Internal Hernia With Enteroenteric Fistula After Roux-en-Y Gastric Bypass in an Adult Female
Michael W Alchaer, Harrison Gorran, Stephanie Gonzalez, Koji Honda, Thomas A Abbruzzese

TL;DR
A rare case of internal hernia caused by an enteroenteric fistula after gastric bypass surgery is reported, highlighting the challenges in diagnosis and the benefits of robotic surgery.
Contribution
Reports a rare enteroenteric fistula causing internal hernia after Roux-en-Y gastric bypass in an adult.
Findings
Enteroenteric fistula after RYGB is extremely rare and can mimic internal hernias on imaging.
Robotic laparoscopy enabled successful excision and diagnosis of the fistula with rapid recovery.
Early surgical exploration is crucial for persistent obstruction despite non-diagnostic imaging.
Abstract
Internal hernia is a recognized late complication of Roux-en-Y gastric bypass (RYGB), often occurring through mesenteric defects at the jejunojejunostomy (JJ) or Petersen’s space. While most hernias result from anatomical defects, the development of an enteroenteric fistula between small-bowel limbs is exceedingly rare. Such fistulae can mimic adhesive bands or internal hernias, creating diagnostic challenges and potential delays in management. A 39-year-old woman with morbid obesity, RYGB eight years prior, and gastric pouch revision three years prior presented with severe abdominal pain, nausea, and vomiting. CT imaging showed small-bowel obstruction (SBO) with a transition point near the JJ. Repeat CT with oral contrast confirmed persistent obstruction. Emergent robotic laparoscopy identified an internal hernia caused by a short fistulous tract connecting the biliopancreatic limb to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
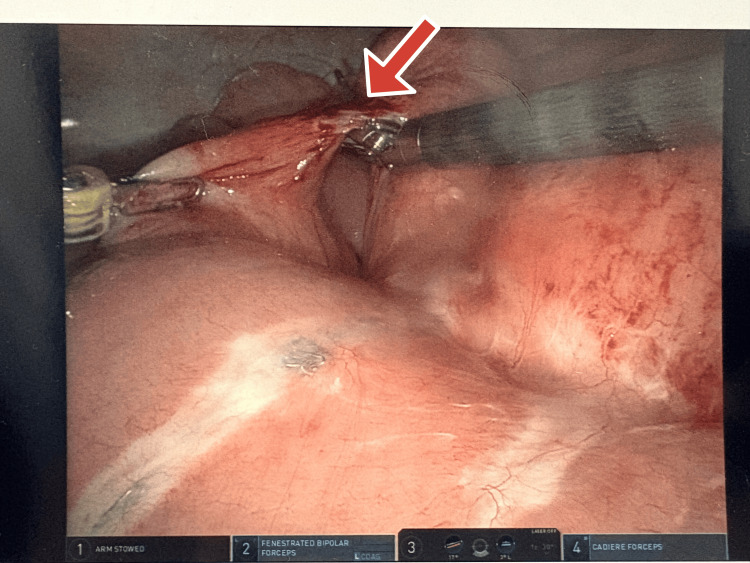 Figure 1
Figure 1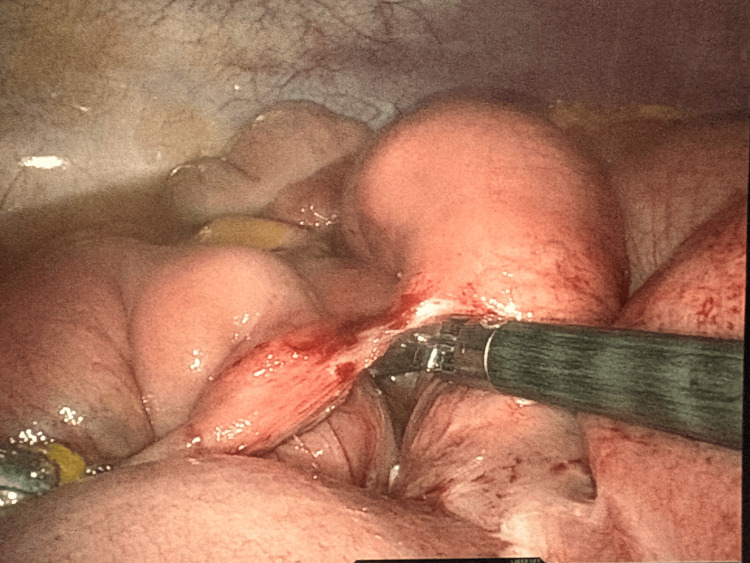 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Bariatric Surgery and Outcomes · Esophageal and GI Pathology
Introduction
Internal hernia is a well-recognized late complication of Roux-en-Y gastric bypass (RYGB), typically occurring through mesenteric defects at the jejunojejunostomy (JJ) or Petersen’s space [1,2]. Closure of these defects has been shown to reduce postoperative herniation, yet small-bowel obstruction (SBO) remains one of the most frequent delayed presentations following RYGB. In contrast, enteroenteric fistula formation between small-bowel limbs is exceedingly rare and represents an underreported etiology of obstruction [3-6]. These abnormal tracts can create inter-loop adhesions, distort normal anatomy, and mimic adhesive or internal hernia patterns, leading to diagnostic challenges [5,6]. We present a unique case of an internal hernia secondary to an enteroenteric fistula between the biliopancreatic limb and the common channel, successfully managed with a robotic-assisted approach.
Case presentation
A 39-year-old woman with morbid obesity, status post-RYGB eight years prior and gastric pouch revision three years prior, presented with one day of sharp central and upper abdominal pain associated with nausea and multiple episodes of vomiting. She was undergoing medical weight loss therapy with semaglutide.
On presentation, her vital signs were within normal limits. Physical examination revealed an obese patient with a soft, nondistended abdomen and tenderness localized to the left hemiabdomen without rebound tenderness or guarding. Laboratory evaluation, including complete blood count and metabolic panel, was within normal ranges.
Computed tomography (CT) imaging of the abdomen and pelvis demonstrated dilated small-bowel loops measuring up to 6 cm with decompressed distal bowel, a transition point near the jejunojejunal (JJ) anastomosis, and mild mesenteric stranding. A repeat CT scan with oral contrast showed persistent SBO without distal contrast passage.
Given concern for a closed-loop obstruction, the patient was taken emergently to the operating room for robotic diagnostic laparoscopy. Abdominal access was obtained via Optiview entry at Palmer’s point, with placement of two additional 8-mm robotic trocars. The small bowel was systematically examined from the terminal ileum proximally. At the level of the JJ anastomosis, a dense inter-loop adhesion with incarcerated small bowel was identified. Reduction of the herniated bowel restored distal bowel filling.
Further inspection revealed chylous ascites and active fluid oozing from a short tract, consistent with an enteroenteric fistula between the biliopancreatic limb and the common channel (Figure 1 and Figure 2). The left upper quadrant port was upsized to facilitate the use of a robotic stapler. The fistulous tract was stapled, excised, and sent for histopathologic evaluation. A Jackson-Pratt drain was placed in the left lower quadrant due to significant ascites.
Intraoperative view of the internal hernia with incarcerated small bowel.Arrow pointing at an internal hernia.
Reduction of the hernia showing viable small bowel loops.
Pathologic examination confirmed an enteroenteric fistula with focal acute inflammation. The patient recovered without complications, regained bowel function by postoperative day three, and was discharged home in stable condition on postoperative day four while tolerating a regular diet.
Discussion
Internal hernia is a well-known late complication of RYGB, most often occurring through mesenteric defects at the JJ or Petersen’s space. Closing these defects during the primary operation significantly decreases the risk of herniation [1,2]. In contrast, enteroenteric fistula formation between small-bowel limbs is exceedingly rare and represents an unusual cause of SBO. These tracts can create inter-loop adhesions, distort anatomy, and mimic adhesive or internal hernias, leading to diagnostic challenges [5,6].
Most reported post-bypass fistulae involve the gastric pouch or gastrojejunal anastomosis rather than the jejunojejunal configuration seen here [3-7]. The proposed mechanisms include chronic inflammation, localized ischemia, staple-line failure, or prior revisional surgery [3,4]. In this patient, previous pouch revision likely contributed to localized inflammation and subsequent fistula formation between the biliopancreatic limb and the common channel.
CT imaging remains the main diagnostic tool for SBO after RYGB, but short fistulous tracts are often undetectable even with oral contrast [2,8-11]. Persistent obstruction despite non-diagnostic imaging should prompt early surgical exploration [4,8]. Minimally invasive approaches, particularly robotic surgery, enable comprehensive inspection of mesenteric defects and precise management of rare findings such as fistulae [1].
This case emphasizes that an enteroenteric fistula should remain in the differential diagnosis for obstruction following RYGB [3-6]. Prompt recognition and minimally invasive repair can achieve excellent outcomes while preserving bowel integrity [1,9,12].
Conclusions
Internal hernia secondary to an enteroenteric fistula is an exceptionally rare cause of SBO after RYGB. Surgeons should maintain a high index of suspicion in post-bariatric patients presenting with unexplained obstruction, even when imaging is inconclusive. Early recognition and minimally invasive repair, particularly with robotic assistance, can lead to excellent outcomes while preserving bowel integrity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevention and management of internal hernias after bariatric surgery: an expert review Mini-Invasive Surg Pokala B Giannopoulos S Stefanidis D 2362022
- 2Petersen's space hernia as a complication of gastric bypass surgery: a case report J Surg Case Rep Palacios MF Guachilema Ribadeneira AP Yepez J Cisneros AL Imbacuan SM Verboonen S 02025202510.1093/jscr/rjae 504PMC 1182648139958681 · doi ↗ · pubmed ↗
- 3S 3891 from Roux-en-Y to Roux-en-why: colonic enteric fistula - a rare complication of Roux-en-Y gastric bypass Off J Am Coll Gastroenterol ACG Patel S Chen B West S 24841182023
- 4Spontaneous gastrojejunal fistulization after Roux-en-Y bypass surgery: a case report and review of literature Cureus Lopez Luciano MJ Then EO Brana CJ Ofosu A Gaduputi V 011201910.7759/cureus.5035 PMC 672186831501727 · doi ↗ · pubmed ↗
- 5Acute perforation in a gastrojejunocolic fistula after a laparascopic Roux-en-Y gastric bypass: case report Surg Case Rep Velleman J Masereel B Geyskens P 41920233693994910.1186/s 40792-023-01620-z PMC 10027975 · doi ↗ · pubmed ↗
- 6S 3004 the fear of obese man: a case of gastrocolic fistula following Roux-en-Y gastric bypass Off J Am Coll Gastroenterol ACG Yoo BS Marcuard M Parekh PJ 15831152020
- 7Gastrojejunocolic fistula: case report of a rare late complication of laparoscopic Roux-en-Y gastric bypass and review of the literature Int J Surg Case Rep Gehle DB Pullatt RC Elias PS 1061528420213428097010.1016/j.ijscr.2021.106152 PMC 8274295 · doi ↗ · pubmed ↗
- 8Gastrocolic fistula in Crohn's disease detected by oral agent contrast-enhanced ultrasound: a case report of a novel ultrasound modality World J Gastroenterol Wu S Zhuang H Zhao JY Wang YF 211921252620203253677910.3748/wjg.v 26.i 17.2119 PMC 7267691 · doi ↗ · pubmed ↗