Necrotizing Pneumonia in an Elderly Patient With Chronic Obstructive Pulmonary Disease (COPD): A Case Report
Andreia Salgadinho Machado, Raquel Borrego, Marta Roldão, Marta Anastácio, Sandra André

TL;DR
An elderly COPD patient developed necrotizing pneumonia, requiring multiple antibiotic changes before recovery, highlighting the challenges in treating this severe condition.
Contribution
This case report emphasizes the complexities of diagnosing and managing necrotizing pneumonia in COPD patients with inconclusive microbiological findings.
Findings
The patient showed clinical improvement after meropenem, but no microbiologic confirmation linked recovery to this antibiotic.
Necrotizing pneumonia in COPD patients requires individualized treatment and frequent reassessment due to diagnostic uncertainty.
Broad-spectrum antibiotics like carbapenems should be used cautiously, based on clinical evidence rather than isolated case experiences.
Abstract
Necrotizing pneumonia (NP) is a severe complication of bacterial pneumonia, characterized by progressive lung necrosis and cavitation. Although advances in imaging and supportive care have improved outcomes, NP remains difficult to manage due to poor antibiotic penetration, frequent polymicrobial infection, and the lack of standardized treatment protocols. An 85-year-old man with chronic obstructive pulmonary disease (COPD) (Global Initiative for Obstructive Lung Disease (GOLD) group C) and a 40-pack-year former smoking history, managed with long-acting beta-agonist/long-acting muscarinic antagonist (LABA/LAMA), was admitted with acute dyspnea and productive cough. Imaging showed left-sided pneumonia, and methicillin-sensitive Staphylococcus aureus (MSSA) was isolated. Amoxicillin-clavulanate led to transient improvement, but recurrent fever, worsening hypoxemia, and new cavitary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
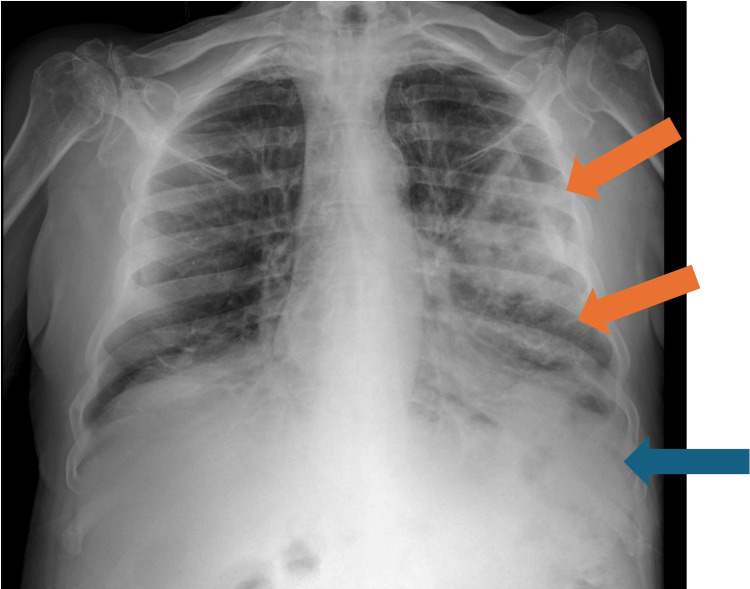 Figure 1
Figure 1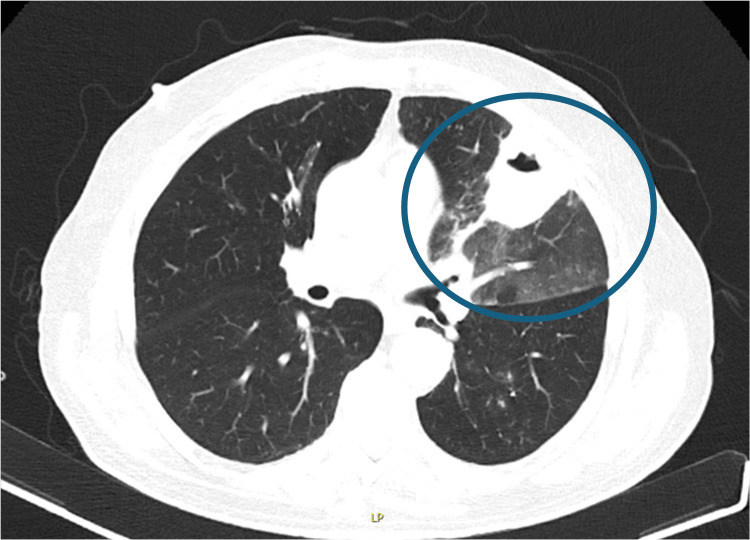 Figure 2
Figure 2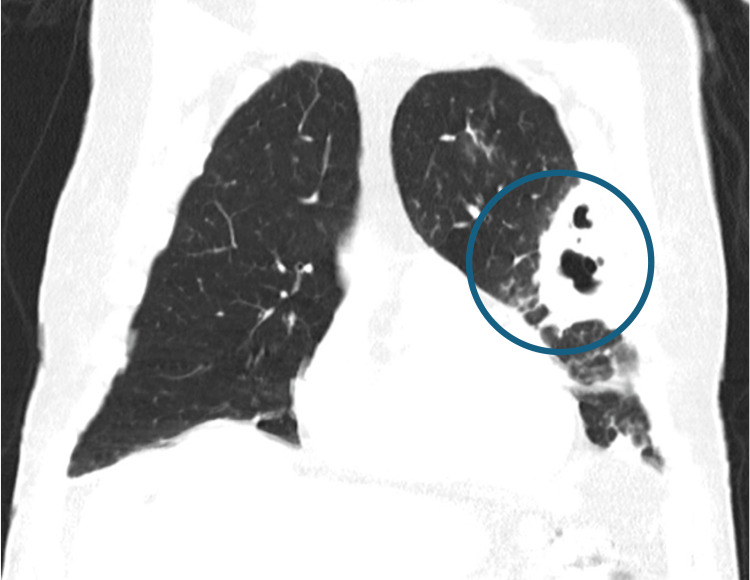 Figure 3
Figure 3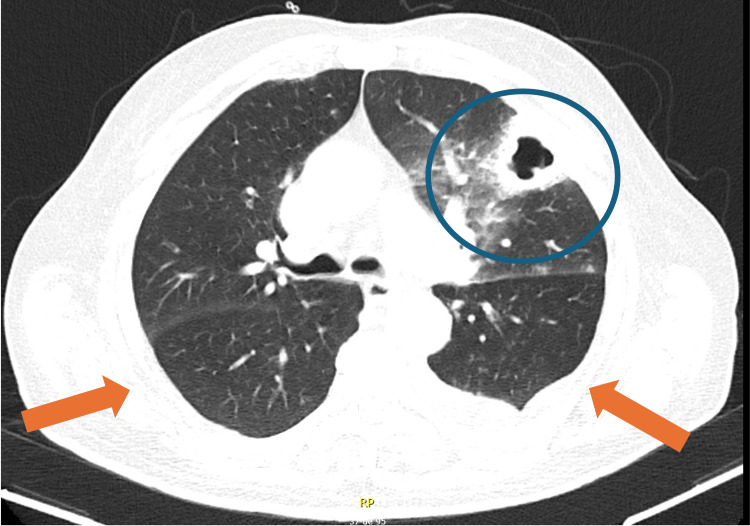 Figure 4
Figure 4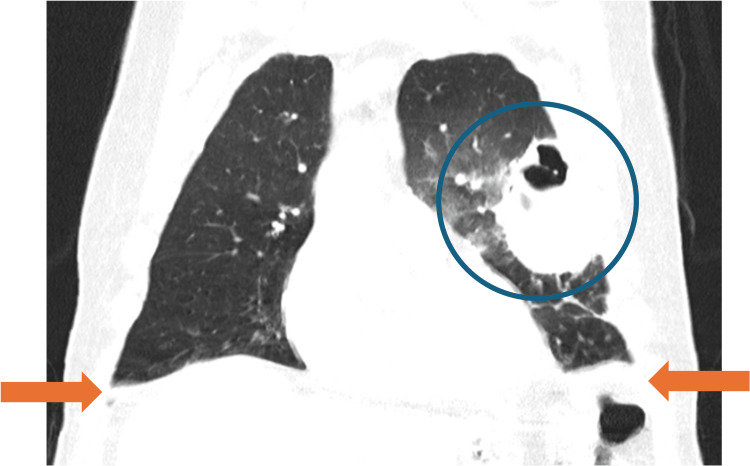 Figure 5
Figure 5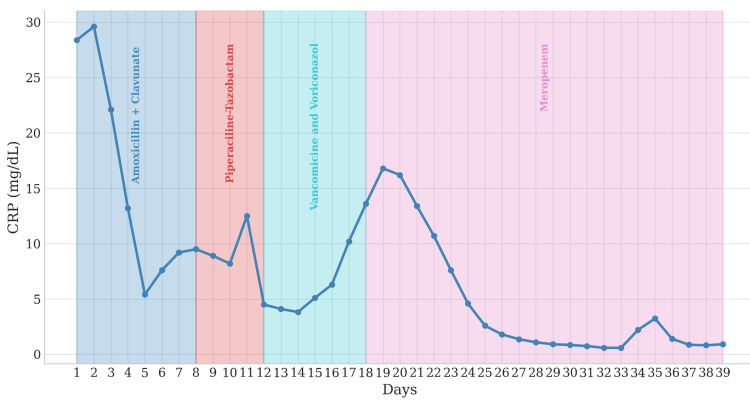 Figure 6
Figure 6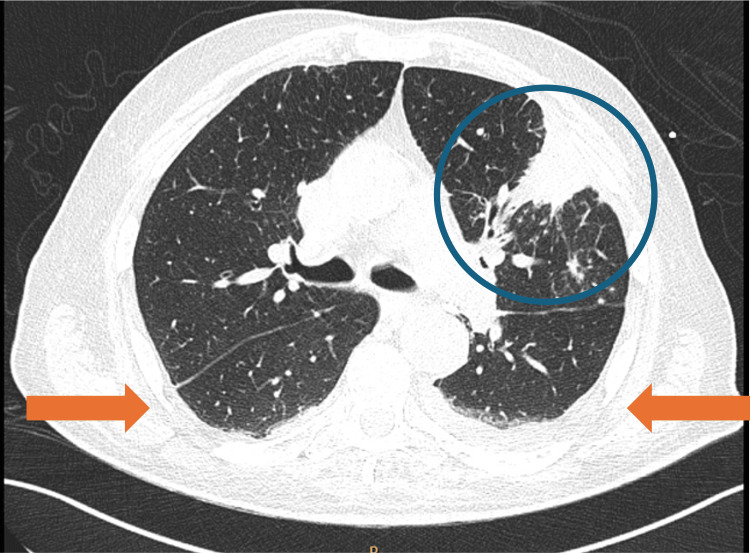 Figure 7
Figure 7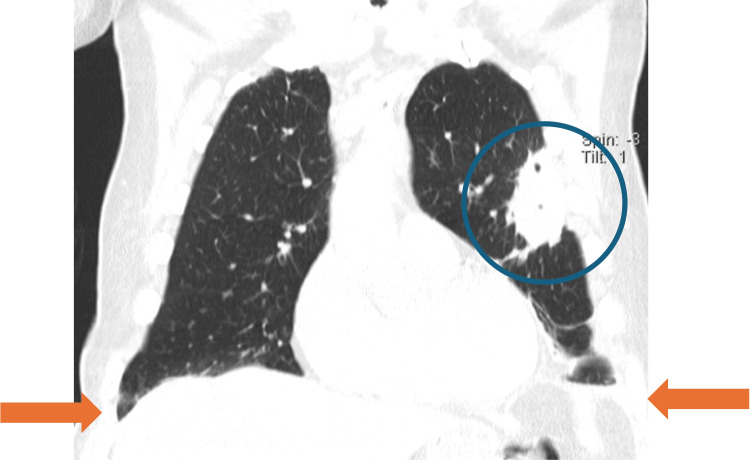 Figure 8
Figure 8| Laboratory parameter | Normal range | Result |
| Hemoglobin (g/dL) | 12-15.3 | 10.7 |
| White Blood Cells (x10^9/L) | 4.0-11.0 | 24900 |
| Neutrophils (x10^9/L) | 1.9-7.5 | 21340 |
| Lymphocytes (x10^9/L) | 1.0-4.8 | 1370 |
| Eosinophils (x10^9/L) | 0-0.5 | 500 |
| Platelets (x10^9/L) | 150-450 | 378 |
| C-reactive protein (mg/dL) | <0.5 | 28.4 |
| Fibrinogen (g/L) | 2-4 | 9.44 |
| D-dimer (ng/mL) | <500 | 2058 |
| Urea (mg/dL) | 16-49 | 65 |
| Creatinine (mg/dL) | 0.5-0.9 | 1.04 |
| Arterial blood gas | ||
| pH | 7.35-7.35 | 7.37 |
| pO₂ (mmHg) | 75–100 | 74 |
| pCO2 (mmHg) | 35-45 | 35 |
| HCO3 (mmol/L) | 22-26 | 21 |
| Lactate (mmol/L) | 0.5–2.0 | 1.5 |
| Autoimmune and hematologic panel | Normal range | Result |
| Complement C3 (mg/dL) | 90-180 | 118 |
| Complement C4 (mg/ dL) | 10-40 | 23.3 |
| Rheumatoid factor (IU/L) | <15 | <15 |
| Anti-cyclic citrullinated peptide antibodies (u/ml) | <5 | <5 |
| Anti-nuclear antibodies | Negative | Negative |
| Anti-dsDNA antibodies | Negative | Negative |
| Anti-Ro/La/Sm/U1-RNP/Scl-70/Jo-1 | Negative | Negative |
| Anti-hepatic antigens antibodies (LKM-1, LC-1, SLA/LP, AMA-M2, AMA-M2-3E, Sp 100, PML, gp210) | Negative | Negative |
| Anti-neutrophil cytoplasmic antibody (c-ANCA, p-ANCA) | Negative | Negative |
| Angiotensin-converting enzyme | Negative | Negative |
| Serum protein electrophoresis | Inflammatory pattern and no monoclonal spike | |
| Beta-2 microglobulin (mg/dL) | 1.09-2.53 | 1.51 |
| Kappa free light chains (mg/L) | 3.3–19.4 | 24.5 |
| Lambda free light chains (mg/L) | 5.7- 26.3 | 39,0 |
| Kappa/Lambda ratio | 0.26-0.65 | 0,628 |
| IgG (mg/dL) | 600−1600 | 1160,0 |
| IgA (mg/dL) | 80−450 | 418,0 |
| IgM (mg/L) | 50-200 | 24,5 |
| Infectious agent | Result |
| Hepatitis B surface antigen | Negative |
| Hepatitis B surface antibody HBs | Negative |
| Hepatitis B core antibody | Negative |
| Hepatitis C antibody | Negative |
| Antibodies against HIV-1 and HIV-2 | Negative |
| Interferon gamma release assay (IGRA) | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Nosocomial Infections in ICU · Pleural and Pulmonary Diseases
Introduction
Necrotizing pneumonia (NP) is a severe complication of bacterial pneumonia, resulting in pulmonary tissue necrosis and cavity formation. Management of NP is challenging due to the involvement of the most frequently implicated pathogens, Streptococcus pneumoniae, Staphylococcus aureus, and Klebsiella pneumoniae, limited antibiotic penetration to affected areas, and the frequent failure of laboratory tests to identify the causative organism [1].
The clinical presentation of NP ranges from mild symptoms to life-threatening infection, depending on the extent of pulmonary involvement and the patient’s comorbidities. Older adults and individuals with chronic illnesses are particularly susceptible to severe complications. Prompt recognition and timely escalation of antibiotic therapy are essential to mitigate adverse outcomes [2].
This report presents a case of necrotizing pneumonia in an elderly man with chronic obstructive pulmonary disease (COPD). We highlight the diagnostic and therapeutic challenges encountered and discuss key clinical lessons derived from this case.
Case presentation
An 85-year-old male with chronic obstructive pulmonary disease (COPD) (Global Initiative for Obstructive Lung Disease (GOLD) group C) and a 40-pack-year smoking history, managed with long-acting beta-agonist/long-acting muscarinic antagonist (LABA/LAMA) therapy, presented to the emergency department on the first day of illness. He reported two days of progressive dyspnea, orthopnea, and productive cough with brownish sputum. Recent, unquantified weight loss was noted, while fever, night sweats, and chest pain were denied. On admission, the patient was tachypneic at rest (24 breaths/min) with an oxygen saturation of 95% on a 2 L/min nasal cannula. He appeared fatigued and dyspneic. Lung auscultation revealed diminished breath sounds, wheezes, and rhonchi over the left upper field, with bilateral crackles. Blood pressure was 144/98 mmHg, heart rate 103 bpm, regular, with a grade II/VI systolic murmur. Bilateral pitting edema was present up to the knees. Laboratory tests demonstrated normocytic normochromic anemia, neutrophilic leukocytosis, elevated C-reactive protein and fibrinogen, increased D-dimers, and mild renal dysfunction. Arterial blood gases on 2 L/min oxygen indicated hypoxemia without hypocapnia or hyperlactatemia (Table 1).
Chest X-ray demonstrated left-sided pneumonia and a pleural effusion (Figure 1). Nasopharyngeal swabs for SARS-CoV-2 and methicillin-resistant Staphylococcus aureus (MRSA), as well as urinary antigen tests for Streptococcus pneumoniae and Legionella pneumophila, were negative. Microbiological evaluation included the collection of sputum and blood cultures at admission, prior to initiation of antibiotic therapy. Due to the minimal volume of the effusion, thoracentesis for pleural fluid sampling was not performed.
Chest X-ray at admission showing left-sided pneumonia (orange arrows) and pleural effusion (blue arrow)
A diagnosis of community-acquired pneumonia with type I respiratory failure was established. Empiric antibiotic therapy with amoxicillin-clavulanate and clarithromycin was initiated. Systemic corticosteroids were administered due to underlying COPD. The CURB-65 score was 5, warranting admission for close monitoring.
Initial clinical and laboratory improvement was observed, including resolution of fever and reduction in inflammatory markers. Sputum culture identified methicillin-sensitive Staphylococcus aureus (MSSA), prompting discontinuation of clarithromycin. Blood cultures remained negative.
On day 4 of hospitalization, increasing inflammatory markers prompted bronchoscopy. Three sputum samples were tested for acid-fast bacilli and Mycobacterium tuberculosis PCR, all of which were negative. CT imaging revealed peribronchovascular interstitial thickening, ground-glass opacities, left upper lobe consolidation, a juxtaplural cavitary lesion, bilateral “tree-in-bud” micronodules, basal bronchiectasis, and mediastinal lymphadenopathy (Figures 2, 3). Antibiotic therapy was escalated to piperacillin-tazobactam.
Axial chest CT demonstrating left upper-lobe consolidation with a well-defined cavitary lesion and surrounding parenchymal inflammation (blue circle)
Coronal chest CT demonstrating extensive left upper-lobe consolidation with a well-defined cavitary lesion and surrounding parenchymal inflammation (blue circle)
By day 10, worsening hypoxemia necessitated 40% oxygen via Venturi mask. CT angiography excluded pulmonary embolism and revealed new right-sided consolidations and increased left pleural effusion (Figures 4, 5). Due to radiologic progression, piperacillin-tazobactam was discontinued, and therapy was escalated to vancomycin and voriconazole. The patient was transferred to the Non-Invasive Ventilation Unit (NIVU) on day 14.
Axial Chest CT showing bilateral progression with cavitary transformation (blue circle) and pleural effusion (orange arrows)
Coronal chest CT demonstrating extensive left upper-lobe consolidation with a large cavitary lesion (blue circle) and pleural effusion (orange arrows)
During the NIVU stay, recurrent fever and hemodynamic instability developed, necessitating norepinephrine (maximum 0.05 mcg/kg/min) and high-flow nasal cannula oxygen (60 L/min, fraction of inspired oxygen (FiO₂) 60%). Empyema was excluded by thoracentesis, and empiric meropenem was initiated. Repeat sputum and blood cultures were obtained during each episode of clinical deterioration, all of which remained negative. Pleural fluid cultures were not performed. Bronchoscopy with bronchoalveolar lavage (BAL)excluded MRSA and fungal infection (negative galactomannan antigen). Vancomycin and voriconazole were discontinued after 6 days due to lack of response. Following initiation of meropenem, marked clinical improvement was observed, including resolution of fever, declining inflammatory markers, and reduced oxygen requirements (Figure 6).
Temporal evolution of C-reactive protein (CRP) levels showing correlation with antibiotic therapy changes
After 11 days of vasopressor support, hemodynamic stability was achieved, and the patient was transferred to the medical ward on day 32 of illness. Oxygen therapy was discontinued on day 37, and the patient remained eupneic on room air. A 21-day course of meropenem was completed. Follow-up CT demonstrated regression of left upper-lobe cavitation, resolution of right lower-lobe infiltrates, and reduced pleural effusions (Figures 7, 8).
Axial chest CT demonstrating improvement of left upper-lobe consolidation with reduction of the cavitary component (blue circle) and decreased bilateral pleural effusions (orange arrows).
Coronal chest CT demonstrating interval improvement of the left upper-lobe consolidation with reduction of the cavitary component (blue circle), along with decreased bilateral pleural effusions (orange arrows).
Due to the atypical severity and progression of the respiratory infection, comprehensive evaluations were conducted to identify potential underlying causes of immunosuppression predisposing to necrotizing pneumonia. During hospitalization, targeted screening for secondary immunodeficiency was performed, including assessments for autoimmune diseases, hematologic malignancies (Table 2), and chronic infections (Table 3), which were negative. Glycated hemoglobin was 5.9%, excluding diabetes mellitus, and transthoracic echocardiography ruled out structural heart disease.
The patient was discharged in stable condition after a 39-day hospital stay and remained asymptomatic at pulmonary follow-up in February 2023. Imaging revealed mild residual fibrosis in the left upper lobe.
Discussion
Necrotizing pneumonia (NP) is a severe condition that necessitates immediate and aggressive intervention because of its high mortality risk. The estimated prevalence of NP is 10-12%. NP is defined by progressive parenchymal necrosis, liquefaction, and cavitary destruction within consolidated lung tissue [1].
The underlying pathogenesis involves severe inflammatory injury, resulting in vascular thrombosis, tissue ischemia, and impaired antibiotic penetration [3].
Elderly patients and individuals with chronic lung conditions like COPD are especially at risk because of weakened airway defenses. This increases their likelihood of experiencing severe, sometimes polymicrobial infections, delayed recovery, and complications such as necrotizing pneumonia [4].
Necrotizing pneumonia may initially resemble severe community-acquired pneumonia, with necrotizing changes becoming apparent as the disease progresses [5]. CT scans are the best way to confirm NP, as they show the lung damage and cavities [6]. In our patient, repeated CT scans helped show that the disease was getting worse, even though he seemed better at first.
Laboratory tests did not identify the specific bacteria causing the infection, which is common in NP and makes it difficult to determine whether the problem is a recurrence of the initial infection or a new hospital-acquired infection [6].
There are currently no standardized protocols for NP management, which relies on clinical judgment, multidisciplinary input, and antimicrobial stewardship. Empiric broad-spectrum antibiotics should be individualized and frequently reassessed based on patient evolution and, when available, microbiological data [7].
The patient initially received amoxicillin-clavulanate for MSSA, with only transient improvement. Clinical deterioration necessitated escalation to broader-spectrum agents, including piperacillin-tazobactam, vancomycin, and voriconazole, but without clinical benefit. Although clinical improvement was noted after initiation of meropenem, attributing this response solely to infection with multidrug-resistant Gram-negative organisms remains speculative in the absence of microbiological confirmation or local resistance data. Alternative explanations, such as delayed antibiotic response, improved lung penetration, or cumulative antimicrobial effects, cannot be excluded. The decision to escalate to carbapenem therapy should be carefully considered and always guided by antimicrobial stewardship principles to avoid the risks associated with unnecessary early use of broad-spectrum agents, especially when multidrug resistance is not confirmed [8].
Necrotizing pneumonia can be very dangerous, with death rates as high as 45% in severe cases, especially for patients with other health issues. However, careful monitoring and being ready to change treatment can lead to recovery, even for high-risk patients [7]. Despite being older and having COPD, our patient recovered fully with medication alone. His case shows that promptly recognizing changes on scans and adjusting antibiotics can prevent serious problems.
Necrotizing pneumonia is a life-threatening complication of bacterial pneumonia that requires early diagnosis, close monitoring, and aggressive antimicrobial management. Clinical deterioration despite appropriate therapy should prompt suspicion of superinfection with resistant organisms. Empiric escalation to carbapenem coverage, guided by imaging findings, clinical response, and local antimicrobial resistance patterns, may be lifesaving in selected patients.
Conclusions
Necrotizing pneumonia remains a severe complication of bacterial pneumonia, with significant morbidity and mortality, particularly in elderly patients with chronic lung disease. This case highlights the importance of dynamic clinical reassessment and timely recognition of radiologic progression. While escalation of antimicrobial therapy may be warranted in the setting of treatment failure, recommendations regarding empiric carbapenem use should be made cautiously. In the absence of microbiological confirmation, the observed clinical improvement with meropenem in this case should be interpreted as hypothesis-generating rather than practice-changing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Necrotizing pneumonia (aetiology, clinical features and management)Curr Opin Pulm Med Krutikov M Rahman A Tiberi S 2252322520193084492110.1097/MCP.0000000000000571 · doi ↗ · pubmed ↗
- 2Necrotizing pneumonia: a practical guide for the clinician Pathogens Kapania EM Cavallazzi R 13202410.3390/pathogens 13110984 PMC 1159780039599537 · doi ↗ · pubmed ↗
- 3Pulmonary gangrene: radiological and pathologic correlation South Med J Curry CA Fishman EK Buckley JA 957960911998 https://pubmed.ncbi.nlm.nih.gov/9786293/9786293 · pubmed ↗
- 4Necrotizing pneumonia as a complication of community-acquired pneumonia in adults at a tertiary institution J Clin Med Boppana LK Isern S Romero KN Ferreira J Garvan G Ashby T 14202510.3390/jcm 14124086 PMC 1219380840565832 · doi ↗ · pubmed ↗
- 5The incidence of necrotizing changes in adults with pneumococcal pneumonia Clin Infect Dis Pande A Nasir S Rueda AM 10165420122204287810.1093/cid/cir 749 · doi ↗ · pubmed ↗
- 6Necrotizing pneumonia: a rare complication of pneumonia requiring special consideration Curr Opin Pulm Med Tsai YF Ku YH 2462521820122238858510.1097/MCP.0b 013e 3283521022 · doi ↗ · pubmed ↗
- 7Survival with optimal medical management in a cohort of severe necrotizing bacterial lung infections J Thorac Dis Larose JC Wang HT Rakovich G 386038691520233755965910.21037/jtd-22-1590 PMC 10407478 · doi ↗ · pubmed ↗
- 8Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society Clin Infect Dis Kalil AC Metersky ML Klompas M 063201610.1093/cid/ciw 353PMC 498175927418577 · doi ↗ · pubmed ↗