A Rare but Critical Presentation in Primary Care: A Case Report on Unilateral Ureterolithiasis Leading to Postrenal Acute Kidney Injury
Melis Dorter, Ahmad Eid, Naela Darwish Saad

TL;DR
A 4 mm kidney stone in a healthy man caused severe kidney damage, showing that even small stones can lead to serious complications if not monitored.
Contribution
Highlights the rare but critical risk of postrenal acute kidney injury from small distal ureteral stones.
Findings
A 4 mm distal ureteral stone led to postrenal acute kidney injury despite initial conservative management.
Urgent stent placement resolved obstruction and restored kidney function within four days.
Persistent symptoms and clinical deterioration necessitate timely reassessment and repeat imaging.
Abstract
Distal ureteral calculi measuring ≤5 mm are generally expected to pass spontaneously and are commonly managed conservatively. However, persistent obstruction may occur and can result in renal impairment. A 31-year-old previously healthy male presented with lower abdominal discomfort, dysuria, and penile pain. Initial noncontrast computed tomography (CT) revealed a 4 mm calculus at the left ureterovesical junction without hydronephrosis. He was discharged with conservative management, including nonsteroidal anti-inflammatory drugs (NSAIDs), oral cefixime 400 mg daily, hydration advice, and follow-up instructions. Ten days later, he re-presented with severe flank pain and reduced urine output. Laboratory evaluation demonstrated elevated serum creatinine consistent with acute kidney injury (AKI). Repeat CT showed the persistent distal ureteral stone with new hydronephrosis and periureteric…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
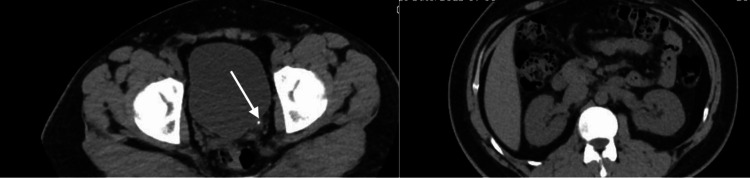 Figure 1
Figure 1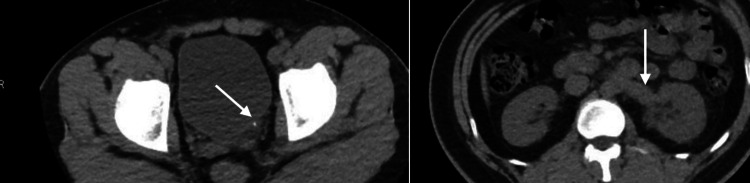 Figure 2
Figure 2| Parameter | Reference range | Initial presentation | 10-day re-presentation |
|---|---|---|---|
| White blood cell count (×10⁹/L) | 4.0-10.0 | 12.2 | 13.2 |
| Hemoglobin (g/dL) | 13-17 | 14.1 | Not repeated |
| Serum creatinine (µmol/L) | 60-110 | 82 | 144 |
| eGFR (mL/min/1.73 m²) | >90 | >90 | 55 |
| Urinalysis | - | Microscopic hematuria | Not documented |
| Time point | Clinical status | Serum creatinine (µmol/L) | Imaging findings | Management |
|---|---|---|---|---|
| Day 0 | Initial presentation | 82 | 4 mm left UVJ stone, no hydronephrosis | NSAIDs, oral cefixime, hydration |
| Day 10 | Re-presentation with reduced urine output | 144 | Persistent stone | Urgent referral to ED |
| Day 10 | Hospital admission | 144 | Mild–moderate hydronephrosis | Double-J stent placement |
| Day 14 | Poststent recovery | 85 | Not repeated | Clinical improvement |
| 4-week follow-up | Outpatient review | Normal | Not indicated | Planned definitive management |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Ureteral procedures and complications · Muscle and Compartmental Disorders
Introduction
Urolithiasis is a common condition worldwide, with a lifetime prevalence estimated at approximately 12% in men and 6% in women [1,2]. Recurrence rates approach 50% within 10 years [1]. Established risk factors include male sex, increasing age, obesity, metabolic syndrome, dehydration, and dietary factors [1,3].
Small ureteral calculi, defined as stones measuring ≤5 mm in maximal diameter, are generally expected to pass spontaneously without intervention [2,3]. Reported spontaneous passage rates for distal ureteral stones of this size range from 90% to 98% [3-5]. Consequently, conservative management with analgesia and observation is recommended in clinically stable patients without infection, refractory pain, or renal impairment [4,5].
Despite these expectations, stone size alone does not reliably predict outcome. Factors such as impaction, duration of obstruction, and anatomical location may contribute to persistent obstruction and renal dysfunction [3,5]. Postrenal acute kidney injury (AKI) is most commonly associated with bilateral obstruction or obstruction in a solitary functioning kidney [6]. However, case reports have described complications arising from small distal ureteral stones, including spontaneous forniceal rupture and ureteral perforation [7-9]. Significant renal impairment secondary to unilateral distal obstruction is less frequently reported, and when present, typically involves delayed recognition or prolonged obstruction. This case describes delayed postrenal AKI caused by a small distal ureteral stone despite initially reassuring imaging findings, underscoring the importance of vigilant follow-up and reassessment when symptoms persist.
Case presentation
A 31-year-old South Asian male with no significant past medical history presented to a primary care clinic with a three-day history of lower abdominal discomfort, dysuria, and prominent penile pain. He denied fever, nausea, vomiting, gross hematuria, or urinary retention. There was no known history of nephrolithiasis, chronic kidney disease, diabetes, hypertension, or recent dehydration.
Vital signs were stable: blood pressure, 116/75 mmHg; heart rate, 72 beats per minute; respiratory rate, 17 breaths per minute; temperature, 36.7°C; and oxygen saturation, 100% on room air. Clinical examination revealed mild left flank tenderness without abdominal guarding.
Laboratory evaluation demonstrated a white blood cell count of 12.2 × 10⁹/L and serum creatinine of 82 µmol/L (estimated glomerular filtration rate (eGFR) >90 mL/min/1.73 m²), confirming normal baseline renal function. Urinalysis showed microscopic hematuria without nitrites or leukocyte esterase. There was no laboratory evidence of urinary tract infection (UTI).
Noncontrast computed tomography (CT) of the urinary tract revealed a 4 mm calculus at the left ureterovesical junction (UVJ) without hydronephrosis and with normal contralateral renal appearance (Figure 1). No cortical thinning or delayed excretion was noted.
Noncontrast computed tomography of the urinary tract demonstrating a 4 mm calculus at the left ureterovesical junction (arrow), without hydronephrosis
Given the small stone size (≤5 mm) and the absence of hydronephrosis or renal impairment, conservative management was initiated. The patient was discharged with oral nonsteroidal anti-inflammatory drugs (NSAIDs) for analgesia, oral cefixime 400 mg daily, hydration advice, and instructions for reassessment if symptoms worsened or urine output decreased.
Ten days later, the patient re-presented with severe left flank pain and reduced urine output, which he described as decreased frequency and volume compared to baseline. He remained hemodynamically stable without signs of hypovolemia.
Repeat laboratory testing demonstrated leukocytosis (13.2 × 10⁹/L) and an elevated serum creatinine of 144 µmol/L (eGFR: 55 mL/min/1.73 m²), meeting criteria for AKI. Electrolytes were within normal limits, and he did not require hemodialysis. No alternative nephrotoxic exposures beyond prescribed NSAIDs were identified.
Given persistent symptoms and renal deterioration, he was urgently referred to the emergency department and admitted under the urology service. Repeat CT demonstrated the persistent 4 mm distal ureteral stone with new mild-to-moderate left hydronephrosis and periureteric fat stranding (Figure 2). The contralateral kidney remained normal.
Repeat noncontrast computed tomography performed 10 days later showing the same 4 mm calculus at the left ureterovesical junction (arrow), now with left-sided hydronephrosis and periureteric fat stranding
The patient underwent cystoscopic placement of a double-J ureteral stent under general anesthesia for urinary decompression. Following the intervention, urine output improved, and flank pain resolved. Serum creatinine progressively normalized, returning to baseline (85 µmol/L) by postoperative day four.
He was discharged hemodynamically stable, pain-free, and with normalized renal function. Follow-up at four weeks confirmed preserved renal function and planned definitive stone management. The clinical timeline and laboratory progression are summarized in Tables 1-2.
Discussion
Distal ureteral stones measuring ≤5 mm are widely regarded as low-risk lesions due to high spontaneous passage rates [3-5]. Conservative management is therefore considered appropriate in carefully selected patients [4,5]. However, persistent obstruction may occur despite a small stone size. The pathophysiology of obstructive nephropathy involves elevated intratubular pressure, decreased renal perfusion, and inflammatory injury, which may lead to progressive renal dysfunction if obstruction is not relieved [6]. Although postrenal AKI most commonly results from bilateral obstruction or obstruction in a solitary kidney [6], unilateral obstruction can impair renal function when prolonged or associated with significant intrarenal pressure changes.
Previous reports have documented serious complications from small distal stones, including spontaneous forniceal rupture and ureteral perforation [7-9]. In these cases, stone size did not reliably predict clinical severity. While significant AKI secondary to unilateral distal obstruction remains less commonly described, delayed recognition of persistent obstruction has been implicated in renal impairment.
In the present case, alternative causes of AKI were considered. Baseline renal function was normal. There was no evidence of systemic infection, hypotension, or hypovolemia. Electrolytes were stable, and dialysis was not required. The contralateral kidney was radiographically normal. Although NSAIDs were prescribed, the temporal association of worsening obstruction on repeat imaging with concurrent hydronephrosis supports obstructive pathophysiology as the primary mechanism.
Current urological guidelines recommend reassessment and consideration of repeat imaging in patients with persistent pain or worsening renal function despite conservative management [4,5]. In this case, repeat imaging was pivotal in identifying new hydronephrosis and confirming persistent obstruction, prompting timely intervention. From a clinical standpoint, this case highlights that stone size alone should not determine reassurance. Persistent symptoms, reduced urine output, or biochemical deterioration warrant prompt reassessment and possible escalation of care.
Conclusions
This case illustrates that small distal ureteral stones may still result in clinically significant obstruction and postrenal AKI despite initially reassuring imaging findings. Persistent symptoms or reduced urine output following conservative management should prompt reassessment and repeat imaging. Stone size alone should not determine clinical reassurance, and appropriate safety-netting and follow-up are essential to prevent delayed recognition of obstruction and renal impairment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of stone disease across the world World J Urol Sorokin I Mamoulakis C Miyazawa K Rodgers A Talati J Lotan Y 130113203520172821386010.1007/s 00345-017-2008-6 · doi ↗ · pubmed ↗
- 2Prevalence of kidney stones in the United States Eur Urol Scales CD Jr Smith AC Hanley JM Saigal CS 1601656220122249863510.1016/j.eururo.2012.03.052PMC 3362665 · doi ↗ · pubmed ↗
- 3Urolithiasis-an interdisciplinary diagnostic, therapeutic and secondary preventive challenge Dtsch Arztebl Int Fisang C Anding R Müller SC Latz S Laube N 839111220152572143510.3238/arztebl.2015.0083 PMC 4349965 · doi ↗ · pubmed ↗
- 4EAU guidelines on interventional treatment for urolithiasis Eur Urol Türk C Petřík A Sarica K Seitz C Skolarikos A Straub M Knoll T 4754826920162634491710.1016/j.eururo.2015.07.041 · doi ↗ · pubmed ↗
- 5Surgical management of stones: American Urological Association/Endourological Society Guideline, PART IJ Urol Assimos D Krambeck A Miller NL 1153116019620162723861610.1016/j.juro.2016.05.090 · doi ↗ · pubmed ↗
- 62007 guideline for the management of ureteral calculi J Urol Preminger GM Tiselius HG Assimos DG 2418243417820071799334010.1016/j.juro.2007.09.107 · doi ↗ · pubmed ↗
- 7Clinical approach to diagnosing acute and chronic tubulointerstitial disease Adv Chronic Kidney Dis Perazella MA 57632420172828438010.1053/j.ackd.2016.08.003 · doi ↗ · pubmed ↗
- 8Spontaneous ureteral rupture: a rare case report and review of literature Radiol Case Rep El Alaoui A Ouraghi A Salem HD El Moudane A Barki A 221022122020254004695510.1016/j.radcr.2025.01.044PMC 11880888 · doi ↗ · pubmed ↗