Expert Tibia Nail: Is a Single Nail Enough to Fix Distal Tibia and Fibula Fractures?
Birju Manjhi, Abhijeet Kunwar, Dipesh Raj Rajak, Utkarsh Kumar, Rituraj Kumar, Anil Kumar Singh Patel

TL;DR
This study finds that using a single Expert Tibial Nail System (ETNS) can effectively treat certain tibia and fibula fractures without needing additional fibular fixation, leading to better outcomes and fewer complications.
Contribution
The study introduces the effectiveness of the ETNS for treating distal tibia and fibula fractures without fibular fixation, challenging conventional surgical practices.
Findings
ETNS fixation resulted in shorter surgery time, less blood loss, and reduced radiation exposure compared to conventional methods.
Patients treated with ETNS had faster bone union and better functional outcomes as measured by the Olerud-Molander ankle score.
ETNS had fewer complications, including lower rates of infection, ankle stiffness, and non-union, compared to fibular plating.
Abstract
Background Management of extra-articular distal tibia fractures associated with supra-syndesmotic fibula fractures remains controversial, particularly regarding the need for fibular fixation. With the advent of the Expert Tibial Nail System (ETNS), which provides multidirectional distal locking, adequate stability may be achieved without fibular fixation, potentially reducing surgical morbidity. Objective To compare clinical, radiological, intra-operative parameters, and complication rates between isolated ETNS fixation and conventional tibial intramedullary (IM) nailing with fibular plating in extra-articular distal tibia and fibula fractures. Materials and methods A hybrid (prospective and retrospective) comparative study was conducted from April 2023 to March 2025, including 120 patients aged 18-60 years with extra-articular distal tibia fractures (4-10 cm from the tibial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
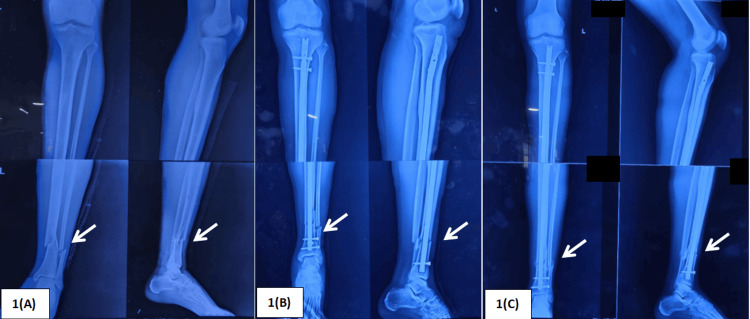 Figure 1
Figure 1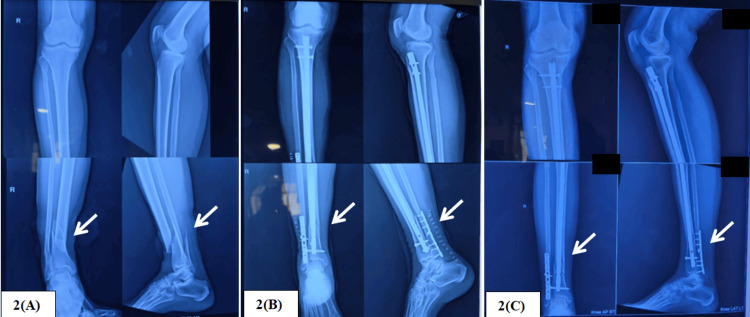 Figure 2
Figure 2| Parameters | ETNS | Tibial nail + fibular plate | Total |
| Mean age | 35.9 ± 10.48 years | 38.06 ± 11 years | 36.6 years |
| Gender | Male: 38 (63.33%); Female: 22 (36.67%) | Male: 36 (60%); Female: 24 (40%) | Male: 74 (61.66%); Female: 46 (38.33%) |
| Laterality | Right: 32 (53.33%); Left: 28 (46.67%) | Right: 34 (56.67%); Left: 26 (43.33%) | Right: 66 (55%); Left: 54 (45%) |
| Mode of injury | RTA: 44 (73.33%); Others: 16 (26.67%) | RTA: 42 (70%); Others: 18 (30%) | RTA: 86 (71.66%); Others: 34 (28.33%) |
| Comorbidity | Smoking: 12 (20%); Diabetes: 8 (13.33%) | Smoking: 18 (30%); Diabetes: 6 (10%) | Smoking: 30 (25%); Diabetes: 14 (11.67%) |
| Parameter | ETNS | Tibial nail + fibular plate | p-value | t-statistic | ||||
| Mean | Range | SD | Mean | Range | SD | |||
| Duration of surgery (min) | 32.9 | 23-48 | 6.91 | 63.86 | 56-82 | 8.73 | <0.001 | -21.54 |
| Blood loss (mL) | 15.53 | 12-25 | 3.16 | 48.91 | 35-65 | 9.91 | <0.001 | -24.86 |
| C-arm shots (number of shots) | 22.68 | 15-38 | 3.89 | 33.55 | 26-48 | 3.97 | <0.001 | -15.15 |
| Parameters | ETNS | Tibial nail + fibular plate | p-value | t-statistic | ||||
| Mean | Range | SD | Mean | Range | SD | |||
| Follow-up (months) | 14.6 | 12-19 | 5.2 | 13.8 | 12-18.5 | 5.1 | 0.063 | 1.88 |
| Olerud-Molander score at 24 weeks | 96 | 90-100 | 6.21 | 90.66 | 82-94 | 6.53 | <0.001 | 12.11 |
| Union time (weeks) | 18.1 | 13-24 | 2.07 | 22.5 | 17-28 | 1.59 | <0.001 | -7.79 |
| Complication | ETNS group | Tibial nail + fibular plate |
| Total | 14 | 26 |
| Superficial surgical site infection | 3 | 5 |
| Deep infection | 0 | 3 |
| Ankle stiffness | 2 | 8 |
| Anterior knee pain | 4 | 3 |
| Procurvatum/recurvatum > 10° | 2 | 2 |
| Varus/valgus > 10° | 3 | 3 |
| Non-union | 0 | 2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone fractures and treatments · Foot and Ankle Surgery · Orthopedic Surgery and Rehabilitation
Introduction
Overall incidence of tibia fractures is 51.7/100,000 per year; of these, distal tibia fractures account for 17.65% [1]. Due to biomechanical interdependence, 75%-90% of distal tibia fractures are associated with concurrent fibula fractures [2]. They cause a substantial burden to the healthcare system. Multiple treatment options are available, from conservative to operative, yet their management is challenging. This complexity is due to poor soft tissue coverage of the tibia, a high degree of comminution due to high-velocity trauma, and poor skin condition. In addition, there are no strict guidelines regarding fixation of the fibula.
The articular part (syndesmotic and infra-syndesmotic) of the fibula plays a crucial role in ankle stability; hence, there is an invariable need for its fixation. However, fixation of the supra-syndesmotic fibula is still controversial. Some surgeons, such as Rüedi T and Allgower M [3], stated that the primary step in fixation of distal tibia and fibula fractures is fixation of the fibula, which helps with indirect reduction of the tibia fracture, while another group of surgeons believes that an intact fibula contributes very little to the stability of the lower leg, creates abnormal strain, and complicates compression at the tibia fracture site [4,5].
For extra-articular distal tibia fractures, the intramedullary (IM) tibia interlock nail is the most commonly used device for fixation, but it provides only uniplanar interlocking screws, which limits the rotational stability provided by the IM nail; hence, fibula fixation may be necessary to achieve multiplanar stability. Since the introduction of the Expert Tibia Nail System (ETNS) [6] in August 2004, it has been claimed to provide additional stability through the multidirectional locking options in both the proximal and distal parts of the nail. Fixing extra-articular tibia fractures with ETNS without fixing a concurrent fibula fracture may provide sufficient multiplanar stability without the complications associated with fibula fixation. Hence, we conducted this study to compare conventional tibia nailing with fibula plating versus isolated Expert tibia nailing for the treatment of extra-articular distal tibia and fibula fractures.
Materials and methods
To compare isolated ETNS fixation with conventional tibial nailing with fibular plating, we conducted a hybrid study (prospective + retrospective) from April 2023 to March 2025 in the Department of Orthopaedics and Traumatology, Institute of Medical Sciences, Banaras Hindu University. We selected a group of 60 patients aged 18-60 years who provided written informed consent to participate in the study and had extra-articular distal tibia and fibula fractures. The tibial fracture was located between 4 cm and 10 cm from the tibial plafond, with a concurrent supra-syndesmotic fibular fracture lying within 9 cm of the syndesmosis; patients presented within 7 days of trauma and were treated with ETNS only (Figure 1). Patients with open fractures, pathological fractures, polytrauma, and pre-existing arthritic conditions were excluded.
Patient in the ETNS group treated with isolated Expert Tibial nailing.1(A) Preoperative X-ray 1(B) Immediate postoperative X-ray 1(C) 12-week follow-up X-rayETNS: Expert Tibial Nail System.
Preoperatively, name, age, gender, laterality, date of injury, mode of injury, and any associated comorbidities were recorded. After routine investigations, patients were taken for surgery following a pre-anesthetic check-up. All patients were operated under similar conditions: supine position, under C-arm guidance, and spinal anesthesia. Surgeries were performed by experienced orthopedic surgeons, and routine surgical steps were followed [6]. Intraoperatively, duration of surgery (in minutes), blood loss (in milliliters; estimated using the gauze visual analogue method) [7], and radiation exposure (number of C-arm shots) were recorded.
One IV antibiotic dose was given preoperatively, and two doses were given postoperatively. Knee and ankle range of motion was started on postoperative day 1. Dressing check and mobilization with a walker, without weight bearing, were done on postoperative day 2. The patient was discharged on oral antibiotics on postoperative day 3 and called on day 14 for suture removal. Toe-touch/partial weight bearing was allowed after 3 weeks. A check X-ray was done at 4 weeks, and patients were called for follow-up monthly thereafter until 12 months. Serial X-rays were performed to document union or any complication. Full weight bearing was allowed once union was documented on X-ray (i.e., three united cortices in two orthogonal X-ray views).
These patients were compared with a group of 60 patients with similar fractures who satisfied the inclusion criteria and were previously operated on at our center with conventional tibial nailing and fibular plating (Figure 2). Clinical outcomes were compared using the Olerud-Molander ankle score [8], and radiological outcomes (union time and deformity) were assessed using orthogonal radiographs of the operated leg. Angulation <10° was considered acceptable in the anteroposterior view (varus/valgus) and lateral view (procurvatum/recurvatum). During follow-up, complications such as non-union, malunion, stiffness, surgical site infection, implant failure, etc., were recorded.
Patient in the tibial nail + fibular plating group treated with a tibial interlocking nail and fibular plate.2(A) Preoperative X-ray 2(B) Immediate postoperative X-ray 2(C) 12-week follow-up X-ray
Statistical analysis
Data were recorded, and continuous variables were expressed as mean and SD and compared using Student’s t-test [9]. Categorical data were expressed as percentages and ranges and compared using the chi-square test [10]. Results were considered significant at p < 0.05.
Results
Mean duration of follow-up was 14.2 months, with an SD of 5.1, and a range of 12-19 months. Mean age of the study population was 36.6 years (ETNS group: 35.9 ± 10.48 vs tibial nailing + fibular plating group: 38.06 ± 11). Out of 120 study subjects, 74 (61.66%) were male and 46 (38.33%) were female. Sixty-six (55%) patients sustained trauma on the right side, while 54 (45%) had a left-sided injury. Road traffic accidents (RTA) were the most common mode of injury, affecting 86 (71.66%) patients, followed by 34 (28.33%) patients who sustained trauma due to falls or sports injuries. Fifty-four (45%) patients had associated comorbidities, i.e., smoking and diabetes. Group-wise demographic distribution of the patient population is presented in Table 1.
All intraoperative parameters recorded during the study, duration of surgery (in minutes), blood loss (in mL), and C-arm exposure (number of shots), were in favor of patients treated with ETNS, with shorter duration, lower blood loss, and less radiation exposure. All parameters with p-value < 0.05 favored the ETNS group (Table 2).
At 24 weeks of follow-up, when union was recorded, and after a significant duration of rehabilitation, the final outcomes of the study were assessed. Clinical outcome was recorded using the Olerud-Molander ankle score, and union was assessed on X-ray (three united cortices out of four in two orthogonal radiographs) (Figures 1-2). Both clinical outcome and union time favored the ETNS group, with p-value < 0.05. The Olerud-Molander ankle score and union time for both groups are documented in Table 3.
Complications
A total of 40 (30%) complications were recorded during the study: 14 in the ETNS group and 26 in the tibial nailing + fibular plating group. Complications such as deep/superficial surgical site infections, anterior knee pain, ankle stiffness, deformity, malunion, and non-union were recorded and are summarized in Table 4.
Discussion
Distal tibia and fibula fractures are a common orthopaedic problem [11], and their anatomical location (poor soft tissue coverage at the distal part of the tibia) and high rate of postoperative complications make them difficult to treat. For a long time, rules established by Rüedi T and Allgower M [3] have formed the basis for the fixation of distal tibia and fibula fractures, where the first step was reduction and fixation of the fibula to restore the length and rotation of the tibia [4]. With advancement of implants and in view of the recent literature, there is an ongoing debate regarding fixation of the fibula. Some authors have suggested that fibular fixation helps in the treatment of distal tibia fractures by restoring reduction and providing rotational stability to the tibia [12], and leads to fewer complications with the fibula fixed compared to when it is left untreated [13,14]. Whereas another group of surgeons believe that there is no additional advantage of fixing the extra-articular fibula in distal tibia and fibula fractures [15,16]. Since the introduction of the ETNS, which promises sufficient rotational stability via multidirectional interlocking screws and can be used in more distal fractures through a tip interlocking mechanism, ETNS might be the solution to this ongoing debate, as sufficient rotational stability can be achieved without fixing the fibula.
The mean age of the study population was 36.6 years (ETNS group: 35.9 ± 10.48 years and tibial nail + fibular plate group: 38.06 ± 11 years). This is consistent with the study conducted by Javdan M et al. [17], where the mean age of the study population was 36.9 ± 13.1 years (case group) and 34.8 ± 12.5 years (control group), in contrast to the study conducted by Pogliacomi F et al. [18], where the mean age of the study population was 56.4 ± 11.6 years (group A, with fibular fixation) and 59.8 ± 13.3 years (group B, without fibular fixation). The majority of the participants were male (61.66%; ETNS group: 63.66% and tibial nail + fibular plate group: 60%), similar to the study by Javdan M et al. [17] with 91.83% males and Pogliacomi F et al. [18] with 59.77% males. This may be because the most common mechanism of injury in all three studies was RTA (Javdan M et al.: 93.87% RTA; our study: 71.66% RTA), which predominantly affects the male population. There was no significant difference in laterality, as both right and left sides were similarly involved. There was no significant difference in associated comorbidities between the groups.
All intraoperative parameters were in favor of the ETNS group compared to the tibial nail + fibular plate group: duration of surgery was 32.9 min vs 63.86 min, blood loss during surgery was 15.53 mL vs 48.91 mL, and radiation exposure during surgery was 22.68 shots vs 33.55 shots in the ETNS and tibial nail + fibular plate groups, respectively. As the entire procedure of fibular fixation was omitted in the ETNS group, procedures were quicker, with less blood loss and less radiation exposure.
Patients were followed for a mean duration of 14.2 months (ETNS group: 14.6 months and tibial nailing + fibular plating group: 13.8 months). During follow-up, earlier union was seen in patients in the ETNS group compared to those treated with tibial nailing + fibular plating (18.1 weeks vs 22.5 weeks, respectively). These results can be explained by the theory of inhibition of cyclical compression at the tibial fracture site described by Teitz CC et al. [19]. In addition, open reduction of the fibula may disturb the fracture hematoma at the tibial fracture site, which can further delay union. Similar results have been reported in other studies where fibular fixation led to delayed union/non-union [20,21]. At six months of follow-up, a better Olerud-Molander ankle score was recorded in the ETNS group (96) compared to the tibial nailing + fibular plating group (90.66). Favorable results in the ETNS group are attributed to early fracture union, less postoperative pain due to a smaller surgical scar leading to earlier range of motion during rehabilitation, and fewer implant- and surgery-related complications.
A total of 40 (30%) complications were reported in the study, of which 14 (23.33%) occurred in the ETNS group and 26 (43.33%) occurred in the tibial nailing + fibular plating group. Overall, the ETNS group had fewer complications. Eight superficial surgical site infections were reported: 3 in the ETNS group and 5 in the tibial nailing + fibular plating group. All were treated with oral antibiotics and regular dressing changes; none required surgical intervention. Three cases of deep infection were reported, all in the tibial nailing + fibular plating group at the fibular plate incision site. In one case, the infection subsided with IV antibiotics and regular dressing. One case required surgical debridement and secondary closure after wound dehiscence. One patient underwent implant removal; however, union had already occurred at the time of removal, so no additional procedure to achieve union was required. Ten cases of ankle stiffness were recorded: 2 in the ETNS group and 8 in the tibial nailing + fibular plating group. The higher incidence of ankle stiffness in the comparison group is attributed to the fibular plate incision, as pain at the incision site can interfere with postoperative rehabilitation, and the surgical scar may further increase ankle joint stiffness. Anterior knee pain was reported in seven patients (4 in the ETNS group and 3 in the tibial nailing + fibular plating group). Anterior knee pain is a commonly reported complication following tibial nailing [22], and the incidence was comparable between groups. Four cases of sagittal plane deformity >10° were noted (2 in each group), and 6 cases of coronal plane deformity >10° were noted (3 in each group). Patients with these deformities did not have significant functional limitation; therefore, no surgical intervention was needed. Two cases of non-union were reported, both in the tibial nailing + fibular plating group. One case was treated with exchange nailing, and the second required bone grafting along with exchange nailing. The higher incidence of non-union in the tibial nailing + fibular plating group may be because the fixed length of the fibula prevents relative micro-movements at the tibial fracture site (inhibition of cyclical compression) [19], which can inhibit callus formation and union.
Our study is limited by the short study duration, limited number of patients, single-center design, and relatively short follow-up; therefore, long-term results and complications could not be recorded. Further large-scale randomized controlled trials with longer follow-up are recommended to validate these findings and establish clear guidelines regarding fibular fixation in distal tibial fractures.
Conclusions
The management of extra-articular distal tibia fractures associated with supra-syndesmotic fibula fractures continues to be debated, particularly regarding the necessity of fibular fixation. Findings from the present study demonstrate that isolated fixation using the ETNS provides adequate multiplanar stability without the need for concurrent fibular plating.
Patients treated with ETNS showed significantly reduced operative time, blood loss, and radiation exposure, reflecting a less invasive and more efficient surgical approach. Additionally, earlier fracture union and superior functional outcomes, as measured by the Olerud-Molander ankle score, were observed in the ETNS group. The overall complication rate, including infection, ankle stiffness, and non-union, was notably lower compared to patients treated with conventional tibial nailing and fibular plating.
These results suggest that fixation of the fibula in extra-articular distal tibia fractures may not only be unnecessary when using modern multidirectional locking nails but may also contribute to delayed union and increased complications. Therefore, isolated ETNS fixation appears to be a safe, effective, and biologically favorable option for treating these injuries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology and incidence of tibia fractures in the Swedish Fracture Register Injury Wennergren D Bergdahl C Ekelund J Juto H Sundfeldt M Möller M 20682074492018 https://www.sciencedirect.com/science/article/abs/pii/S 00201383183048933022063410.1016/j.injury.2018.09.008 · doi ↗ · pubmed ↗
- 2Anatomy, biomechanics and pathomechanics of the tibial pilon Ful Sprunggelenk Bartonícek J Mittlmeier T Rammelt S 311102012
- 3Fractures of the lower end of the tibia into the ankle-joint Injury Rüedi TP Allgöwer M 929911969 https://www.injuryjournal.com/article/S 0020-1383(69)80066-5/abstract
- 4Plating of the fibula. Its potential value as an adjunct to external fixation of the tibia Clin Orthop Relat Res Morrison KM Ebraheim NA Southworth SR Sabin JJ Jackson WT 209213(266)1991 https://pubmed.ncbi.nlm.nih.gov/2019053/2019053 · pubmed ↗
- 5Fractures of the lower end of the tibia into the ankle joint: results 9 years after open reduction and internal fixation Injury Rüedi T 13013451973 https://www.sciencedirect.com/science/article/abs/pii/S 0020138373800890477476410.1016/s 0020-1383(73)80089-0 · doi ↗ · pubmed ↗
- 6Expert Tibial Nail System (ETNS) 11 2004 2004 https://www.aofoundation.org/approved/approvedsolutionsfolder/2004/expert-tibial-nail-system-etns
- 7Blood loss estimation using gauze visual analogue Trauma Mon Ali AE Aleisa AA Alsubaie HI Buhlaiqah NR Algadeeb JB Alsneini HA 0212016 https://pubmed.ncbi.nlm.nih.gov/27626017/10.5812/traumamon.34131 PMC 500349927626017 · doi ↗ · pubmed ↗
- 8Olerud and Molander Scoring System J Orthop Trauma 0202006 https://journals.lww.com/jorthotrauma/fulltext/2006/09001/olerud_and_molander_scoring_system.25.aspx