Incidence, risk factors and prevention of hypothyroidism following laryngectomy: a systematic review and meta-analysis
JY Tan, E Westwood, O Edafe

TL;DR
About half of patients who undergo laryngectomy develop hypothyroidism, with risk factors like hemithyroidectomy and radiotherapy identified.
Contribution
This study provides a systematic review and meta-analysis to quantify hypothyroidism risk and suggest preventative strategies after laryngectomy.
Findings
The overall incidence of hypothyroidism after laryngectomy is 50%.
Hemithyroidectomy, radiotherapy, and neck dissection are significant risk factors.
Preventative measures include preserving thyroid blood supply and monitoring thyroid function.
Abstract
Hypothyroidism following laryngectomy is a well-recognised complication. The symptoms are multisystemic and can cause significant morbidity in patients. We aim to characterise the incidence of hypothyroidism following laryngectomy, and identify risk factors and preventative measures. A systematic search of EMBASE and PubMed was performed. We appraised relevant articles as per the predefined eligibility criteria. A quality assessment of the included studies was done. A meta-analysis was performed to evaluate the association between reported risk factors and hypothyroidism. Forty articles were included. This encompassed a total of 3,061 patients with a median age of 61 years. Overall incidence of hypothyroidism was 50% (interquartile range: 38.3–75.7). The following factors were significantly associated with hypothyroidism: hemithyroidectomy, odds ratio (OR) 4.84 (95% confidence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
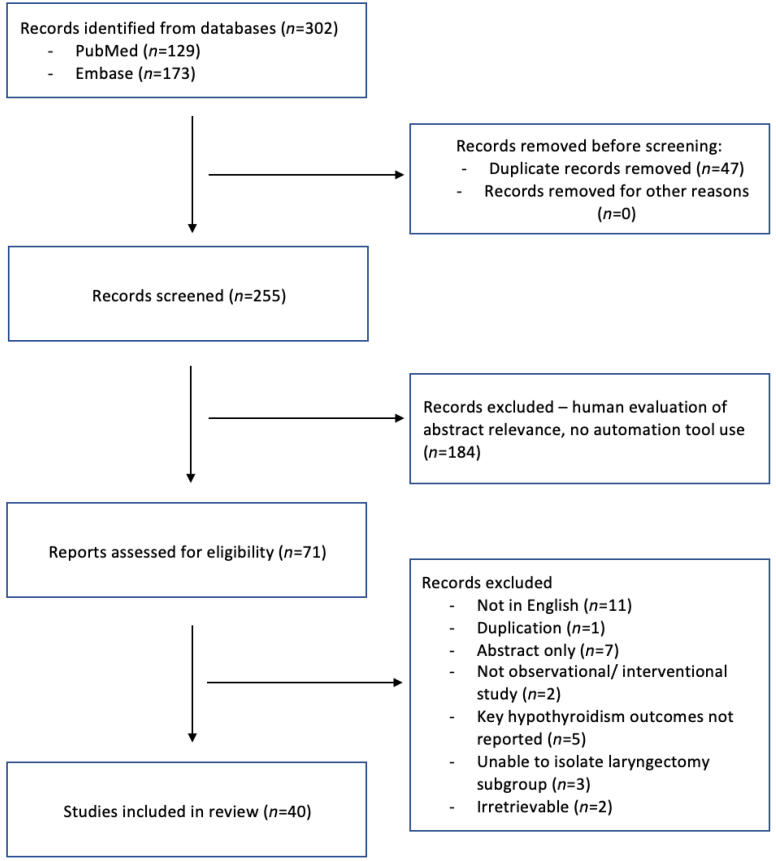 Figure 1
Figure 1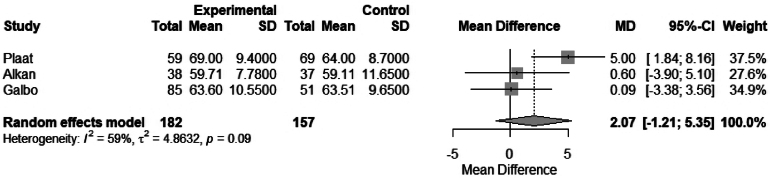 Figure 2
Figure 2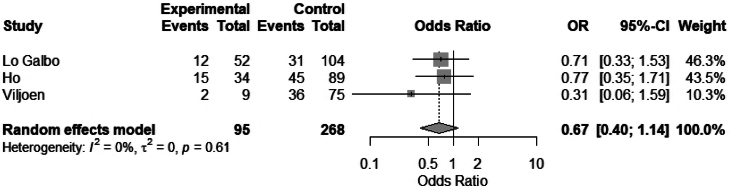 Figure 3
Figure 3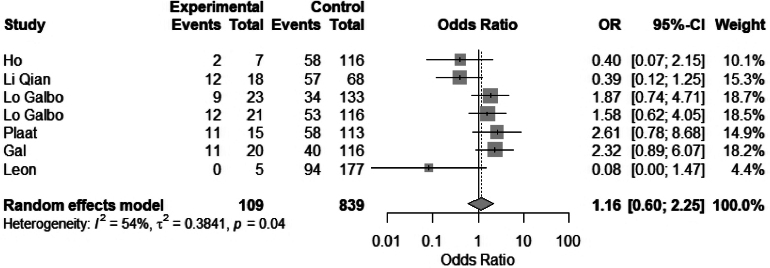 Figure 4
Figure 4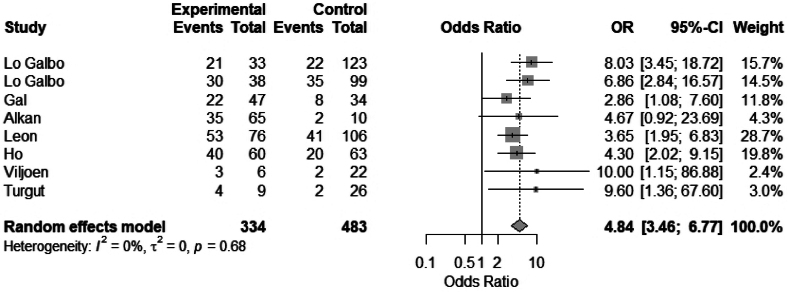 Figure 5
Figure 5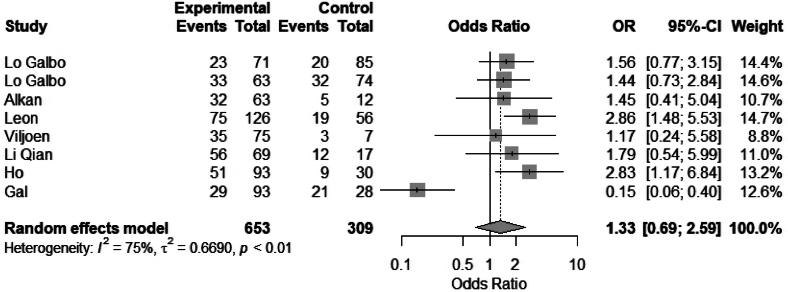 Figure 6
Figure 6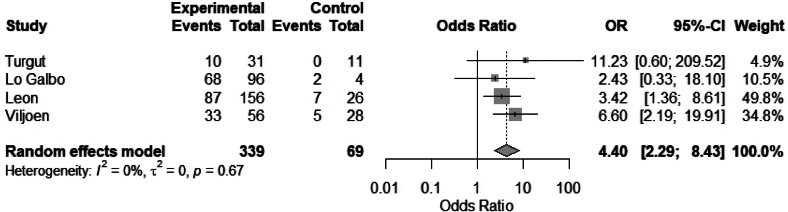 Figure 7
Figure 7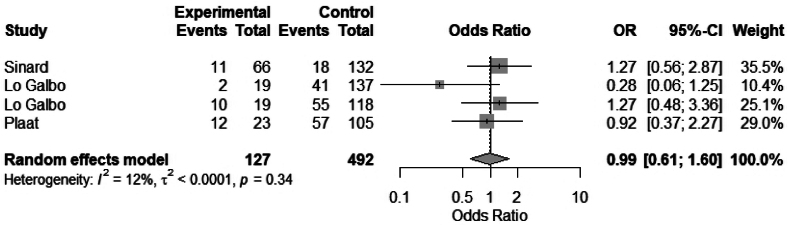 Figure 8
Figure 8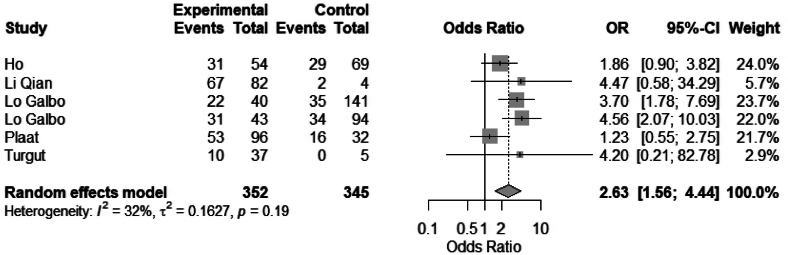 Figure 9
Figure 9| Median age, years | 61 |
| Male to female ratio | 87:13 |
| Patients on adjuvant or neoadjuvant radiotherapy, | 1,766 (63) |
| Primary treatment | 1,252 patients |
| Salvage treatment | 813 patients |
| Extent of thyroid dissections, | |
| Hemithyroidectomy | 1,418 (52) |
| Total thyroidectomy | 425 (15) |
| No thyroid dissection | 897 (33) |
| Risk factors | Reduced risk | No risk | Increased risk |
|---|---|---|---|
| Older patients | Plaat | Alkan | Lo Galbo |
| Female | Ho | Gal | |
| Advanced tumours | Lo Galbo | Ho | |
| Hemithyroidectomy | Lo Galbo | Ho | |
| Radiotherapy | Turgut | Sinard | |
| Chemotherapy | Sinard | ||
| Neck Dissection | Ho | Lo Galbo |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVoice and Speech Disorders · Thyroid Cancer Diagnosis and Treatment · Thyroid and Parathyroid Surgery
Introduction
Hypothyroidism is a well-recognised complication of laryngectomy; however, reported incidence varies.^1–5^ The extent of thyroid dissection and the requirement for multimodal treatment regimens including radiotherapy differ between patients, and have long been linked with this variance. Several demographic factors such an age and sex are also considered influential.^6,7^ Hypothyroidism itself can be broadly divided into overt hypothyroidism and subclinical hypothyroidism. Both are defined, investigated and managed in several ways, adding further to heterogeneity in the literature.
Symptoms of hypothyroidism are insidious and multisystemic, resulting in significant morbidity for the patient. Classic features include fatigue, cold intolerance, weight gain, constipation and dry skin, but the signs and symptoms are non-specific.^8^ In the postoperative context, hypothyroidism is associated with poor wound healing, complications such as salivary fistula formation, cardiac morbidity and depression.^9^ Mechanisms of developing postoperative hypothyroidism include concomitant thyroidectomy, iatrogenic injuries or sacrificed blood vessels of the thyroid gland during surgery. Both preoperative and postoperative neck radiation may also play a role in the development of hypothyroidism, likely confounded by advanced disease and the extent of surgical treatment.^6,10^
We aim to characterise the incidence of hypothyroidism following laryngectomy, and identify risk factors and preventative measures.
Methods
We included all observational or interventional studies that evaluated the incidence, risk or prevention of hypothyroidism following laryngectomy. We excluded articles with fewer than ten patients, case reports, reviews, commentaries and articles not available in the English language.
A systematic literature search of EMBASE and PubMed was undertaken to publication date (8 August 2023). We restricted the search to articles available in the English language. We used the following search strategy: (thyroid replacement OR underactive thyroid OR hypothyroid OR hypothyroidism OR thyroid hormone OR thyroxine OR levothyroxine) AND (laryngectomy OR pharyngolaryngectomy). A further search update was done post analysis on 18 December 2024, and one article met our criteria as stated; the findings are presented in the discussion.
Two authors (EW and OE) screened titles and abstracts according to the eligibility criteria. Any query over the selection process was discussed between the two authors (EW and OE).
One author (EW) independently evaluated texts using a standardised data collection proforma. All extracted data were checked for accuracy by another author (JYT). Any discrepancies were discussed and amended accordingly.
The following data were collected in individual studies: study characteristics and population; extent of surgery; radiotherapy; definition of hypothyroidism; rates, risk factors and prevention of hypothyroidism. Participant demographics and underlying pathology, the extent of dissections performed and the use of any additional treatment modalities were recorded.
Murad’s tool was used to assess the quality of the included single-arm observational studies (Appendix 1 – available online).^11^ Cochrane collaboration’s tool was used to assess risk of bias in randomised controlled trials (Appendix 2 – available online).^12^
Statistical analysis
Meta-analysis was done to evaluate the association between reported risk factors and hypothyroidism where complete data were available. A random effect model was used because of the variability in definitions, disease and treatment extent across studies. The I^2^ statistic was used to evaluate the degree of heterogeneity in the meta-analysis. RStudio with meta package was used to perform the meta-analysis. Forest plots for the individual risk factors are included in this review. Summary statistics of categorical variables were summarised as count and percentages. The median age (interquartile range [IQR]) of the review population was calculated. Where possible, rates of hypothyroidism were calculated and summarised across studies.
Because the review was based on previously published studies, no ethical approval or patient consent were required.
Results
Forty studies were included in this review. Figure 1 shows the PRISMA flow chart outlining the search strategy used for this systematic review. The study designs were as follows: retrospective, 26; prospective, 13; randomised controlled trial, 1. The median (IQR) quality score of observational studies included was 3 (2–3). The one randomised controlled trial showed a high risk of bias on assessment with the Cochrane risk of bias tool for randomised controlled trials. The systematic review’s objectives were studied as the primary outcome in 29 studies and as the secondary outcome in 11 studies.
PRISMA flow chart outlining search strategy used for this systematic review
The systematic review included a total of 3,061 patients who had total laryngectomy. In total, 20 of 40 studies established thyroid status preoperatively. A definition of hypothyroidism using thyroid-stimulating hormone (TSH) or free T4 (fT4) measurements was reported in 29 studies; 11 studies did not record TSH or free T4 measurements.
Table 1 shows the demographics of patients in the review population and treatment details.
Incidence
The median (IQR) reported incidence of hypothyroidism was 50% (38.3–75.7). The median incidence of subclinical and clinical hypothyroidism across all studies was 27% (range 10–54%) and 24% (range 3.3–64.7%), respectively.
Risk factors
Nineteen studies evaluated the risk factors of hypothyroidism following laryngectomy. The risk factors evaluated were age and sex, hemithyroidectomy or total thyroidectomy, tumour stage, radiotherapy, chemotherapy and neck dissection. Table 2 shows risk factors evaluated for their association with postoperative hypothyroidism. A meta-analysis was carried out to evaluate the association between reported risk factors and hypothyroidism following laryngectomy.
Demographic factors
The association of hypothyroidism and age was assessed in 11 studies. Of these, three studies had complete data to perform a meta-analysis to evaluate the mean difference in age between euthyroid and hypothyroid patients. No association was found between age and hypothyroidism: mean difference 2.0 (95% CI −1.21 to 5.35), I^2^ = 59.3% (Figure 2). Three studies stratified patients by age >70 years, and no significant difference was found in the meta-analysis: odds ratio (OR) 0.67 (95% CI 0.40 to 1.14), I^2^ = 0.0% (Figure 3).
Meta-analysis comparing mean difference in age between euthyroid and hypothyroid patients
Meta-analysis of age over 70 vs age under 70
Sex as a risk factor for hypothyroidism following laryngectomy was evaluated by 11 studies. Seven studies were included in a meta-analysis for sex. No statistically significant difference was found between females and males: OR 1.1 (95% CI 0.6 to 2.25), I^2^ = 52 (Figure 4). Gal et al found that being female was associated with hypothyroidism and suggested that the relationship between female sex and hypothyroidism could be due to the effect of oestrogen supplements and the risk of subclinical Hashimoto’s thyroiditis in females.^6^ Léon et al found a significant difference between females and the development of hypothyroidism in univariate analysis only, possibly because of the increased incidence of thyroid diseases in females.^13^
Meta-analysis of female vs male
Thyroidectomy
Eleven studies evaluated the association between hemithyroidectomy and hypothyroidism. A total of eight studies were included in a meta-analysis. Hemithyroidectomy was significantly associated with hypothyroidism following laryngectomy: OR 4.84 (95% CI 3.46 to 6.77), I^2^ = 0% (Figure 5). Of the 11 studies, 9 showed a significantly increased risk of hypothyroidism in patients who had concomitant hemithyroidectomy.^4,5,7,10,13–17^
Meta-analysis of hemithyroidectomy vs no thyroidectomy
Tumour stage
Eight studies were included in a meta-analysis to compare the association between early (T1, T2) vs advance tumour stage (T3, T4) and hypothyroidism. No significant difference was found in the meta-analysis: OR 1.33 (95% CI 0.69 to 2.59), I^2^ = 75% (Figure 6). Three multivariate analyses reported significantly increased rates of hypothyroidism in more advanced tumours.^4,18,19^ Rosko et al reported a relative risk of 3.2 for patients with advanced-stage disease (stage 3 or 4) compared with early-stage disease (stage 1 or 2) (95% CI 1.4 to 7.3, p = 0.005).^19^ However, nine studies reported no significant difference for stage as a risk factor.^5,10,13,14,16,20–23^ In a multivariate study, Gal et al reported that thyroid gland invasion by the tumour increased risk of hypothyroidism.^6^
Meta-analysis of early stage vs advanced stage
Radiotherapy
Nine studies evaluated the association between radiotherapy and hypothyroidism; four studies were eligible to be included in the meta-analysis. We found that radiotherapy was significantly associated with hypothyroidism: OR 4.4 (95% CI 2.29 to 8.43), I^2^ = 0% (Figure 7). Radiotherapy was identified as having significant associations with hypothyroidism in six studies.^3,10,13,16,23,24^ Three other studies showed no significant difference in radiotherapy treatment.^17,20,21^ Gal et al reported that preoperative radiotherapy was associated with a 2.76-fold relative risk (p < 0.01) of developing hypothyroidism compared with no radiotherapy, whereas postoperative radiotherapy was associated with a 0.92-fold relative risk (p = 0.72). Plaat et al found that postoperative radiotherapy alone was associated with a lower risk of developing hypothyroidism (hazard ratio 0.49 [95% CI: 0.28–0.86]) when compared with salvage total laryngectomy after radiotherapy.^7^ Two studies reported a significant dose-dependent relationship between radiotherapy and hypothyroidism.^5,14^
Meta-analysis of radiotherapy vs no radiotherapy
Chemotherapy
Four studies were included in a meta-analysis to evaluate the association between chemotherapy and hypothyroidism. We found no statistically significant difference: OR 0.9 (95% CI 0.61 to 1.60), I^2^ = 12% (Figure 8). No studies found a statistically significant association with chemotherapy in their individual analysis.^3,5,7,10,13,19–21^
Meta-analysis of chemotherapy vs no chemotherapy
Neck dissection
Eight studies evaluated the association between neck dissection and hypothyroidism.^3–5,7,10,17,20,21^ Seven of these studies were evaluated in a meta-analysis. Neck dissection was significantly associated with hypothyroidism: OR 2.63 (95% CI 1.56 to 4.44), I^2^ = 32 (Figure 9). Multivariate analysis by Lo Galbo et al showed a statistical significance (p = 0.003) that was applicable to both ipsilateral and bilateral neck dissections.^10^ Four studies looked specifically at pretracheal or level VI dissection and risk of hypothyroidism.^10,17,19,21^ Lo Galbo et al found that paratracheal lymph node dissection was a predictive factor for developing hypothyroidism (p < 0.017).^10^ Univariate regression analysis by Turgut et al showed that the risk for hypothyroidism was 31 times higher with level VI dissection (p < 0.004) (no confidence interval was stated).
Meta-analysis of neck dissection vs no neck dissection
Prevention
Three studies referred to establishing prevention measures in their stated aims. These studies focused primarily on a demonstration of reduced hypothyroidism without impaired oncologic control when thyroidectomy is targeted to select patient groups rather than applied empirically.^16,25,26^
Primary measures of restricted thyroid dissection in selected cases were advocated in nine studies; preserving the thyroid gland where possible to reduce the risk of hypothyroidism.^15,16,26–32^ El-Sebai Ali et al reported no difference in local recurrence rates between patients who had preservation of the thyroid gland and those who did not.^15^ Hemithyroidectomy is recommended in selected cases of subglottic tumours, extra-laryngeal tumours, direct invasion of the thyroid gland, paratracheal nodal metastases and invasion of the paraglottic space.^15,16,26–32^ Attention to preservation of the blood supply to the thyroid gland is recommended as a preventative measure during dissection of contralateral lobe.^1,3,25^
The main secondary prevention recommendation was advocating preoperative (n = 4)^6,10,20,24^ and/or postoperative (n = 25) thyroid function test (TFT) monitoring. Several studies justified this further, with recommendations of monitoring postoperative TFTs in all treatment modalities.^2,28^ Others recommended monitoring only for patients who underwent combined surgery and radiotherapy or for patients receiving postoperative radiotherapy.^18,33,34,35^ Life-long surveillance of thyroid function was recommended in patients who had any treatment for hypopharyngeal or laryngeal cancer.^17^ The frequency and duration of the suggested surveillance varied.
Ten studies advised treatment of all forms of hypothyroidism.^10,13,17,18,24,25,33–36^ Some suggested empirical prescription of levothyroxine in patients with high risk factors, following laryngectomy, pharyngo-laryngo-oesophagectomy with chemoradiotherapy, or total laryngectomy with thyroid lobectomy and radiotherapy.^3,6,20,37^ Saito et al suggested empirical treatment for patients who underwent postoperative radiotherapy to prevent symptomatic endocrine complications.^37^ These studies did not specify the duration of routine thyroxine treatment or assess the long-term outcomes of patients on this treatment.
Discussion
This systematic review and meta-analysis aim to evaluate the incidence of hypothyroidism following laryngectomy, and identify risk factors and preventative measures. Our study of 40 articles showed an overall incidence of hypothyroidism of 50% (38.3–75.7). From our meta-analysis, the following risk factors were significantly associated with hypothyroidism following laryngectomy: hemithyroidectomy, OR 4.84 (95% CI 3.46 to 6.77); radiotherapy, OR 4.4 (95% CI 2.29 to 8.43); and neck dissection, OR 2.63 (95% CI 1.56 to 4.44). The preventative strategies of hypothyroidism observed in our study included restricted thyroid dissection in selected cases, preservation of blood supply to the thyroid gland during dissection, preoperative TFTs and postoperative TFT monitoring, including in those with subclinical hypothyroidism.^1,3,15,16,25–32,^
The updated search retrieved the study by Nasser et al, which reported hypothyroidism in 45% of patients following total laryngectomy,^38^ comparable with our findings. The Nasser et al study also showed a significant association between adjuvant radiotherapy (p = 0.001) and central neck dissection (p = 0.007) with the development of postoperative hypothyroidism.
This systematic review confirmed variability in the reported incidence of hypothyroidism after laryngectomy, with heterogeneity noted in patient characteristics and treatment modalities. Definitions of hypothyroidism varied between the 40 studies. Half of the reports used both TSH and fT4 levels. Nine studies used only TSH levels.^2,3,7,15,18,19,27,37,39^ Eleven studies reported rates of hypothyroidism without defining levels that meet the diagnosis of hypothyroidism.^1,6,26,28–32,40–42^ The wide incidence range for hypothyroidism of 38.3–75.7% is likely attributed to variability in the definition used and surgical extent. Timings of ascertainment of hypothyroidism and the length of follow-up were also variable or not reported in the studies.
The British Thyroid Association defined overt primary hypothyroidism as TSH ≥ 10mU/L with fT4 levels below the reference range, whereas subclinical hypothyroidism was defined as TSH of 5–10mU/, but fT4 levels in the reference range.^43^ Standardising the definition of clinical hypothyroidism and subclinical hypothyroidism is important to allow appropriate comparisons and summation of outcomes.
We would recommend increasing the number of high-quality studies aiming to formally assess the efficacy of prevention measures, such as the timing and targeting of postoperative testing or the effects of thyroid replacement on patient outcomes.
From our review, it is evident that the treatment of subclinical hypothyroidism is variable between these studies. A systematic review reported no improvement in survival or cardiovascular morbidity following levothyroxine replacement therapy for asymptomatic subclinical hypothyroidism.^44^ Although this was acknowledged by Lo Galbo et al, the study recommended screening for hypothyroidism with subsequent treatment if indicated owing to the low burden of this therapy.^10^
We recommend that patients should be monitored for hypothyroidism annually during long-term follow-up to prevent the progression to overt hypothyroidism. In patients treated with external radiotherapy, TFT should be performed every 12 months, because subclinical hypothyroidism can be present for many years before developing into overt hypothyroidism.^45^
Initial timing of the ascertainment of hypothyroidism is important because measurement in the early postoperative period may not reflect true hypothyroidism. The gold standard measure is free T4 measurements to ascertain hypothyroidism because TSH is influenced by a range of medical factors. As recommended by the British Thyroid Association report, where a diagnosis of overt hypothyroidism cannot be confirmed, clinicians should trial without levothyroxine with a repeat serum TSH after 6 weeks. Emphasis should be made to check TFTs following discharge from hospital to prevent undiagnosed overt or subclinical hypothyroidism.^43^
Management of primary hypothyroidism by the British Thyroid Association states that synthetic levothyroxine is the treatment of choice in hypothyroidism. TSH levels should be monitored 6–8 weekly with dose adjusted accordingly. Following stabilisation of TSH levels, this can be checked 4–6 monthly, and then annually.^46^
The evidence base underpinning the timing and efficacy of postoperative testing of hypothyroidism and any subsequent treatment is lacking despite this being common practice in most reporting institutions. A standardised protocol for the identification, prevention and treatment, and follow-up of hypothyroidism specifically in laryngectomy patients is recommended.
Study limitations
Limitations of this systematic review include the heterogeneity of the study population with regards to disease extent and treatment modalities. Furthermore, some studies did not exclude preoperative hypothyroidism, and thus reported rates of hypothyroidism post laryngectomy may be overestimated. From our quality assessment, 39 of the 40 studies were observational with low to moderate quality. There was only one randomised controlled trial.^15^ In addition, we excluded articles not available in the English language because formal translation and analysis was beyond the scope of this review.
Conclusions
Our systematic review of 40 studies showed that a significant proportion of patients develop hypothyroidism following laryngectomy. Commonly recognised risk factors of developing hypothyroidism are hemithyroidectomy, radiotherapy and neck dissection. This review shows the lack of data on preventative measures. Utilising these known risk factors may direct a consensus to prevent and manage hypothyroidism. Further well-designed multicentre observational studies are needed to design a protocol for managing hypothyroidism following laryngectomy.
Author contributions
Conceptualisation and methodology, EW and OE; literature search, EW; data entry and analyses, JYT and EW; original drafting of manuscript, JYT; review and revision of manuscript, JYT and OE. All authors have read and agreed to the published version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Palmer BV, Gaggar N, Shaw HJ. Thyroid function after radiotherapy and laryngectomy for carcinoma of the larynx. Head Neck Surg 1981; 4: 13–15.7287444 10.1002/hed.2890040105 · doi ↗ · pubmed ↗
- 2Buisset E, Leclerc L, Lefebvre JL et al. Hypothyroidism following combined treatment for hypopharyngeal and laryngeal carcinoma. Am J Surg 1991; 162: 345–347.1951886 10.1016/0002-9610(91)90145-4 · doi ↗ · pubmed ↗
- 3Sinard RJ, Tobin EJ, Mazzaferri EL et al. Hypothyroidism after treatment for nonthyroid head and neck cancer. Arch Otolaryngol Head Neck Surg 2000; 126: 652–657.10807335 10.1001/archotol.126.5.652 · doi ↗ · pubmed ↗
- 4Ho AC, Ho WK, Lam PK et al. Thyroid dysfunction in laryngectomees–10 years after treatment. Head Neck 2008; 30: 336–340.17636544 10.1002/hed.20693 · doi ↗ · pubmed ↗
- 5Lo Galbo AM, de Bree R, Kuik DJ et al. The prevalence of hypothyroidism after treatment for laryngeal and hypopharyngeal carcinomas: are autoantibodies of influence? Acta Otolaryngol 2007; 127: 312–317.17364370 10.1080/00016480600818096 · doi ↗ · pubmed ↗
- 6Gal RL, Gal TJ, Klotch DW, Cantor AB. Risk factors associated with hypothyroidism after laryngectomy. Otolaryngol Head Neck Surg 2000; 123: 211–217.10964293 10.1067/mhn.2000.107528 · doi ↗ · pubmed ↗
- 7Plaat RE, van Dijk BAC, Muller Kobold AC et al. Onset of hypothyroidism after total laryngectomy: effects of thyroid gland surgery and preoperative and postoperative radiotherapy. Head Neck 2020; 42: 636–644.31833166 10.1002/hed.26048 PMC 7154538 · doi ↗ · pubmed ↗
- 8Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet 2017; 390: 1550–1562.28336049 10.1016/S 0140-6736(17)30703-1PMC 6619426 · doi ↗ · pubmed ↗