Clinical Profile of Patients Admitted With Venous Thrombosis to a Tertiary Care Hospital in India
Bibin George, Sujeet Raina, Rajesh Sharma, Narvir S Chauhan, Krishna B Reddy

TL;DR
This study describes the clinical profile of Indian patients with venous thrombosis, highlighting the prevalence of deep vein thrombosis and the effectiveness of the modified Wells criteria in classifying cases.
Contribution
The study provides new clinical data on venous thrombosis in a hilly region of India and evaluates the modified Wells criteria's applicability in this population.
Findings
Deep vein thrombosis was the most common type of venous thrombosis observed in the study.
The modified Wells criteria classified most confirmed DVT and PTE cases as 'likely' when applied retrospectively.
Elevated D-dimer levels were prevalent across various venous thrombosis sites, with the highest in cerebral venous thrombosis.
Abstract
Background and objectives: Venous thrombosis is a frequent cause of hospitalization worldwide; however, data describing its clinical profile in Indian patients, particularly from hilly regions, remain limited. The present study aimed to describe the clinical profile of patients admitted with venous thrombosis to the medical wards of a tertiary care hospital in Himachal Pradesh, India. Additionally, we examined the prevalence of elevated D-dimer levels across different venous thrombosis sites and assessed the proportion of patients with confirmed deep vein thrombosis (DVT) and pulmonary embolism who would have been retrospectively classified as “likely” using the modified Wells criteria. Methods: This cross-sectional observational study was conducted over a one-year period. All adult patients admitted with clinically suspected and radiologically confirmed venous thrombosis who met the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
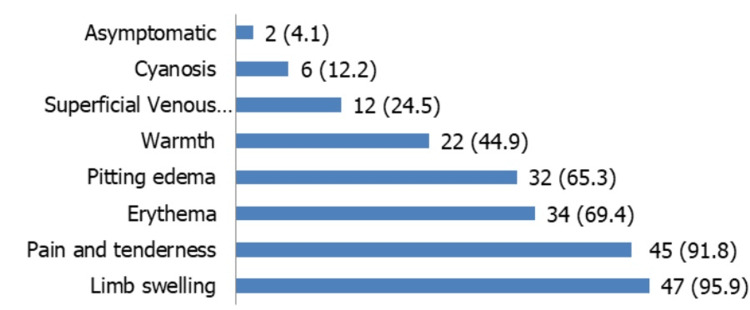 Figure 1
Figure 1| Age Group & Thrombus Site | 21-30 | 31-40 | 41-50 | 51-60 | 61-70 | >70 | Total |
| DVT | 3 | 13 | 8 | 7 | 8 | 5 | 44 |
| PTE | 1 | 1 | 4 | 2 | 0 | 1 | 9 |
| CVT | 3 | 2 | 2 | 0 | 0 | 0 | 7 |
| DVT + PTE | 1 | 0 | 1 | 0 | 0 | 1 | 3 |
| Isolated PVT | 1 | 1 | 1 | 0 | 0 | 0 | 3 |
| DVT + CVT | 0 | 0 | 1 | 0 | 1 | 0 | 2 |
| Isolated SVT | 0 | 1 | 0 | 1 | 0 | 0 | 2 |
| PVT+SVT | 0 | 0 | 1 | 0 | 1 | 0 | 2 |
| Isolated IVC | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| PVT + IVC | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| PVT + SVT | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| Superior Mesenteric | 1 | 0 | 0 | 0 | 0 | 0 | 1 |
| Total | 10 | 20 | 18 | 11 | 10 | 7 | 76 |
| Vessels involved | Frequency | Percentage |
| Femoral + popliteal vein | 19 | 38.8 |
| Isolated femoral vein | 11 | 22.4 |
| Isolated popliteal vein | 9 | 18.4 |
| Infrapopliteal vein | 2 | 4.1 |
| Femoral + GSV | 2 | 4.1 |
| Popliteal + infrapopliteal vein | 2 | 4.1 |
| Common iliac + external iliac + femoral | 1 | 2.0 |
| External iliac + femoral + popliteal+ GSV | 1 | 2.0 |
| Infrapopliteal + short saphenous vein | 1 | 2.0 |
| Axillary vein | 1 | 2.0 |
| Anterior tibial vein | 0 | 0.0 |
| Posterior tibial vein, peroneal vein | 0 | 0.0 |
| Presentation | Frequency | Percentage |
| Headache | 5 | 55.6 |
| Vomiting | 3 | 33.3 |
| Focal deficits | 2 | 22.2 |
| Convulsions | 1 | 11.1 |
| Altered sensorium | 1 | 11.1 |
| Fever | 1 | 11.1 |
| Vessels involved in PTE | Frequency | Percentage |
| Isolated main pulmonary artery | 7 | 58.3 |
| Isolated segmental branches | 2 | 16.7 |
| Isolated sub-segmental branches | 1 | 8.3 |
| Segmental + lobar artery | 1 | 8.3 |
| Pulmonary + segmental + lobar artery | 1 | 8.3 |
| Isolated lobar pulmonary artery | 0 | 0.0 |
| Predisposing Factors | DVT [n=49] n (%) | PTE [n=12] n (%) | CVT [n=9] n (%) | Other [n=11] n (%) | Total [n=76] n (%) |
| Smokers | 13 (26.5) | 5(41.7) | 1 (11.1) | 6 (66.7) | 25(32.9) |
| Tobacco chewers | 3 (6.1) | 0 | 0 | 0 | 3 (3.9) |
| Steroid abuse | 1 (2) | 0 | 0 | 0 | 1 (1.3) |
| OCP use | 1 (2) | 0 | 0 | 0 | 1 (1.3) |
| Hypertension | 7 (14.3) | 3 (25) | 0 | 2 (22.2) | 12(15.8) |
| Hyperlipidemia | 7 (14.3) | 2(16.7) | 1 (11.1) | 0 | 10(13.2) |
| Diabetes | 8 (16.3) | 2(16.7) | 0 | 2 (22.2) | 12(15.8) |
| RHD | 2 (4.1) | 0 | 0 | 0 | 2 (2.6) |
| CAD | 1 (2) | 0 | 0 | 0 | 1 (1.3) |
| Heart failure | 2 (4.1) | 0 | 0 | 0 | 2 (2.6) |
| Atherosclerotic peripheral artery disease | 2 (4.1) | 0 | 0 | 0 | 2 (2.6) |
| Stroke or transient ischemic attack | 2 (4.1) | 0 | 1 (11.1) | 0 | 3 (3.9) |
| Chronic kidney disease | 3 (6.1) | 1 (8.3) | 0 | 0 | 4 (5.3) |
| Gastrointestinal bleed | 0 | 0 | 0 | 4 (44.4) | 4 (5.3) |
| Sepsis | 6 (12.2) | 4(33.3) | 0 | 0 | 10(13.2) |
| a. Pneumonia (HAP/CAP) | 2 | 4 | |||
| b. Klebsiella | 1 | 1 | |||
| c. Klebsiella + Pseudomonas | 1 | 3 | |||
| d. Urosepsis | 2 | 0 | |||
| e. Rickettsial | 2 | 0 | |||
| Varicose veins | 2 (4.1) | 0 | 0 | 0 | 2 (2.6) |
| Pregnancy | 0 | 0 | 0 | 0 | 0 |
| LSCS | 4 (8.2) | 1 (8.3) | 0 | 0 | 5 (6.6) |
| Chronic liver disease | 0 | 0 | 0 | 2 (22.2) | 2 (2.6) |
| COPD | 1 (2) | 2(16.7) | 0 | 0 | 3 (3.9) |
| DCMP | 2 (4.1) | 0 | 0 | 0 | 2 (2.6) |
| Hypothyroidism | 3 (6.1) | 0 | 0 | 0 | 3 (3.9) |
| Hematological disorder | 2 (8.2) | 0 | 2 (22.2) | 0 | 4 (5.3) |
| a. Acute leukemia | 1 | 0 | 1 | ||
| b. Multiple myeloma | 1 | 0 | 1 | ||
| Malignancy | 8 (16.3) | 2(16.7) | 4 (44.4) | 2 (22.2) | 16(21.1) |
| Recent surgery | 4 (8.2) | 0 | 0 | 0 | 4 (5.3) |
| Recent immobilization | 3 (6.1) | 1 (8.3) | 0 | 0 | 4 (5.3) |
| Fracture shaft of femur | 1 (2) | 0 | 0 | 0 | 1 (1.3) |
| Previous DVT prophylaxis | 3 (6.1) | 1 (8.3) | 0 | 0 | 4 (5.3) |
| HIV infection | 1 (2) | 0 | 0 | 0 | 1 (1.3) |
| HCV infection | 0 | 0 | 0 | 1 (11.1) | 1 (1.3) |
| Tuberculosis | 4 (8.2) | 4(33.3) | 0 | 1 (11.1) | 9 (11.8) |
| Pulmonary | 4 | 4 | 0 | ||
| Extrapulmonary | 0 | 0 | 1 | ||
| Obesity | 10(20.4) | 3 (25) | 1 (11.1) | 2 (22.2) | 16(21.1) |
| Overweight | 8 (16.3) | 0 | 0 | 2 (22.2) | 10(13.2) |
| Connective tissue disorder | 4 (8.2) | 0 | 0 | 0 | 4 (5.3) |
| a. SLE | 2 | ||||
| b. Systemic sclerosis | 1 | ||||
| c. Mixed connective tissue disorder | 1 | ||||
| Thrombophilia profile | 0 | ||||
| a. Hyperhomocysteinemia | 6 (12.2) | 0 | 3 (33.3) | 9(11.8) | |
| b. Protein C deficiency | 0 | 0 | 0 | 0 | |
| c. Protein S deficiency | 1 (2) | 0 | 0 | 1(1.3) | |
| d. Prothrombin gene mutation | 0 | 0 | 0 | 0 | |
| e. Factor V laden mutation | 0 | 0 | 0 | 0 | |
| f. Antiphospholipid antibody syndrome | 2 | 0 | 0 | 2(2.6) | |
| g. Hypofibrinogenemia | 0 | 1 (8.3) | 1(11.1) | 2(2.6) |
| Venous thromboembolism type | Elevated D-dimer (n) | Total cases (N) | Proportion (%) |
| Deep vein thrombosis | 45 | 49 | 91.8 |
| Pulmonary thromboembolism | 12 | 12 | 100 |
| Cerebral venous thrombosis | 8 | 9 | 88.9 |
| Other venous thrombosis | 9 | 11 | 81.8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Cerebral Venous Sinus Thrombosis · Vascular anomalies and interventions
Introduction
Venous thrombosis is a common cause of hospitalization globally and venous thromboembolism (VTE) represents the third most common cause of death from cardiovascular disease worldwide, after myocardial infarction and stroke [1]. Thrombus can be defined as an aggregate of coagulated blood containing platelets, fibrin, and entrapped cellular elements within the vascular system, in accordance with standard pathology definitions. Deep vein thrombosis (DVT) is a blood clot that usually forms within the deep veins of the leg, but it can occur in the veins of the arms as well as the mesenteric, thoracic, cerebral, hepatic, renal, and portal veins. The disruption of the clot through the venous circulation can cause blockage in the pulmonary vasculature, resulting in fatal pulmonary embolism (PE). DVT leading to post-thrombotic or post-phlebitis syndrome, as long-term sequelae, can cause significant morbidity to the patient. Clinical symptoms and signs of venous thrombosis are non-specific. A high index of suspicion and validated clinical prediction rules like Wells criteria for PE help in categorizing patients with pre-test probability. VTE can be a consequence of acquired risk factors, referred to as a provoked event, or lack such provoking risk factors, referred to as an unprovoked event [2]. Most Indian data on venous thrombosis originate from urban or low-altitude settings, with limited representation from hilly regions such as Himachal Pradesh. Regional variations in geography, lifestyle, and healthcare access may influence risk factors and clinical presentation. This study aims to address this gap by characterizing the clinical profile of venous thrombosis involving multiple venous sites in patients from a tertiary center in this region. D-dimer levels were analyzed as the proportion of confirmed cases showing elevation across different venous thrombosis sites. The performance of the modified Wells pre-test probability score in classifying confirmed cases of DVT and PE as likely or unlikely was evaluated [3,4].
Materials and methods
Study setting
This cross-sectional observational study was conducted in a tertiary care referral hospital in Kangra district, Himachal Pradesh, India.
Patient selection and data collection
All patients diagnosed with venous thrombosis over a one-year period (January 2019 to January 2020) fulfilling the inclusion and exclusion criteria were recruited using consecutive (total enumeration) sampling. All patients above the age of 18 years who were diagnosed with venous thrombosis of any site in medical wards and were willing to participate in this study were included. Exclusion criteria included patients younger than 18 years of age and those who declined to provide informed consent. Diagnosis was based on clinical presentation and radiological confirmation using standard imaging modalities: compression ultrasound or venous duplex sonography for upper and lower limb venous thrombosis, magnetic resonance venography for cerebral venous thrombosis (CVT), CT pulmonary angiography for pulmonary thromboembolism (PTE), and contrast-enhanced CT abdomen for abdominal or mesenteric venous thrombosis. DVT was defined by venous non-compressibility with or without intraluminal thrombus on ultrasonography; CVT by absent flow or filling defects in cerebral venous sinuses on MR venography; and PTE by intraluminal filling defects within the pulmonary arterial tree on CT pulmonary angiography. Data were collected using a structured proforma that recorded demographic variables, clinical presentation, comorbidities and predisposing risk factors, laboratory parameters including D-dimer levels, and thrombophilia evaluation where indicated, which included serum homocysteine levels, protein C and protein S activity, antithrombin III levels, antiphospholipid antibody testing, factor V Leiden mutation, and prothrombin gene mutation analysis, along with radiological findings, anatomical site of thrombosis, and final confirmed diagnosis. D-dimer levels were measured at admission using a quantitative immunoassay as part of routine laboratory evaluation. A value of ≥0.5 µg/mL was considered positive. Age-adjusted D-dimer cut-offs were not applied. D-dimer levels were analyzed descriptively as the proportion of patients with confirmed venous thrombosis who demonstrated elevated values across different thrombosis sites (DVT, PE, CVT, and other sites). Performance of pre-test probability score by modified Wells criteria in predicting cases of DVT and PE was assessed retrospectively, based solely on clinical variables documented at initial presentation and prior to radiological confirmation, to minimize information bias. A score of 2 or higher indicated that DVT was likely, while a score of less than 2 indicated that it was unlikely. A score of 4 or more indicated that PE was likely, while one of less than 4 indicated that it was unlikely [3,4].
Data analysis
Data were entered into Microsoft Excel (Redmond, WA, USA). Quantitative variables were expressed as means with standard deviations and categorical variables as frequencies and percentages. For D-dimer levels and Wells scores, results are presented as proportions with 95% confidence intervals (CIs), calculated using the Wilson method. No formal diagnostic accuracy measures requiring non-diseased controls were estimated.
Results
During the study period, 76 patients admitted with venous thrombosis were enrolled in the study. Patients’ mean age was 47.4 ± 16.3 years, and they ranged in age from 24 to 92. Of the 76 patients, 44 (57.9%) were females, and 32 (42.1%) were males. The female to male ratio was 1.3:1. The mean age of males was 46.0 ± 15.2 years, while that of females was 48.5 ± 17.1 years. The distribution of age and thromboembolism types is depicted in Table 1.
Most patients had DVT (64.5%) (n=49), followed by PTE (15.8%) (n=12) and CVT (11.8%) (n=9) either as an isolated event or in combination with other venous thrombosis. Most males had DVT (46.9%) (n=15), followed by PTE (25%) (n=8), portal venous thrombosis (PVT) + splenic venous thrombosis (SVT) (6.3%) (n=2), and CVT (6.2%) (n=2). Among females, DVT was most common (65.9%) (n=29), followed by CVT (20.6%) (n=7) and isolated PVT (6.8%) (n=3). Out of 49 patients with DVT, 48 patients had lower limb DVT (97.5%), and one had upper limb DVT (2.1%). The left lower limb was most commonly affected (75%) (n=36). Out of the 49 patients, 40 had provoked DVT (81.6%), and nine had no provoking factor (18.4%). The distribution of clinical symptoms and signs in patients with DVT is shown in Figure 1.
*Clinical presentations of deep vein thrombosis (DVT) (n=49)Values are expressed as frequency and percentage [n (%)]
The distribution of vessels involved in DVT is depicted in Table 2.
Of the 49 patients, 45 had deep sites (91.8%) and four had superficial + deep sites (8.2%). Moreover, 44 patients had proximal (89.8%), three had distal (6.1%), and two had proximal + distal (4.1%) DVT sites.
In CVT patients, the transverse sinus (44.4%) (n=4) was most involved, followed by the superior sagittal sinus (33.3%) (n=3), while four patients (44.4%) had multiple sinuses involved. The left side of the brain was involved in 66.7% (n=6), while the rest had right side involvement (33.3%) (n=3). Four of the patients (44.4%) had nonhemorrhagic infarcts. The clinical presentation of patients with CVT is shown in Table 3.
Among the 12 PTE patients, the most common clinical presentation was dyspnea (91.7%) (n=11), followed by tachycardia (91.7%) (n=11). The most common ECG finding in PTE patients was sinus tachycardia alone (41.7%) (n=5), followed by sinus tachycardia + S1Q3T3 pattern (25%) (n=3). The distribution of vessels involved in PTE is shown in Table 4.
Common predisposing factors for venous thrombosis are presented in Table 5.
Elevated D-dimer levels were observed in 91.8% (95% CI, 80.4-97.73%), 88.9% (95% CI, 51.75-99.72%), 100% (95% CI, 73.54-100%), and 81.82% (95% CI, 48.22-97.72%) of patients with DVT, CVT, PTE, and other thrombosis sites, respectively, as depicted in Table 6.
When the modified Wells scores were applied retrospectively, 46 of 49 patients with DVT (93.9%; 95% CI: 83.13-98.72%) were classified as “Likely DVT” (score ≥2), while three patients (6.1%) were classified as “Unlikely DVT”. Among the 12 patients with PTE, 11 patients (91.7%; 95% CI: 61.52-99.79%) were classified as “Likely PTE” according to the modified Wells criteria.
Discussion
VTE, comprising DVT and PE, can result in significant mortality, morbidity, and healthcare expenditure. Approximately one-third of patients with symptomatic VTE manifest as PE, whereas two-thirds manifest as DVT alone. Both DVT and PE can be clinically silent (asymptomatic) and hence may not be suspected [5]. In our study, the mean age of patients with venous thrombosis was 47.4±16.3 years; 60.5% (n=46) were aged above 40 years, 26% (n=20) were aged between 31 and 40 years, and 14% (n=10) were aged between 21 and 30 years. These data align with those of other studies [6-8]. Females predominated over males with a ratio of 1.3:1, which is in concordance with studies by Naqvi et al. and Garg et al. but differs from some Indian subgroup studies [8-10]. In our study, DVT (72.7%) (n=32/44) and CVT (77.8%) (n=7/9) were most common among females, while PTE was most common among males (75%) (n=9/12). Our findings are in concordance with Agarwal et al. and Garg et al. [10,11]. The female predominance observed in our study can be attributed to pregnancy and the postpartum period, including cases following caesarean section, a higher proportion of CVT among women, and the presence of hyperhomocysteinemia likely related to nutritional deficiencies. As this was a hospital-based study, referral patterns may also have influenced the gender distribution.
The lower limb was most commonly involved (n=48/49) (97.9%), and one patient had upper limb DVT (n=1/49) (2.1%). Among lower limb DVTs, the left lower limb (75%) (n=36) was the most common. These findings are in line with those of other Indian studies [12,13]. Virchow suggested that this disparity may be related to compression of the left common iliac vein by the right common iliac artery [14]. We observed that proximal DVT was more common, occurring in 89.7% (n=44) of patients, whereas isolated distal DVT was seen in 6.1% (n=3); an additional 4.1% (n=2) of patients had involvement of both proximal and distal veins. Limb swelling was the most common symptom (95.7%) (n=47), and the femoropopliteal vein was most commonly involved (38.8%) (n=19). These results are consistent with other Indian and Western studies [8,15-18].
Among the 76 patients with venous thrombosis, the most common predisposing factors found were as follows: smoking (33%) (n=25), followed by obesity and malignancy (21% (n=16) each), diabetes and hypertension (16% (n=13) each), hyperlipidemia and sepsis (13% (n=10) each), tuberculosis and hyperhomocysteinemia (11.8% (n=9) each), postpartum period (6.6% (n=5)), and hematological disorder, recent surgery and immobilization, connective tissue disorders, and chronic kidney disease (CKD) (5.3% (n=4) each). We observed that 26.5% (n=13/49) of DVT patients, 41.7% (n=5/12) of PTE patients, 11.1% (n=1/9) of CVT patients, and 66.7% (n=6/11) of other thromboembolism site patients were smokers. Several prospective studies have reported smoking to be an independent risk factor [19,20], whereas others have failed to detect a significant relationship between smoking and VTE. As this was a descriptive study without a control group, these findings reflect the prevalence of smoking within the cohort and do not permit inference regarding smoking as an independent risk factor for VTE. We observed that 10 patients (13.2%) with venous thrombosis had underlying sepsis. Among patients with sepsis, six had pneumonia, two had urosepsis, and two had rickettsial infections. The pneumonic illnesses included both community-acquired and hospital-acquired pneumonia. In these patients, venous thrombosis occurred in the clinical context of acute infection and hospitalization, often accompanied by factors such as immobilization, systemic inflammation, hypoxia, and dehydration. Coexisting factors such as smoking were also commonly observed, as reported in previous observational studies [21]. Given the descriptive nature of the present study, these findings do not establish independent causality. Rickettsial infection may cause a hypercoagulable state, leading to disseminated intravascular coagulation and DVT in severe infection cases during the acute phase [22]. Regarding thrombophilia profile, nine patients (11.84%) with hyperhomocysteinemia (six DVT and three CVT), two with antiphospholipid antibody syndrome (2.6%), and one with protein C deficiency were found. These data are in contrast with other studies, and the higher rate of hyperhomocysteinemia might be due to the concomitant vitamin B12 deficiency observed in our population [23].
As in other studies, none of the patients with chronic liver disease had DVT, CVT, or PTE, while chronic liver disease contributed to 22% (n=2) of mesenteric thrombosis cases. This can be attributed to the protective antithrombotic mechanisms in liver disease [24]. All five patients who had developed venous thrombosis during the postpartum period were in the first month after delivery, and all had undergone lower segment caesarean section (LSCS). It is suggested that puerperal CVT is 10-12 times more frequent in India and the predisposing factors, like anemia, increased coagulability of blood, slowing of the blood stream, and dehydration, aggravated in puerperium, contributed to the high incidence of CVT. Caesarean sections further increase the risk due to the postsurgical decline of protein C levels caused by surgically induced tissue damage. This causes activation of blood clotting with increased thrombin generation, which in turn activates protein C and promotes its clearance from the plasma [25]. Out of 16 malignancy patients (21%), 50% (n=8) had DVT, 25% (n=4) had CVT, and 12.5% (n=2) each had PTE and other VTE types.
The proportion of patients with elevated D-dimer levels among those diagnosed with DVT, PTE, and CVT, as well as the distribution of patients classified as “likely DVT” and “likely PTE” using the modified Wells criteria, was comparable to that reported in previous studies [26-28]. In this case-series, retrospective application of the modified Wells model demonstrated that most patients with confirmed DVT or PTE fell into the “likely” category; however, these findings are descriptive and do not constitute validation of diagnostic performance. Among the seven patients with D-dimer levels <0.5 µg/mL, three had DVT, one had CVT, and two had PVT. VTE can occur with a negative D-dimer concentration and related to methodological limitations. However, the lack of increase in D-dimer levels could also be caused by fibrinolysis alteration. This can also be attributed to the thrombus volume and chronicity [29].
Limitations
This was a single-center, hospital-based study, which may limit the generalizability of the findings. The sample size was modest, especially for subgroups such as CVT, PTE, and other uncommon thrombosis sites, reducing the power of subgroup analyses. The cross-sectional design precluded assessment of outcomes such as recurrence, long-term complications, and mortality. The absence of a control or non-VTE comparison group is the most significant limitation, as it precludes assessment of independent risk factors. As the study included only patients with radiologically confirmed VTE, formal diagnostic accuracy measures (specificity, false-positive rates, and predictive values) for D-dimer and Wells scores could not be assessed. The findings therefore represent the proportion of confirmed cases with elevated D-dimer levels or classified as “likely” by Wells criteria, rather than true diagnostic sensitivity in a suspected population. Well's scores were applied retrospectively, which may have introduced information bias. Thrombophilia testing was not performed uniformly in all patients; it was selectively done when no clear provoking factor was identified in order to avoid unnecessary financial burden, which may have led to underestimation of inherited or acquired prothrombotic states.
Conclusions
This study describes the clinical profile of patients admitted with venous thrombosis in the medical wards of a tertiary care hospital. Venous thrombosis was not an uncommon presentation, with most patients having isolated DVT, followed by PTE and CVT. The cohort predominantly comprised younger patients with a female preponderance. Most of the patients had isolated DVT followed by PTE and CVT. Smoking and malignancy were commonly observed among patients with venous thrombosis in this cohort. Elevated D-dimer levels and classification as “likely” by the modified Wells criteria were frequent among patients with confirmed disease, reflecting case-based positivity rather than diagnostic accuracy or validation of these tools.
Early diagnosis and treatment of VTE can essentially reduce morbidity and mortality. More prospective studies are required on this topic to draw more evidence and add to the existing data.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): the Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)Eur Heart J Konstantinides SV Meyer G Becattini C 543603412020 https://doi.org/10.1093/eurheartj/ehz 4053150442910.1093/eurheartj/ehz 405 · doi ↗ · pubmed ↗
- 2American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism Blood Adv Ortel TL Neumann I Ageno W 4693473842020 https://doi.org/10.1182/bloodadvances.20200018303300707710.1182/bloodadvances.2020001830 PMC 7556153 · doi ↗ · pubmed ↗
- 3Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis N Engl J Med Wells PS Anderson DR Rodger M 122712353492003 https://doi.org/10.1056/NEJ Moa 0231531450794810.1056/NEJ Moa 023153 · doi ↗ · pubmed ↗
- 4Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography JAMA van Belle A Büller HR Huisman MV 1721792952006 https://doi.org/10.1001/jama.295.2.1721640392910.1001/jama.295.2.172 · doi ↗ · pubmed ↗
- 5Causes of sudden unexpected death of adult hospital patients J Hosp Med Nichols L Chew B 70670872012 https://doi.org/10.1002/jhm.19802302405510.1002/jhm.1980 · doi ↗ · pubmed ↗
- 6Physician practices in the management of venous thromboembolism: a community-wide survey J Vasc Surg Anderson FA Jr Wheeler HB 707714161992 https://doi.org/10.1067/mva.1992.41080143365810.1067/mva.1992.41080 · doi ↗ · pubmed ↗
- 7Real world data on clinical profile, management and outcomes of venous thromboembolism from a tertiary care centre in India Indian Heart J Singh S Kapoor S Singh B 336341732021 https://doi.org/10.1016/j.ihj.2021.02.0063415475210.1016/j.ihj.2021.02.006PMC 8322750 · doi ↗ · pubmed ↗
- 8Analysis of patients with venous thromboembolism in a multi-specialty tertiary hospital in South India Indian J Vasc Endovasc Surg Pawar P Ayyappan MK Jagan J 293372020 https://doi.org/10.4103/ijves.ijves_31_19