The limitations of the application of nanoformulated lipid carriers include cytotoxic influences associated with lipid matrix, irritation and sensitizing effects of surfactants, and issues related to the stability of lipids [161].
Imran et al. [143] proposed the topical application of a nanoformulated lipid carrier gel containing quercetin and resveratrol in skin cancer to improve their distribution in epidermal and dermal layers in vitro and ex vivo. This nano‐based formulation included a surfactant (Cremophor RH40) and lipid binary mixture (1.0% w/w). The mean particle size and polydispersity index of the nanoformulated lipid carrier were 191 nm ± 5.20 and 0.33 ± 0.01, respectively, showing dispersion homogeneity and competency of the formulated nanogel for dermal delivery. The cytotoxic evaluations of various concentrations (12.5–200 μM) of the gel in A431 cell lines were carried out using the MTT method. The permeability and flux coefficients of quercetin and resveratrol from nanoformulated lipid carrier gel were 3.70 μg/cm²/h, 14.09 μg/cm²/h, and 4.69 × 10^−2^ cm/h, and 7.21 × 10^−2^ cm/h, respectively, suggesting their good potential for deeper layers of the skin. This formulation also had a high entrapment effectiveness and drug loading due to the solubility of these two natural compounds in lipids and the disorganized crystal structure of the nanogel. IC50 values for conventional gel, which was obtained using Carbopol P934 (a polymer of acrylic acid cross‐linked with polyalkenyl alcohols), and nanoformulated gel were 123.64 and 86.50 μM, respectively, revealing the higher cellular toxicity and more anti‐skin cancer influences of the nanogel on A431 cells than the conventional gel [143]. On the whole, it seems that nanoformulated lipid carrier gel not only can solve pharmacological limitations of quercetin therapy by elevating aqueous solubility, permeability, managed and sustained release, and drug loading capacity, but also can target skin cancer cells through the reduction of cell viability of cancer cells; however, more in‐depth studies are needed to illustrate the anti‐cancer mechanisms of this nano‐based formulation.
Other Nano‐Based Formulations
6.5
In addition to the mentioned nano‐based formulations of quercetin, which have been discussed in skin cancer therapy, there are experimental data recommending some nano‐based drug delivery systems, such as quercetin‐loaded transliposomal gel and optimized mesoporous silica NPs (MSNs) [141, 142].
Liposomes are defined as spherical lipid vesicles, typically ranging from 50 to 500 nm in diameter, that consist of one or more lipid bilayers made by synthetic lipids or emulsifying natural lipids in an aqueous medium [162]. Liposomes are broadly utilized as NPs in nanomedicine owing to several key advantages, including their stability, biocompatibility, simplicity for synthesis, bioavailability, and high drug loading capacity [163, 164, 165]. Besides, the excipients required in these formulations are generally safe [166]. Their unique characteristics, encompassing size and hydrophilic and hydrophobic properties, allow liposomes to effectively encapsulate drug molecules, either within the lipophilic membrane or within the aqueous interior of the vesicles [167]. Ergo, liposomes are known as promising drug delivery systems. Regrettably, liposomes also have some restrictions, like weak targeting, short‐time circulation in vivo, and the likelihood of the fusion leakage of loaded drugs [168, 169].
Lately, Kalam et al. [141] have investigated the dermal usage of fabricated and optimized transliposomes loaded with quercetin (TLQ), based on the ethanol injection method, against melanoma in vitro. This research pointed out that TLQ may solve the pharmacological challenges of quercetin by promoting the skin permeation of quercetin, showing an elevated permeability of quercetin from TLQ and a sustained release pattern. In addition, it was shown that TLQ not only has more antioxidant function but also can decrease the cell viability of B16F10 melanoma cells more effectively than pure quercetin [141].
MSNs are composed of a mesostructured porous network belonging to silicon oxide, which is formed by harnessing the hydrolytic sol‐gel method. This approach comprises the hydrolysis and condensation of silicon alkoxide precursors in basic or acidic circumstances, utilizing a surfactant template [170]. MSNs have suitable biodegradability and biocompatibility and favorable chemical stability, positioning them as a good choice for drug delivery‐related goals [171]. Despite these benefits, MSNs encounter some barriers. For example, the kidney, liver, and other organs may receive encapsulated drugs non‐specifically and confer systemic toxicity [172]. Other limitations of MSNs include compatibility problems, unmanaged degradability, and weak potential for drug encapsulation, which negatively affect their medical uses [173]. Intriguingly, in another scientific effort, optimized MSNs were utilized in order to discover whether this nano‐based platform can boost skin permeation and exert cytotoxic effects on melanoma cells. In this work, MSNs were fabricated via the sol‐gel method and optimized using a Box‐Behnken design. The attained findings revealed that MSNs had favorable sustained profiles in drug release and skin permeation, making them a suitable approach to elevate the effectiveness of quercetin therapy for melanoma. Moreover, the MTT results demonstrated that MSNs loaded with quercetin are more successful in serving as a cytotoxic agent against A375 Melanoma cells [142].
Clinical Translation: What Are the Challenges?
7
Although quercetin‐based nanoformulations have recently attracted much attention as potential anti‐cancer therapies in the current era; however, there are some limitations that hinder their clinical applications [174]. The substantial challenges associated with translating quercetin‐based nanoformulations into clinical practice comprise biological problems, safety‐related concerns, biocompatibility, large‐scale manufacturing difficulties, government regulations, intellectual property rights, and unaffordable costs [175]. The transition to the clinical application of quercetin‐based nanoformulations is mainly hindered by biological obstacles and their unclear fate at the diseased site in biological systems [176, 177]. In these systems, nanomaterials interplay with various biomolecules, resulting in the formation of what is known as a “bio‐corona.” The bio‐corona is referred to as different biomolecules, including lipids, peptides, and proteins, that are linked with a NP surface once it is encountered by a biological system. The bio‐corona has a controlling role in the nanodrug efficacy and affects the function of adaptive and natural immunity [178]. Given that NPs and biological aggressors have the same size range, the possibility of interactions with agents related to the immune system increases. So, a main barrier in nanomedicine is the accurate examination of the fate of nano‐based drugs as anti‐cancer agents in the biological system [179]. Overall, certain criteria should be considered to expedite the clinical translation of nanoformulations [1]: The influences of physicochemical features of nanoformulations and their possible mechanisms on their toxicity are still opaque and must be comprehended prior to entering clinical practices, and [2] the benefits provided by nano‐based formulations must outweigh their production costs [180]. So, an achievement in clinical translation of nanoformulations is not always easy to work; it demands in‐depth preclinical research, carefully chosen clinical indications, appropriate design, and faithful implementation of clinical trials.
Clinical Attempts and Registered Patents
8
According to data reported from Clinical Trials.gov, the clinical investigation of treatment with quercetin or its nano‐based formulations against skin cancer has not been initiated yet. However, there are some ongoing clinical assessments to show the anti‐cancer potential of quercetin or its combined formulation with dasatinib (a second‐generation inhibitor of tyrosine kinases) against some diseases, including breast cancer, head and neck SCC, and childhood cancer (https://clinicaltrials.gov). Moreover, it has been stated that some clinical trials related to quercetin therapy, either alone or combined, are in the final stage. These clinical studies have investigated the effectiveness of capsulated quercetin, combined quercetin, or a glycosylated form of quercetin (isoquercetin) on some cancers/malignancies, including colorectal cancer, prostate cancer, blood malignancy, non‐small cell lung cancer, and pancreatic cancer (Table 4). These clinical trials are conducted in various countries, mainly in the United States and Iran, and include different phases of clinical research ranging from Phases 1 to 3. The dosages of quercetin or its associated compounds differ from one trial to another. In some research, certain doses, such as 250 mg, 500 mg, or 1000 mg, are prescribed daily for a set period of time, whereas in others, the exact dosage has not been mentioned. In some clinical studies, quercetin is being studied accompanied by other substances like green tea extract, curcumin (a polyphenol obtained from Curcuma longa), sulindac (a nonsteroidal anti‐inflammatory drug), and rutin (a quercetin glycoside), showing that these combinations might work together to improve cancer treatment.
Table 4: Registered clinical trials (in the completed or terminated status) regarding the effects of quercetin on various cancers/malignancies worldwide (Source: https://clinicaltrials.gov).
There is also some patent literature available to aid scientists working on the application of nanoformulations for skin cancer. In Table 5, a collection of registered patents about the performance of nano‐based formulations for skin cancer treatment has been summarized based on data extracted from the Espacenet database (worldwide.Espacenet.com).
These patents cover a broad range of NPs, comprising liposomes, metallic NPs (e.g., gold, platinum, and palladium), polymeric NPs, and carbon‐based structures like nanotubes. The majority of these formulations are designed to deliver drugs—like temozolomide, doxorubicin, and vemurafenib —in targeted ways to treat melanoma and other skin cancers more effectively. Some patents have noticed the usage of pH‐sensitive organometallic complexes, photothermal agents, and bimetallic NPs, whereas others concentrate on combining NPs with antibodies or peptides in order to target tumor regions better. Collectively, these scientific efforts include lab studies for potential clinical utilization, with specific attention to improving how drugs are delivered, overcoming resistance, and establishing systems that are safe for the human body.
Barriers to Clinical Translation
9
No clinical trials specifically evaluating quercetin or its nanoformulations for skin cancer treatment have been conducted to date, despite promising preclinical data. Key barriers include safety concerns, such as quercetin's dose‐dependent pro‐oxidant effects leading to potential organ toxicity (e.g., liver/kidney damage at high doses > 1 g/day) and NP‐related risks like inflammation, oxidative stress, and accumulation in skin or systemic organs.
Regulatory hurdles further complicate translation, as novel nanoformulations require extensive toxicological profiling under FDA/EMA guidelines for nanomaterials, including genotoxicity, biodistribution, and long‐term stability data, which current preclinical studies largely lack. High production costs for scalable, GMP‐compliant nano‐systems (e.g., TiO2 NPs, PLGA‐TPGS) involving complex synthesis, purification, and characterization limit feasibility for large‐scale manufacturing [127].
Perspectives and Challenges
10
In the last decades, nanotechnology has been recommended as a new hope to eliminate the limitations of traditional modalities for skin cancer treatment [181]. NPs, thanks to their potential to serve as anti‐cancer agents, tumor‐targeting moieties, skin permeability enhancers, and drug carriers, are generally assumed to be serious candidates to treat this malignancy effectively [182]. As discussed through several experimental studies, nano‐based formulations of quercetin (e.g., titanium dioxide NPs, nanoemulsion, nanostructured lipid carriers, and PLGA‐TPGS NPs) have addressed considerable potential in skin cancer therapy in comparison with conventional strategies. These nanoformulations have changed the landscape of targeted therapy, chemotherapy, and immunotherapy in terms of needed dose, toxicity, therapeutic effectiveness, stability, etc [183]. In particular, for costly therapeutic approaches, like targeted therapy and immunotherapy, enhancing the therapeutic effectiveness with a minimum possible dose is of significance in lowering overall treatment costs [182]. One of the potential therapeutic opportunities for skin cancer is that several other nano‐based formulations have been recommended for skin cancer that can be used for effective and targeted delivery of quercetin to tumor regions [184]. For example, inorganic NPs, including cerium oxide NPs, copper oxide NPs, zinc oxide NPs, platinum, silver NPs, carbon nanotubes, gold NPs, and mesoporous silica, have been offered for skin cancer therapy. These inorganic NPs have several advantages, like small size, biocompatibility, bioactivity, large surface area, and functionalizing capability, which make them appropriate choices for skin cancer treatment [185, 186]. However, they can act as photosensitizing or photothermal agent, which are more commonly used in photodynamic or photothermal therapy [185]. Alongside inorganic NPs, polymer‐based NPs, such as dendrimer, polymersome, polymeric NPs, and polymeric micelle, have also exhibited their ability to adsorb, entrap, conjugate, or load anti‐cancer drugs (lipophilic and hydrophilic drugs, monoclonal antibodies, genes, etc.) for tumor targeting, monitored release, elevated tumor uptake, and safeguard in physiological circumstances [187, 188]. Other suitable types of NPs for skin cancer therapy are lipid‐based NPs. Lipid‐based NPs are unique drug delivery systems that consist of either lipid monolayer (nanostructured lipid carriers and solid lipid NPs) or lipid bilayer (e.g., ethosomes, niosomes, and liposomes) accompanied by aqueous core (ethosomes, niosomes, and liposomes), liquid lipid core (nanostructured lipid carriers), or solid lipid core (solid lipid NPs), wherein drugs can either dissolve or disperse to carry through different administration ways [189, 190]. However, one of the main challenges related to NPs is achieving suitable chemical, physical, pharmacodynamic, and pharmacokinetic features of NPs concerning mass, size, and unique shape. These features are also linked with the secondary features of NPs, like biocompatibility and toxicity [191]. The efficacy of most nanoformulations is affected by some biological challenges, such as biodistribution modulation and controlled NP permeation, across various biological obstacles [192]. Another key challenge for developing nano‐based formulations in the clinic is monitoring the biological fate of NPs. Plus, one of the important barriers of some NPs, especially inorganic NPs, is their prolonged retention in the body, which may increase the possibility of serious side effects, such as chronic toxicity [193].
Conclusion
11
This review demonstrates that quercetin exerts potent anti‐cancer effects against skin cancer through multiple mechanisms, including induction of apoptosis, cell cycle arrest, inhibition of proliferation, migration, and invasion, as well as modulation of pathways like IGF‐1, HIF‐1, and RIG‐I in preclinical models of melanoma, SCC, and BCC. Nano‐based formulations, such as TiO2 NPs, nanoemulgels, and PLGA‐TPGS NPs, significantly enhance these effects by improving quercetin's solubility, stability, skin permeability, bioavailability, and targeted delivery, leading to superior cytotoxicity against cancer cells compared to free quercetin while sparing normal cells.
Despite these promising findings, several challenges persist, including quercetin's inherent limitations of poor aqueous solubility, low bioavailability, rapid metabolism, and potential toxicity at high doses. Additionally, nanoformulation issues include particle stability, scalability, cost, and long‐term safety concerns, such as inflammation or organ accumulation. Clinical translation remains hindered by the scarcity of human trials, variability in nanoformulation efficacy across models, and regulatory hurdles for topical or systemic applications.
Future research should prioritize comprehensive preclinical optimization of nano‐quercetin systems, including dose‐response studies, biodistribution analyses, and combination therapies with standard treatments to overcome resistance. Rigorous clinical trials are essential to establish safety, efficacy, optimal dosing, and long‐term outcomes in skin cancer patients, paving the way for regulatory approval and clinical implementation.
Author Contributions
Mahtab Khanyabzadeh, Alireza Emamifar, Nikoo Emtiazi, Amir Nazari, Masoumeh Shekarriz, Amin Karami, and Fateme Hashem Beik Mahallati: conceptualization, methodology, supervision, writing, review and editing. Rahineh Nomani Lafmejani, Atieh Dariush, Seyed Mohammad Mahdi Rohani, Elaheh Mohseni Vadeghani, and Negin Khoshnood: resources, writing – review and editing, supervision. Hamid Reza Ojaghi, Fatemeh Rezaei‐Tazangi, and Reza Arefnezhad: formal analysis, methodology, visualization, writing – original draft.
Funding
The authors received no specific funding for this work.
Disclosure
All authors have read and approved the final version of the manuscript. The corresponding author had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The corresponding author Fatemeh Rezaei‐Tazangi affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. M. Smak Gregoor , T. E. Sangers , L. J. Bakker , et al., “An Artificial Intelligence Based App for Skin Cancer Detection Evaluated in a Population Based Setting,” NPJ Digital Medicine 6, no. 1 (2023): 90.37210466 10.1038/s 41746-023-00831-w PMC 10199884 · doi ↗ · pubmed ↗
- 2H. M. Balaha and A. E.‐S. Hassan , “Skin Cancer Diagnosis Based on Deep Transfer Learning and Sparrow Search Algorithm,” Neural Computing and Applications 35, no. 1 (2023): 815–853.
- 3M. Mehdizadeh , Z. Mehdizadeh , E. Jafarzadeh , et al., “Skin Cancer Prevention by Nutraceuticals.” Nutraceuticals in Cancer Prevention, Management, and Treatment (Apple Academic Press, 2024), 191–213.
- 4A. K. Gupta , M. Bharadwaj , and R. Mehrotra , “Skin Cancer Concerns in People of Color: Risk Factors and Prevention,” Asian Pacific Journal of Cancer Prevention: APJCP 17, no. 12 (2016): 5257–5264.28125871 10.22034/APJCP.2016.17.12.5257 PMC 5454668 · doi ↗ · pubmed ↗
- 5N. H. Matthews , K. Fitch , W.‐Q. Li , et al., “Exposure to Trace Elements and Risk of Skin Cancer: A Systematic Review of Epidemiologic Studies,” Cancer Epidemiology, Biomarkers & Prevention: A Publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 28, no. 1 (2019): 3–21.10.1158/1055-9965.EPI-18-0286 PMC 632496530297516 · doi ↗ · pubmed ↗
- 6X. Geng , X. Qiu , J. Gao , et al., “CREB 1 Regulates KPNA 2 by Inhibiting mir‐495‐3p Transcription to Control Melanoma Progression: The Role of the CREB 1/mi R‐495‐3p/KPNA 2 Axis in Melanoma Progression,” BMC Molecular and Cell Biology 23, no. 1 (2022): 57.36522613 10.1186/s 12860-022-00446-1PMC 9756468 · doi ↗ · pubmed ↗
- 7F. Rezaei‐Tazangi , A. Forutan Mirhosseini , A. Fathi , H. Roghani‐Shahraki , R. Arefnezhad , and F. Vasei , “Herbal and Nano‐Based Herbal Medicine: New Insights Into Their Therapeutic Aspects Against Periodontitis,” Avicenna Journal of Phytomedicine 14, no. 4 (2024): 430–454.38952769 10.22038/AJP.2023.23261 PMC 11179182 · doi ↗ · pubmed ↗
- 8A. Rasul , F. M. Millimouno , W. Ali Eltayb , M. Ali , J. Li , and X. Li , “Pinocembrin: A Novel Natural Compound With Versatile Pharmacological and Biological Activities,” Bio Med Research International 2013 (2013): 1–9.10.1155/2013/379850 PMC 374759823984355 · doi ↗ · pubmed ↗