Initial Vancomycin Taper for the Prevention of Recurrent Clostridioides difficile Infection: A Randomized Clinical Trial
Emily G. McDonald, Guillaume Butler-Laporte, James M. Brophy, Sarah Elsayed, Charles Frenette, Iman Huseen, Vivian G. Loo, Kristen Moran, Bryan Coburn, Susy S. Hota, Yves Longtin, Ling Y. Kong, Matthew P. Muller, Theodore S. Steiner, Louis Valiquette, Nick Daneman, Peter Daley

TL;DR
A 4-week vancomycin pulse and taper regimen may help prevent early recurrence of Clostridioides difficile infection compared to a 2-week pulse regimen.
Contribution
The study introduces a new vancomycin taper regimen to reduce recurrence of Clostridioides difficile infection.
Findings
The vancomycin pulse and taper regimen had a 73.8% posterior probability of superiority in preventing recurrence at day 56.
Recurrence at day 38 was significantly lower in the taper group compared to the pulse-only group.
Adverse effects were rare in both treatment groups.
Abstract
Does a 4-week pulse and taper regimen of vancomycin reduce the risk of recurrent Clostridioides difficile infection compared with a standard pulse regimen among patients with a first episode or first recurrence? In this randomized clinical trial of 265 participants, the posterior probability of superiority for vancomycin pulse plus taper was 74%. The trial was stopped early due to feasibility of recruitment. The vancomycin pulse and taper regimen could represent a safe and accessible treatment option to delay or prevent early recurrence of C difficile infection. This randomized clinical trial tested whether a 4-week pulse and taper vancomycin regimen was superior to a 2-week pulse regimen for preventing recurrence among patients with a first episode or first recurrence of Clostridioides difficile infection. Clostridioides difficile infection (CDI) is associated with substantial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
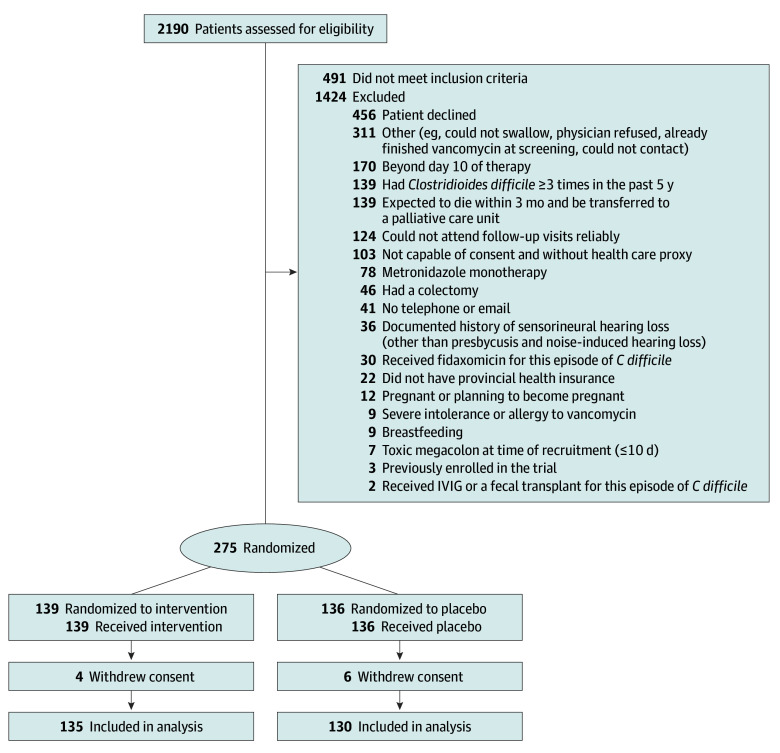 Figure 1
Figure 1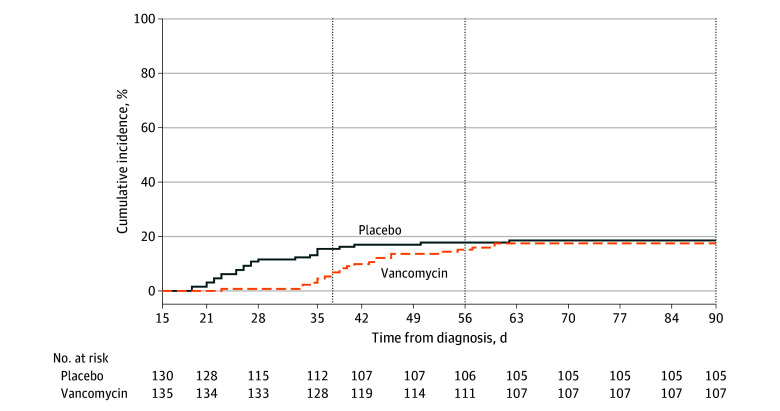 Figure 2
Figure 2| Characteristic | Patient group, No. (%) | ||
|---|---|---|---|
| Intervention (n = 135) | Placebo (n = 130) | All (n = 265) | |
| Age, median (IQR), y | 63 (44-76) | 62 (50-76) | 63 (47-74) |
| Sex | |||
| Female | 77 (57.0) | 61 (46.9) | 138 (52.1) |
| Male | 58 (43.0) | 69 (53.1) | 127 (47.9) |
| Language | |||
| English | 99 (73.3) | 90 (69.2) | 189 (71.3) |
| French | 36 (26.7) | 40 (30.8) | 76 (28.7) |
| Setting of diagnosis | |||
| Outpatient | 40 (29.6) | 40 (30.8) | 80 (30.2) |
| ED | 50 (37.0) | 34 (26.2) | 84 (31.7) |
| Hospital | 45 (33.3) | 56 (43.1) | 101 (38.1) |
| Comorbidities | |||
| Proton pump inhibitor use | 62 (45.9) | 57 (43.8) | 119 (44.9) |
| Solid organ cancer | 22 (16.3) | 28 (21.5) | 50 (18.9) |
| Without metastases | 14 (10.4) | 19 (14.6) | 33 (12.5) |
| With metastases | 8 (5.9) | 9 (6.9) | 17 (6.4) |
| Hematologic cancer | 13 (9.6) | 9 (6.9) | 22 (8.3) |
| With transplant | 3 (2.2) | 2 (1.5) | 5 (1.9) |
| Solid organ transplant | 14 (10.4) | 18 (13.8) | 32 (12.1) |
| Inflammatory bowel disease | 8 (5.9) | 21 (16.2) | 29 (10.9) |
| CDI details | |||
| Diagnosis by EIA for toxin | 2 (1.5) | 4 (3.1) | 6 (2.3) |
| First episode | 124 (91.9) | 121 (93.1) | 245 (92.5) |
| Concurrent antibiotics at enrollment | 23 (17.0) | 24 (18.5) | 47 (17.7) |
| Cotreatment | |||
| Nonstudy antibiotics | 21 (15.6) | 33 (25.4) | 54 (20.4) |
| Open-label vancomycin prophylaxis | 16 (11.9) | 15 (11.5) | 31 (11.7) |
| Characteristic | Patient group, No. (%) | Adjusted relative risk (95% CrI) | Posterior probability of superiority, % | |
|---|---|---|---|---|
| Intervention group (n = 135) | Placebo group (n = 130) | |||
| Recurrence of CDI | ||||
| Day 56 (primary outcome) | 20 (14.8) | 23 (17.7) | 0.84 (0.48-1.45) | 73.8 |
| Day 38 (secondary outcome) | 9 (6.7) | 20 (15.4) | 0.43 (0.19-0.89) | 99.0 |
| Day 90 (secondary outcome) | 23 (17.0) | 24 (18.5) | 0.92 (0.54-1.56) | 62.1 |
| Complications by day 90 | ||||
| All-cause mortality | 4 (3.0) | 2 (1.5) | 3.91 (0.44-34.50) | 9.8 |
| Colectomy | 0 | 0 | NA | NA |
| ED or readmission to hospital | 22 (16.3) | 26 (20.0) | 0.82 (0.48-1.38) | 78.3 |
| ED or readmission to hospital for CDI | 3 (2.2) | 1 (0.8) | 2.85 (0.30-27.01) | 16.4 |
| Secondary CDI therapies by day 90 | ||||
| Fecal microbiota transplant | 0 | 0 | NA | NA |
| Receipt of fidaxomicin | 1 (0.7) | 4 (3.1) | 0.19 (0.01-1.47) | 94.2 |
| Outcome | Patient group, No. (%) | |
|---|---|---|
| Intervention (n = 132) | Placebo (n = 129) | |
| Any adverse effect | 15 (11.4) | 13 (10.1) |
| Stopped study drug due to effect | 2 (1.5) | 3 (2.3) |
| Required health care contact due to effect | 1 (0.8) | 1 (0.8) |
| Gastrointestinal | ||
| Heartburn and/or reflux | 1 (0.8) | 1 (0.8) |
| Abdominal discomfort | 3 (2.3) | 3 (2.3) |
| Nausea | 4 (3.0) | 1 (0.8) |
| Diarrhea | 2 (1.5) | 3 (2.3) |
| Mouth sores | 1 (0.8) | 0 |
| Nongastrointestinal | ||
| Headache | 1 (0.8) | 1 (0.8) |
| Light-headedness | 0 | 2 (1.6) |
| Tingling | 0 | 1 (0.8) |
| Drowsiness | 1 (0.8) | 0 |
| Vertigo | 0 | 0 |
| Tinnitus | 0 | 0 |
| Rash | 2 (1.5) | 2 (1.6) |
| Pruritus | 0 | 1 (0.8) |
| Leg swelling | 1 (0.8) | 0 |
| Upper respiratory tract infection symptoms | 1 (0.8) | 1 (0.8) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Antimicrobial Resistance in Staphylococcus · Antibiotic Use and Resistance
Introduction
There are more than 450 000 cases of Clostridioides difficile infection (CDI) annually in the US and another 37 000 cases in Canada with an estimated combined annual cost approaching 5 billion.^[1](#zoi251619r1),[2](#zoi251619r2),[3](#zoi251619r3),[4](#zoi251619r4)^ Even with successful treatment, approximately 20% to 25% of patients develop recurrent CDI (rCDI) within 8 weeks.^[5](#zoi251619r5),[6](#zoi251619r6)^ The morbidity and mortality of recurrences^[7](#zoi251619r7)^ are estimated to cost 2.8 billion in the US^8^ and $65 million annually in Canada.^4^ Consequently, there is an urgent need for strategies to prevent rCDI.
One treatment option to prevent recurrence is fidaxomicin, having demonstrated a clinically significant reduction in the risk of rCDI compared with 10 days of vancomycin monotherapy (15.4% vs 25.3%) for patients experiencing a first or a second episode of CDI.^9^ In the fidaxomicin randomized clinical trials,^9,20^ a more pronounced difference in relapse was observed within 14 days of stopping vancomycin therapy (7.4% for fidaxomicin vs 19.3% for vancomycin), whereas later, recurrence rates were similar (8.1% for vancomycin vs 6.6% for fidaxomicin).^10^ This is relevant as the duration of vancomycin treatment for CDI arose from limited animal and observational data, potentially derived from a single case report of resolution following 10 days of treatment.^11^ Furthermore, despite the availability of fidaxomicin and newer treatments for CDI during the last 10 to 15 years, a recent international survey found that more than 66% of clinicians still use vancomycin for the initial treatment of CDI.^12^
Longer vancomycin pulse and taper regimens are used in the treatment of multiple recurrences of CDI and are effective for preventing recurrence following initial episodes of C difficile in the in vitro gut model^13^ and in retrospective cohort studies (mean treatment duration of 25 days).^14^ Recognizing that fidaxomicin is not universally available and is more expensive than vancomycin even after accounting for lower recurrence,^15^ we sought to determine whether a 4-week pulse and taper vancomycin regimen would be superior for preventing rCDI when compared with a 2-week pulse vancomycin regimen.
Methods
Trial Design and Oversight
The Initial Vancomycin Taper for the Prevention of Recurrent Clostridium Difficile Infection (TAPER-V) was a parallel-design double-blind clinical trial. TAPER-V began recruitment November 19, 2020, and all follow-up was completed by October 4, 2024. The protocol was approved by local and/or provincial research ethics boards at all participating sites with the Research Institute of the McGill University Health Centre serving as the board of record. The trial was conducted with a “no objection letter” from Health Canada. The protocol and statistical analysis plan are included in Supplement 1. We followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline. All patients or their substitute decision makers provided written informed consent. The Clinical Practice Assessment Unit of McGill University coordinated and conducted the trial and collected the data.
Patients
Patients who tested positive for C difficile at participating centers were screened between days 7 to 10 of treatment to identify those meeting eligibility criteria. Inclusion criteria were being 18 years or older and undergoing treatment for a first episode or first recurrence of CDI. CDI was defined as 3 or more episodes of diarrhea in 24 hours with positive results of one of the following: a positive nucleic acid amplification test (NAAT); toxin A/B enzyme immunoassay; or cell cytotoxicity assay. Patients who had less than 3 bowel movements could be included if they had a positive test result in the setting of ileus, toxic megacolon, or pseudomembranous colitis on colonoscopy results.
Exclusion criteria included failure to achieve clinical cure by the end of day 10 (>3 unformed stools per day for 2 days and/or unresolved toxic megacolon); the use of metronidazole monotherapy for more than 3 days; receipt of fidaxomicin, fecal microbiota transplant, or immunoglobulin products for the current episode; previous or current total or subtotal colectomy; severe allergy or intolerance to oral vancomycin; more than 2 episodes of C difficile within 5 years; documented sensorineural hearing loss (other than presbycusis and noise-induced hearing loss); and known or planned pregnancy or breastfeeding. Administrative exclusion criteria are listed in the trial protocol (Supplement 1).
Participants were recruited by local investigators and research personnel after obtaining approval from treating physicians. If a patient met eligibility criteria, trial personnel obtained informed consent and prior to randomization collected baseline data about the patient’s demographic characteristics, comorbid medical conditions, proton pump inhibitor use, and history of concomitant antibiotics. Patients could be recruited in the emergency department, as inpatients, or as outpatients.
Randomization and Interventions
All patients had the length of their initial vancomycin pulse treatment standardized at 14 total days, which is the longest recommended duration in the 2018 Canadian CDI guidelines.^16^ If a patient was receiving more than 125 mg vancomycin orally 4 times per day, the dose was decreased to 125 mg 4 times daily prior to enrollment. Patients were randomly assigned to start the study taper on day 15: 125-mg vancomycin or placebo capsules were given twice daily for 7 days, then once daily for 7 days. This particular taper was chosen as it represents 2 steps of a commonly used 4-week tapering regimen.^17^ Patients underwent randomization using permuted block (random sizes of 2, 4, 6 or 8), which was stratified by the presence or absence of a prior episode of CDI. The allocation sequence was generated by an independent statistician (T.C.L.) using specialized software.^18^ Blinded coded packages of medications were prepared by a central research pharmacy and stored at satellite pharmacies at each site. After the software revealed the randomization code, the packages were dispensed from the pharmacy to the patient either in person or via express courier. Unblinded pharmacists were otherwise not involved in any trial-related activities. The vancomycin and placebo capsules were purchased from Canadian wholesale suppliers. The treating physicians, trial staff, and patients remained unaware of the randomized assignments. Analysis and data safety monitoring were also conducted while blinded.
Outcome Measures
The primary outcome was rCDI between days 15 and 56, with day 1 being the first day that vancomycin treatment of the qualifying episode of CDI began. Recurrence used the same definition of CDI as study inclusion, combined with a requirement for the administration of treatment. Recurrence events were adjudicated in duplicate, with the reviewers (E.G.M., S.E., and T.C.L) blinded to the intervention and disagreement resolved by consensus with a third reviewer.
Secondary outcomes at day 28 consisted of adverse effects, including those leading to treatment cessation. At day 38, we compared recurrence rates to allow direct comparison with the fidaxomicin randomized clinical trials.^9,19^ Secondary outcomes within 90 days included: recurrence as defined above; receipt of fidaxomicin, colectomy, or fecal microbiota transplantation; emergency department visits and readmission to hospital; and all-cause mortality. As potential modifiers of the primary outcome, we also recorded receipt of off-study antibiotics and receipt of vancomycin secondary prophylaxis. Quality of life was assessed by the CDI health-related quality of life Cdiff32 questionnaire^20^ at day 56, to be analyzed and reported in a subsequent report.
Trial Procedures
Patients were evaluated on days 28 and 56 (±3 days) for the primary outcome. Subjects also had weekly check-ins via text message, email, or telephone until day 56, and then every 2 weeks until day 90. Positive responses would trigger a physician visit or in-person trial follow-up as appropriate.
Data Safety and Monitoring Committee Oversight
The first patient was enrolled November 19, 2020. The data safety and monitoring committee (DSMC) met 2 times after enrollment of the first patient to assess the safety and efficacy of the vancomycin taper as compared with the placebo taper regarding the primary outcome, based on prespecified thresholds in the statistical analysis plan (Supplement 1). On November 22, 2024, the DSMC met and following review of the blinded data recommended stopping the trial although the statistical stopping criteria had not been met. Reasons included: (1) the event rates in both arms were lower than anticipated, reducing the power of the study to demonstrate the estimated effect size, and (2) changes to provincial CDI guidelines had repositioned fidaxomicin as first-line therapy for higher-risk patients in the province of Quebec. As the Quebec sites recruited the most patients, it was believed that recruitment to the full sample size was no longer feasible. The DSMC recognized the research question remained scientifically valid and of interest in regions where fidaxomicin was unavailable or not adopted as first-line therapy.
Statistical Analysis
The initial design assumed an event rate of 25% in the control group and 15% in the intervention group based on fidaxomicin randomized clinical trials.^9,19^ With 80% power and an overall 2-sided α = .05, the trial would require 496 (rounded to 500) patients to demonstrate superiority. After the recruitment of 50 patients, the analytic plan was modified to use a bayesian framework on April 3, 2023, prior to completion of study enrollment and before data were locked and blinded for analysis. This allowed for earlier stopping while preserving the overall type I error rate and maximal sample size in response to an update to the Infectious Diseases Society of America guidelines for the treatment of CDI, which were changed to recommend fidaxomicin as first-line therapy in place of vancomycin.^21^ As the study results could have substantial clinical and financial^15^ implications, integrating early stopping rules was salient. We used the adaptr package, version 1.2.0 (R Project for Statistical Computing),^22^ to simulate 50 000 two-armed trials under both the null and alternative hypotheses using the funded 500 patient sample size and interim analyses at 125, 250, and 500 patients. The thresholds for superiority (relative risk [RR], <1.00) were 99.0% at the first analysis and 97.5% at subsequent analyses. A futility analysis was included whereby the trial would be stopped if there was less than a 15% probability of at least a 4% absolute risk reduction (number needed to treat, ≤25). These simulations estimated an overall type I error rate of 5.1% with 72.6% power and a median expected sample size of 250 patients. If the intervention showed a posterior probability of efficacy or futility by crossing a boundary, the DSMC could recommend stopping the trial.
We applied a bayesian framework to all analyses and reported the posterior probabilities for superiority of vancomycin to placebo for the primary and secondary outcomes. The posterior probability determines how likely it is that the new treatment is better, given the available data. The characteristics of the patients at baseline are reported as counts and percentages or, for continuous variables, as medians with IQRs. All binary outcomes were analyzed using a bayesian generalized linear model (binomial family, log link), which yields log RR with 95% bayesian credible intervals (CrI). These were exponentiated to give risk ratios. Priors were minimally informative (N ~ [0, 100^2^]). Stratification was included in the model,^23^ and we ran 4 chains of 50 000 Markov chain Monte Carlo simulations. Exploratory subgroup analyses were assessed in accordance with the prespecified statistical analysis plan included in Supplement 1. Post hoc analysis using restricted mean survival time was suggested by the independent DSMC statistician and is presented in eTable 1 in Supplement 2 using frequentist methods.^24^ Post hoc analyses adjusting for secondary antibiotic exposure and accounting for the site of enrollment were conducted at the request of peer reviewers and are presented in eAppendices 1 and 2 in Supplement 2. Analyses were conducted in Stata, version 17.0 (StataCorp LLC).
Results
Trial Population
A total of 2190 potential participants were screened for inclusion, of whom 275 were recruited and were randomized. Of 275 patients, 139 were randomly assigned to receive vancomycin and 136 to receive placebo (Figure 1). Four and 6 participants, respectively, withdrew from the trial, did not consent to retain their data, leaving 265 patients to be included in the analysis (median age, 63 [IQR, 47-74] years; 138 [52.1%] women and 127 [47.9%] men). Two hundred forty-five included patients (92.5%) were experiencing their first episodes of CDI. Table 1 includes other baseline clinical details.
Study Flow DiagramThe intervention group was randomized to a vancomycin pulse and taper regimen; the placebo group was randomized to a vancomycin pulse regimen. Patients could be excluded for more than 1 reason. IVIG indicates intravenous immunoglobulin.
Primary Outcome
In the intention-to-treat population, 56-day recurrence occurred in 20 of 135 patients (14.8%) patients in the intervention group, as compared with 23 of 130 (17.7%) in the placebo group (adjusted RR, 0.84 [95% CrI, 0.48-1.45]; posterior probability of superiority, 73.8%) (Table 2).
Secondary Outcomes
Most recurrences occurred within the first 2 weeks after stopping vancomycin treatment (Figure 2), with only 1 recurrence (0.7%) during therapy in the vancomycin pulse and taper group. At day 38, corresponding to the follow-up of the fidaxomicin randomized clinical trials,^9,19^ 9 of 135 patients (6.7%) in the vancomycin pulse and taper group had experienced recurrence compared with 20 of 130 (15.4%) in the vancomycin pulse group (adjusted RR, 0.43 [95% CrI, 0.19-0.89]; posterior probability of superiority, 99.0%). Other secondary outcomes are reported in Table 2. The analysis using restricted mean survival time found a modest benefit in favor of the vancomycin pulse and taper regimen of 2.19 (95% CI, 0.51-3.87) days (P = .01) (eTable 1 in Supplement 2**)**. Most recurrences occurred as outpatients, and there was a low rate of emergency department visit or hospitalization in both arms, with only 4 C difficile–related visits.
Kaplan-Meier Curve of Clostridium difficile Infection Recurrence Over TimeThe intervention group was randomized to a vancomycin pulse and taper regimen; the placebo group was randomized to a vancomycin pulse regimen.
Safety
Adverse effects occurred in 15 of 132 patients (11.4%) in the vancomycin pulse and taper group and 13 of 129 (10.1%) in the vancomycin pulse group (Table 3). These were generally mild, with discontinuation due to adverse effects occurring in 2 (1.5%) and 3 (2.3%) patients, respectively.
Subgroup Analyses
Exploratory subgroup analyses are included in the eFigure in Supplement 2 and were generally consistent with the overall trial results. The per protocol analyses are presented in eTable 2 in Supplement 2 and were consistent with the intention-to-treat analysis.
Discussion
This placebo-controlled randomized clinical trial found a 73.8% probability that a 4-week pulse and taper vancomycin regimen reduced the risk of CDI recurrence at day 56 and a 99.0% probability of reduction at day 38. The observed reduction in the probability of superiority from 99.0% at day 38 to 73.4% at day 56 as visualized by the Kaplan-Meier survival curve suggests that some recurrences were delayed as opposed to prevented.
While the initial vancomycin treatment duration for CDI may have been established based on the timing of initial clinical cure,^11^ by 1980 it was obvious that recurrence was a common phenomenon.^25^ It was not until use of fidaxomicin that clinical trials achieved an adequate sample size to adequately study recurrence (as opposed to initial clinical cure).^9^ A possible limitation of the fidaxomicin trials was the shorter follow-up period when compared with the recurrence definition of 56 days of the Society for Healthcare Epidemiology of America and the Infectious Diseases Society of America.^17^ It remains unknown from placebo-controlled trials whether or not fidaxomicin delays or prevents recurrence over a longer time frame. Based on these trials, treatment guidelines^21,26^ have been updated to favor fidaxomicin because of the reduced risk of recurrence when compared with 10 days of vancomycin treatment. Nonetheless, most clinicians worldwide still use vancomycin for the initial treatment of CDI, even in the presence of risk factors for recurrence.^12^ This may be because access to fidaxomicin is not universal and the incremental drug costs remain an important consideration.^15^ The vancomycin pulse and taper regimen could be an option for cases where fidaxomicin is not accessible, and/or where delaying recurrence is important (eg, among more frail, older, patients with more comorbidities). In support of this approach, a recent RCT of a vancomycin pulse and taper regimen vs 10 days of vancomycin for rCDI (first or second episode) presented in abstract form also found a pulse and taper was superior to 10 days of vancomycin for sustained clinical response at day 59.^27^ Importantly, oral vancomycin is considered safe; however antimicrobial resistance has been postulated as a risk of therapy. A propensity-matched cohort study of 82 405 patients treated for CDI with vancomycin or metronidazole did not detect an increased risk of vancomycin-resistant enterococcus in those receiving oral vancomycin.^28^
Limitations
A major limitation of this trial is that it was stopped early, and the power to demonstrate a benefit at day 56 was consequently reduced. It is possible that the benefits shown at day 38 would have translated into a demonstrable residual benefit at day 56 had we achieved the planned sample size. Another limitation was that both initial and recurrence testing was mainly performed by NAAT in patients with clinical symptoms. Some have advocated for 2-stage testing with enzyme-linked immunosorbent assay to reduce false-positive findings vs NAAT alone^29^; however, in a systematic review including 12 737 patients, the 30-day mortality was not significantly different between those who did and did not have positive toxin findings, and furthermore, the treatment of cases with negative enzyme-linked immunosorbent assay toxin-positive findings were associated with a reduction in mortality.^30^ Therefore, the use of NAAT in patients who meet a clinical case definition in combination with strict submission criteria (eg, laboratory rejection of formed specimens) is still considered an acceptable diagnostic standard.^29,31^ Importantly, the placebo-controlled nature of the trial minimized clinical bias with respect to testing and treatment decisions. Another limitation was the use of an initial 14-day pulse of vancomycin therapy in the control group, which may have biased our findings toward the null. Given the time dependence of recurrence,^10^ it is likely that compared with a 10-day pulse of baseline therapy, we would have demonstrated greater probability of superiority. Finally, use of a longer taper may have further delayed or ultimately prevented recurrences. We opted for a 4-week pulse and taper regimen to limit the impact of a longer regimen on the microbiome.
Conclusions
For this randomized clinical trial of patients with first episode or first recurrence of CDI, a 4-week vancomycin pulse and taper regimen had a 73.8% probability of being superior to a 14-day pulse therapy for CDI recurrence at day 56, which may have simply been due to delayed recurrences. This approach may represent a safe and accessible treatment option to delay or prevent early CDI recurrence. Further pragmatic randomized evidence will be essential to optimizing therapy for CDI, particularly a head-to-head clinical trial of a vancomycin pulse and taper regimen vs fidaxomicin with longer term follow-up.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leffler DA, Lamont JT. Clostridium difficile infection. N Engl J Med. 2015;372(16):1539-1548. doi:10.1056/NEJ Mra 1403772 25875259 · doi ↗ · pubmed ↗
- 2The Lancet. A new approach to treating infection. Lancet. 2018;391(10122):714. doi:10.1016/S 0140-6736(18)30320-9 29486930 · doi ↗ · pubmed ↗
- 3Lessa FC, Gould CV, Mc Donald LC. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(suppl 2):S 65-S 70. doi:10.1093/cid/cis 319 22752867 PMC 3388017 · doi ↗ · pubmed ↗
- 4Levy AR, Szabo SM, Lozano-Ortega G, . Incidence and costs of Clostridium difficile infections in Canada. Open Forum Infect Dis. 2015;2(3):ofv 076. doi:10.1093/ofid/ofv 076 26191534 PMC 4503917 · doi ↗ · pubmed ↗
- 5Mc Donald EG, Milligan J, Frenette C, Lee TC. Continuous proton pump inhibitor therapy and the associated risk of recurrent Clostridium difficile infection. JAMA Intern Med. 2015;175(5):784-791. doi:10.1001/jamainternmed.2015.42 25730198 · doi ↗ · pubmed ↗
- 6Sheitoyan-Pesant C, Abou Chakra CN, Pépin J, Marcil-Héguy A, Nault V, Valiquette L. Clinical and healthcare burden of multiple recurrences of Clostridium difficile infection. Clin Infect Dis. 2016;62(5):574-580. doi:10.1093/cid/civ 958 26582748 · doi ↗ · pubmed ↗
- 7Olsen MA, Yan Y, Reske KA, Zilberberg MD, Dubberke ER. Recurrent Clostridium difficile infection is associated with increased mortality. Clin Microbiol Infect. 2015;21(2):164-170. doi:10.1016/j.cmi.2014.08.017 25658560 · doi ↗ · pubmed ↗
- 8Rodrigues R, Barber GE, Ananthakrishnan AN. A comprehensive study of costs associated with recurrent Clostridium difficile infection. Infect Control Hosp Epidemiol. 2017;38(2):196-202. doi:10.1017/ice.2016.246 27817758 · doi ↗ · pubmed ↗