Invasive Pulmonary Aspergillosis in a Young Adult With Hyperimmunoglobulin E Syndrome and Hypogammaglobulinemia Following Rituximab Therapy
Gautam K Pandrangi, Ritika N Golechha, Logan R Mills, John T Brown, Nicholas Helmstetter

TL;DR
A young adult with a rare immune disorder and low antibody levels developed a severe fungal lung infection after treatment for lymphoma.
Contribution
This case highlights the risk of invasive aspergillosis in HIES patients with hypogammaglobulinemia following rituximab therapy.
Findings
The patient's respiratory decline was due to invasive pulmonary aspergillosis, not bacterial infection.
Rituximab-induced hypogammaglobulinemia increased the risk of opportunistic fungal infections in this HIES patient.
Early fungal testing is critical in immunocompromised patients with worsening symptoms despite antibiotics.
Abstract
Hyperimmunoglobulin E syndrome (HIES) is a rare primary immunodeficiency marked by elevated IgE levels, recurrent skin and pulmonary infections, and immune dysregulation. While typically diagnosed in childhood, adult presentations can occur, often complicated by structural lung disease, opportunistic infections, and malignancies. We report a 37-year-old female with signal transducer and activator of transcription 3 (STAT3)-deficient HIES, diffuse large B-cell lymphoma (DLBCL) in remission, rituximab-induced hypogammaglobulinemia, and recurrent infections, who presented with acute-on-chronic dyspnea. Imaging revealed a large cavitary lesion in the left upper lobe. Despite 30 days of appropriate antibiotics targeting methicillin-resistant Staphylococcus aureus (MRSA) and gram-negative organisms, her respiratory status deteriorated, necessitating intubation. Subsequent bronchoalveolar…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
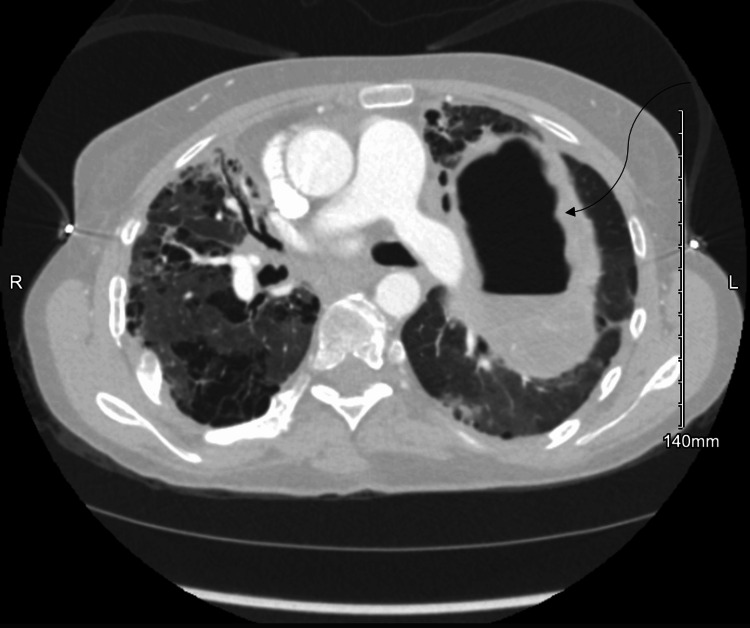 Figure 1
Figure 1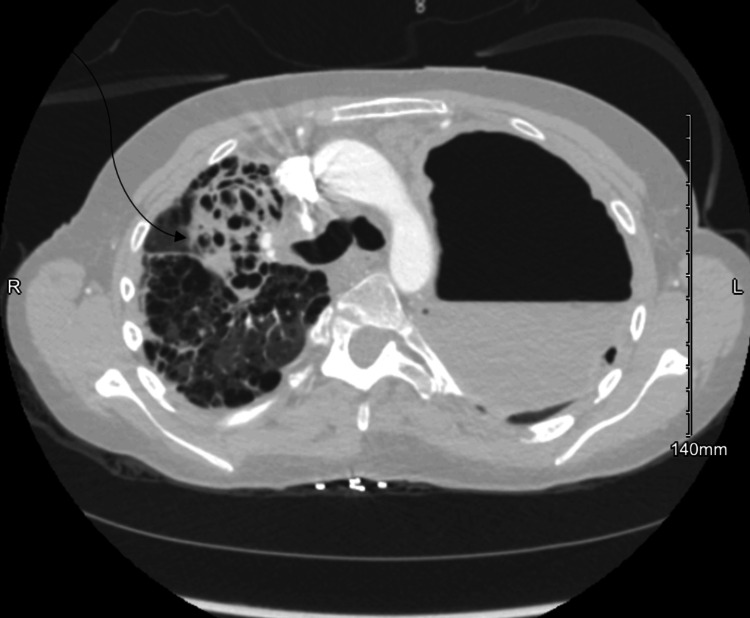 Figure 2
Figure 2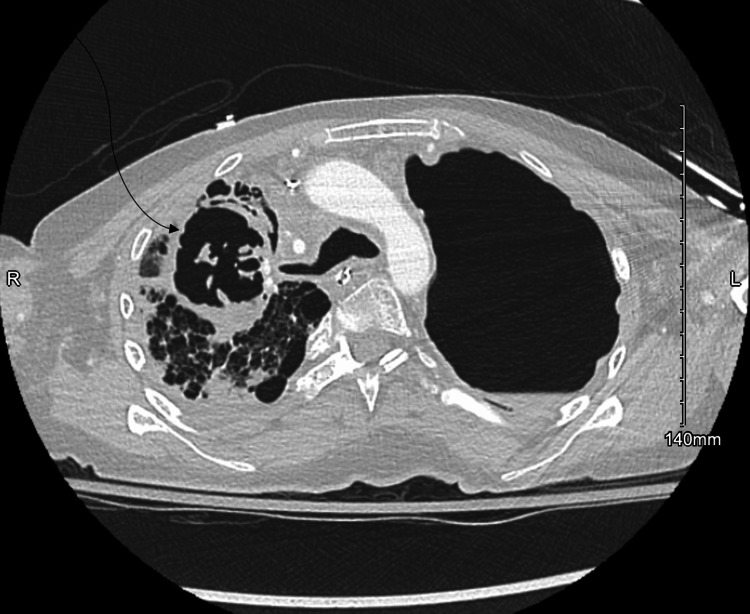 Figure 3
Figure 3| Feature | Description | Clinical Implication |
|
| Autosomal dominant, dominant-negative | Impaired Th17 differentiation leading to compromised neutrophil recruitment |
| Typical disease progression | Recurrent bacterial infections → structural lung damage → recurrent infections | Cavitary lesions and bronchiectasis increase fungal infection risk |
| Early pathogens | Staphylococcus aureus | Predominantly bacterial infections in childhood |
| Late pathogens |
| Opportunistic infections in advanced disease |
| Clinical relevance | Advanced structural lung disease | High risk for invasive pulmonary aspergillosis in adults |
| Feature | Description | Clinical Implication |
| Malignancy | Increased risk of lymphomas, especially DLBCL | Immune dysregulation predisposes to lymphoma |
| Therapy | Rituximab-based chemotherapy | CD20-positive B-cell depletion leads to prolonged hypogammaglobulinemia |
| Duration of immune suppression | Up to 24 months following rituximab | Increased susceptibility to serious infections |
| IVIG use | Not routinely indicated in | Considered in secondary hypogammaglobulinemia with structural lung disease |
| Clinical challenge | Self-discontinuation due to myalgias | Loss of humoral protection; need alternative formulations or premedication |
| Feature | Description | Clinical Implication |
| Polymicrobial cultures |
| Diagnostic uncertainty in advanced structural lung disease |
| Initial interpretation | Bacterial pathogens treated; fungal organisms presumed colonizers | Delay in antifungal therapy |
| Clinical course | Progressive respiratory decline despite antibiotics | Suggests a superimposed invasive fungal infection |
| Diagnostic complexity | Overlapping colonization and infection | Requires reassessment and multimodal diagnostics |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImmunodeficiency and Autoimmune Disorders · Otitis Media and Relapsing Polychondritis · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
Hyperimmunoglobulin E syndrome (HIES), formerly known as Job syndrome, is a heterogeneous group of primary immunodeficiencies characterized by markedly elevated IgE levels and recurrent infections [1]. The autosomal dominant form is most commonly caused by dominant-negative mutations in the signal transducer and activator of transcription 3 (STAT3) gene, resulting in multisystem disease involving the immune system, skeletal and integumentary system, dentition, and connective tissues [2]. STAT3 mutations impair T helper 17 (Th17) cell differentiation, thereby compromising neutrophil recruitment. Keratinocytes and bronchial epithelial cells rely on Th17 cytokines, in combination with classical proinflammatory signals, to produce anti-staphylococcal factors, including chemokines and antimicrobial peptides [3]. This mechanism explains the selective vulnerability to skin and pulmonary infections observed in HIES [3].
Although HIES typically presents in childhood, recognition in adult patients is essential. Progressive immune dysfunction and cumulative pulmonary damage increase susceptibility to severe and opportunistic infections. Thus, this case aims to highlight the complex interplay of primary immunodeficiency, secondary immunosuppression, and structural lung disease resulting in life-threatening invasive pulmonary aspergillosis (IPA) in the setting of STAT3-deficient HIES.
Case presentation
A 37-year-old female with autosomal dominant STAT3-deficient HIES, diffuse large B-cell lymphoma (DLBCL) in remission since 2024, chronic hypoxemic respiratory failure requiring 2 L/min of home supplemental oxygen, and rituximab-induced hypogammaglobulinemia presented with acute-on-chronic dyspnea. She had a documented allergy to trimethoprim-sulfamethoxazole (urticaria) and had self-discontinued intravenous immunoglobulin (IVIG) therapy several months prior to presentation.
Her medical history was significant for recurrent methicillin-resistant Staphylococcus aureus (MRSA) pulmonary infections resulting in progressive structural lung disease, including bronchiectasis and pneumatoceles. In March 2024, she was diagnosed with DLBCL. Her oncologic course was complicated by multiple episodes of necrotizing pneumonia and recurrent lung abscesses. Thus, she was only able to tolerate two out of six rounds of standard first-line treatment with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) chemotherapy. Despite the abbreviated regimen, she achieved remission.
Following chemotherapy, IVIG was initiated to provide passive immunity and reduce infection burden. This was self-discontinued by the patient due to serum-sickness-like symptoms with diffuse myalgias and arthralgias. She was subsequently hospitalized for left upper lobe pneumonia, with cultures growing Serratia and Klebsiella aerogenes, and she was discharged on levofloxacin.
Despite adherence to treatment, her respiratory status worsened, with increasing oxygen requirements, prompting readmission. Computed tomography (CT) of the chest revealed a 12×12×9 cm cavitary lesion in the left upper lobe (Figure 1), consistent with a lung abscess. It also showed extensive areas of bronchiectasis, bronchial wall thickening, and airspace opacities in the right upper lobe and apex, suggesting a second cavitary lesion (Figure 2). Respiratory cultures grew MRSA and Klebsiella pneumoniae. Bronchial cultures also yielded Candida albicans and *Aspergillus *species, which were initially interpreted as colonizers.
Computed Tomography Scan Demonstrating a Large Left Upper Lobe Cavitary Lesion With Surrounding InfiltratesThe image shows a de-identified left upper lobe cavitary lesion in a patient with STAT3-deficient hyperimmunoglobulin E syndrome and secondary hypogammaglobulinemia. No identifying patient information is present, and informed consent for publication was obtained.
Computed Tomography Scan Demonstrating a Cavitary Lesion of the Right Upper Lobe and ApexThe image shows a de-identified right upper lobe cavitary lesion in a patient with STAT3-deficient hyperimmunoglobulin E syndrome and secondary hypogammaglobulinemia. No identifying patient information is present, and informed consent for publication was obtained.
Despite empiric therapy targeting MRSA and gram-negative organisms with vancomycin and cefepime, her respiratory failure progressed, necessitating intubation. Follow-up chest CT demonstrated increasing complexity of the right apical cavitation (Figure 3). Though initial bronchial cultures suggested *Aspergillus *species colonization, repeat tracheal aspirates grew MRSA in addition to *Aspergillus *species. Thus, in combination with the full clinical picture, bronchoalveolar lavage (BAL) and serum galactomannan testing were used to confirm IPA. Combination antifungal therapy with voriconazole and micafungin was initiated, along with continued antibacterial therapy with vancomycin, linezolid, and ertapenem. Her hospitalization lasted 51 days, including one month of antifungal treatment at standard adult dosing.
Follow-Up Computed Tomography Scan Demonstrating Further Progression of the Right Upper Lobe Cavitary LesionThe image shows a de-identified right upper lobe cavitary lesion in a patient with STAT3-deficient hyperimmunoglobulin E syndrome and secondary hypogammaglobulinemia. Compared with Figure 2, the cavitation shows increased complexity and wall thickening, suggestive of progression such as fungal infection or necrotizing pneumonia. No identifying patient information is present, and informed consent for publication was obtained.
Discussion
Baseline aspergillosis risk in STAT3-deficient HIES
STAT3-deficient HIES is associated with progressive pulmonary structural damage compared with other HIES variants [4]. Disease progression typically follows a three-step process: recurrent bacterial infections, development of structural lung abnormalities, and subsequent reinfections that further exacerbate pulmonary injury [5]. Early infections are predominantly Staphylococcus aureus, while later stages involve opportunistic pathogens such as *Aspergillus *species, Mycobacterium tuberculosis, and Pseudomonas aeruginosa [5]. Our patient had reached the advanced disease stage, placing her at a higher risk for invasive fungal infections (Table 1).
DLBCL and rituximab-induced hypogammaglobulinemia
Patients with STAT3-deficient HIES are predisposed to lymphomas due to underlying immune dysregulation, with DLBCL reported among the most common malignancies [6,7]. Our patient developed DLBCL and was treated with two cycles of R-CHOP (Table 2). Rituximab depletes CD20-positive B cells, which can result in prolonged hypogammaglobulinemia that may persist for up to 24 months, with sustained IgG reductions of four months or longer conferring a significantly increased risk of serious infections [8]. Notably, our patient presented nearly one year after cessation of R-CHOP therapy, illustrating the prolonged window of immunologic vulnerability that can persist despite oncologic remission.
Although IVIG therapy is not routinely indicated in STAT3-deficient HIES, given that most patients retain baseline antibody production, this case represents a unique clinical context [9,10]. Recent chemotherapy, rituximab-induced hypogammaglobulinemia, structural lung disease, and recurrent infections created a compounded risk state that justified immunoglobulin replacement. Thus, IVIG was initiated to provide passive immunity and reduce infectious burden while maintaining IgG levels within the normal range. However, the patient self-discontinued IVIG due to myalgias and arthralgias, resulting in loss of critical humoral immune support and further increasing susceptibility to encapsulated bacteria and opportunistic pathogens [9]. Alternative strategies such as subcutaneous immunoglobulin, premedication protocols, or different IVIG formulations may have allowed continued immunoglobulin replacement while minimizing adverse effects [11,12].
Polymicrobial nature and diagnostic complexity
The polymicrobial nature of this patient’s infection reflects severely compromised host defense and structural lung disease, characteristic of advanced HIES, contributing to diagnostic complexity (Table 3). Initial respiratory cultures grew Klebsiella, MRSA, Candida albicans, and Aspergillus species. Bacterial pathogens were initially presumed causal, while Candida and Aspergillus were considered colonizers. Respiratory status continued to decline despite appropriate antibiotic therapy. Progression from bacterial pneumonia to invasive aspergillosis illustrates how bacterial infections can create favorable conditions for fungal superinfection in cavitary lesions [13]. This underscores the importance of continuously re-assessing treatment response and considering alternative superinfections in patients with worsening clinical status.
Invasive aspergillosis carries mortality rates exceeding 50% in critically ill patients if not adequately treated, making early diagnosis critical [14]. Complex cases may require multiple diagnostic modalities, including cultures from multiple sites, imaging, BAL, and serum markers such as galactomannan, beta-D-glucan, and PCR assays [15]. The American Thoracic Society supports serum and BAL galactomannan testing as alternatives when tissue biopsy is not feasible [15]. Lung biopsy should be pursued if noninvasive testing fails and is clinically appropriate.
Management challenges and treatment considerations
The Infectious Diseases Society of America (IDSA) and American Thoracic Society recommend voriconazole as first-line therapy for invasive aspergillosis, with isavuconazole and liposomal amphotericin B as alternatives [16,17]. Given the high mortality in critically ill patients, combination therapy with voriconazole and an echinocandin may be considered in high-risk cases [17]. This patient required intubation due to acute hypoxic respiratory failure, underscoring disease severity. She received micafungin and voriconazole for one month, alongside cefepime, vancomycin, linezolid, and ertapenem for bacterial coverage.
Prophylaxis gaps and preventive strategies
This case highlights critical gaps in infection prevention. The National Comprehensive Cancer Network (NCCN) recommends mold-active antifungal prophylaxis for patients at intermediate to high infection risk, including those undergoing or recently completing intensive chemotherapy [18]. Given her HIES, structural lung disease, and planned R-CHOP therapy, this patient would have been an ideal candidate for primary antifungal prophylaxis [5]. The IDSA recommends mold-active triazoles when the risk of invasive aspergillosis exceeds 6%, a threshold likely met by this patient [16]. Guidelines may benefit from clarification that STAT3-deficient HIES patients with structural lung damage should receive extended antimicrobial coverage, including antifungals [16].
Discontinuation of IVIG due to myalgias represents a missed opportunity for ongoing humoral immune support. Alternative IVIG preparations, subcutaneous immunoglobulin, or premedication strategies could have maintained prophylaxis while mitigating adverse effects [19]. Secondary prophylaxis following initial bacterial infections during chemotherapy should also be considered. Given a sulfa-drug allergy limiting *Pneumocystis jirovecii *prophylaxis, alternatives such as atovaquone or dapsone could have been employed [20].
Conclusions
This case highlights the potentially severe consequences when multiple layers of immune dysfunction overlap: primary immunodeficiency (STAT3-deficient HIES), structural lung disease, secondary immunosuppression (rituximab-induced hypogammaglobulinemia), and gaps in prophylaxis. Optimal outcomes depend on rapid recognition, prompt antifungal therapy, and surgical intervention when needed. Long-term care requires vigilance for recurrent infections, proactive pulmonary management, and strategic use of antifungal prophylaxis during periods of heightened immunologic risk.
Several important diagnostic and management principles emerge from this presentation. In immunocompromised patients with progressive respiratory symptoms despite adequate antibacterial treatment, clinicians should maintain a broad differential diagnosis that includes invasive fungal disease. Early diagnostic evaluation with fungal biomarkers, advanced imaging, and tissue sampling, when feasible, may facilitate earlier diagnosis and improve outcomes. Optimal management is best achieved through a multidisciplinary approach involving immunology, infectious diseases, oncology, and pulmonary medicine, allowing coordinated decisions regarding antimicrobial therapy, immunoglobulin replacement strategies, and procedural interventions. Prophylactic measures should be strongly considered in patients with overlapping risk factors for invasive fungal infections. When standard therapies are contraindicated or poorly tolerated, individualized strategies, including alternative immunoglobulin formulations or modified premedication protocols, may be necessary to ensure continuity of care. Recognition of this compounded high-risk state is critical to minimizing diagnostic delays and reducing morbidity and mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1STAT 3 mutations in the hyper-Ig E syndrome N Engl J Med Holland SM De Leo FR Elloumi HZ 1608161935720071788174510.1056/NEJ Moa 073687 · doi ↗ · pubmed ↗
- 2Dominant-negative mutations in the DNA-binding domain of STAT 3 cause hyper-Ig E syndrome Nature Minegishi Y Saito M Tsuchiya S 1058106244820071767603310.1038/nature 06096 · doi ↗ · pubmed ↗
- 3Impaired T(H)17 cell differentiation in subjects with autosomal dominant hyper-Ig E syndrome Nature Milner JD Brenchley JM Laurence A 77377645220081833772010.1038/nature 06764 PMC 2864108 · doi ↗ · pubmed ↗
- 4Practice parameter for the diagnosis and management of primary immunodeficiency J Allergy Clin Immunol Bonilla FA Khan DA Ballas ZK 1186120513620152637183910.1016/j.jaci.2015.04.049 · doi ↗ · pubmed ↗
- 5Pulmonary features and stage of disease in adult patients with hyper-Ig E syndrome: a single-centre clinical study and literature review Orphanet J Rare Dis Xie T Xu N Zhao H 2702020254046221910.1186/s 13023-025-03749-6PMC 12131643 · doi ↗ · pubmed ↗
- 6A systematic review regarding the prevalence of malignancy in patients with the hyper-Ig E syndrome Clin Exp Med Mohammadi T Azizi G Rafiemanesh H Farahani P Nirouei M Tavakol M 483548592320233792445510.1007/s 10238-023-01228-5 · doi ↗ · pubmed ↗
- 7Diffuse large B cell lymphoma in hyper-Ig E syndrome due to STAT 3 mutation J Clin Immunol Kumánovics A Perkins SL Gilbert H Cessna MH Augustine NH Hill HR 8868933020102085966710.1007/s 10875-010-9452-z · doi ↗ · pubmed ↗
- 8Association of immunoglobulin levels, infectious risk, and mortality with rituximab and hypogammaglobulinemia JAMA Netw Open Barmettler S Ong MS Farmer JR Choi H Walter J 01201810.1001/jamanetworkopen.2018.4169 PMC 632437530646343 · doi ↗ · pubmed ↗