Clinical, social, and economic burdens of schizophrenia in Japan: a targeted literature review
Fumiko Ono, Miyu Okamura

TL;DR
This review explores the clinical, social, and economic impacts of schizophrenia in Japan, highlighting the need for coordinated interventions to reduce patient and caregiver burdens.
Contribution
The study provides a comprehensive analysis of schizophrenia's multifaceted burdens in Japan, emphasizing gaps in stakeholder-driven initiatives.
Findings
Cognitive impairment in schizophrenia is severe, with a Z-score of -2.1 on the Brief Assessment of Cognition in Schizophrenia.
Caregivers face significant productivity losses, with an estimated annual loss of JPY 2.4 million due to presenteeism.
Interventions targeting cognitive function and community cooperation are key to reducing early readmission rates.
Abstract
Schizophrenia is a severe mental disorder with substantial clinical, economic, and humanistic impacts. This targeted literature review evaluated the burden of schizophrenia on patients and caregivers in Japan. Data were collected from PubMed, Ichushi, CiNii, J-STAGE, and the Cochrane Database (2013–2023) and supplementary materials from medical associations, government agencies, and patient organizations (2018–2023). The review focused on epidemiology, clinical management, societal, humanistic, and economic burdens experienced by patients and caregivers. The review identified 156 journal publications, 73 conference proceedings, and 37 additional data sources. Obesity, depression, and type 2 diabetes were highlighted as frequent comorbidities. Cognitive impairment in schizophrenia, assessed by the Brief Assessment of Cognition in Schizophrenia, indicated severe functional deficits with a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
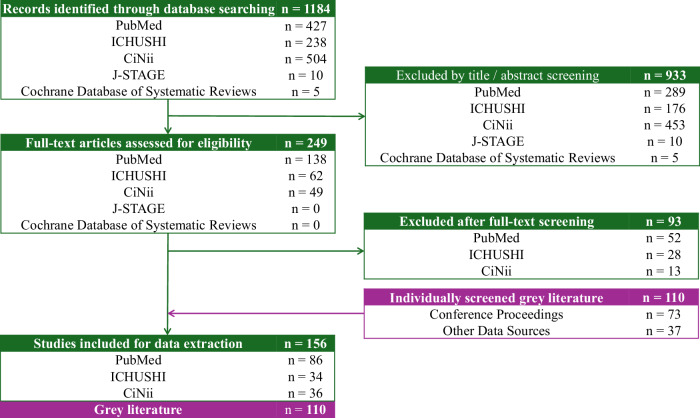 Figure 1
Figure 1- —Nippon Boehringer Ingelheim Co., Ltd.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily Caregiving in Mental Illness · Schizophrenia research and treatment · Mental Health Treatment and Access
Introduction
Schizophrenia is a chronic and severe mental disorder that profoundly affects an individual’s thinking, emotions, and behavior. Globally, approximately 23 million people are estimated to live with schizophrenia^1^, with a lifetime prevalence of approximately 0.3–0.7%^2,3^. This disorder significantly disrupts patients’ lives, creating challenges in interpersonal relationships and employment^4^. These difficulties impose substantial social burdens on patients, including stigma and social exclusion, which may hinder reintegration into society and contribute to increasing unemployment and long-term disability.
In Japan, approximately 0.6% of the population is affected by schizophrenia^5^. The healthcare system is based on universal public insurance, which covers mental healthcare, including outpatient services and some psychological therapies. Psychiatric care remains largely hospital-centered, and long-term hospitalization is common. In recent years, community-based support has gradually expanded, including outreach teams funded by prefectural governments and mental health consultation services at the municipal level^6^. From a policy perspective, Japan’s 8th Medical Care Plan includes provisions for mental health, emphasizing the promotion of community-based care^7^. In addition, the government has issued guidelines for the general public titled “The Mental Health Policy for Workplaces,” which aims to improve mental well-being among workers through preventive measures and support systems^8^.
Despite these institutional frameworks and efforts, significant challenges remain in addressing the burden of schizophrenia and other mental disorders. These include understaffed psychiatric services, inadequate physical healthcare for people with mental illness, slow progress in community transitions, and weak coordination with social services^9^.
This targeted literature review (TLR) aims to comprehensively assess the burdens of schizophrenia in Japan from epidemiological, clinical, societal, economic, and humanistic perspectives. It also seeks to identify stakeholders’ current activities addressing those burdens of disease and unmet needs and to analyze remaining outcome gaps. We hypothesize that despite ongoing efforts, significant gaps remain between stakeholder activities and the multifaceted burdens of schizophrenia.
Methods
Data sources
This TLR adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines^10^, as shown in Fig. 1, and consisted of a biomedical database search and a hand search of gray literature. The database search covering January 1, 2013, to December 31, 2023, was conducted using PubMed, Ichushi, CiNii, J-STAGE, and the Cochrane Database. This 10-year period was chosen to reflect recent trends in research and policy relevant to schizophrenia in Japan.Fig. 1PRISMA flow diagram of study selection process.
A hand search of gray literature was conducted to identify relevant evidence in Japan from conference abstracts, government statistics, and organizational reports covering January 1, 2018, to December 31, 2023. Fifteen gray literature sources were selected based on consultation with a clinical expert. The list of sources is presented in Supplementary Table S1. Additionally, stakeholders’ activities were reviewed to clarify their roles and contributions to schizophrenia-related challenges over the past 5 years.
Inclusion and exclusion criteria
The inclusion and exclusion criteria were defined using the Population, Intervention, Comparators, Outcomes, and Study Design (PICOS) framework as shown in Table 1. This review examined studies on schizophrenia, focusing on patients and caregivers. It included journal and gray literature covering medical treatments, social support, healthcare programs, and policies. The same PICOS criteria were applied to identify stakeholder activities related to schizophrenia.Table 1. Inclusion and exclusion criteria based on the PICOS framework.Inclusion CriteriaPopulation:∙ Patients living with schizophrenia in Japan∙ Individuals caring for patients with schizophrenia in JapanIntervention & Comparators:∙ Any schizophrenia intervention (medical treatment, social support, healthcare program, healthcare policy) or observationOutcome Measures:∙ Epidemiology: prevalence, incidence, comorbidities, complications, mortality, risk factors∙ Clinical Management: treatment options, treatment of comorbidities, nursing care, healthcare resource utilization (HCRU), outcomes/prognosis (including relapse prevention, social functions, daily functions, activities of daily living (ADL), social/personal recovery, participation in society)∙ Society and Welfare: social welfare services, community medicine, peer supporters, stigma, awareness, healthcare policy, multidisciplinary support/team, employment support, housing support, financial support, accessibility to mental health treatment∙ Humanistic: health-related quality of life (HRQoL), quality-adjusted life year (QALY), patient-reported outcomes (e.g., cognitive impairment, disability, disease burden, recovery)∙ Economic: economic burden (direct/indirect costs), productivity impact, quality of life impactStudy Type:Journal published studies:∙ Interventional/empirical studies of healthcare programs∙ Prospective and retrospective observational studies∙ Knowledge, Attitude, and Behavior (KAB) studies∙ Patient/caregiver-centric studies (qualitative studies, surveys, mixed methods, etc.)∙ Economic evaluation studies, economic models∙ Systematic reviews, meta-analyses∙ Treatment guidelines∙ Other reports (think tanks, policy papers)Gray literature:∙ Reports∙ White papers∙ Conference proceedings∙ Statements and press releases from patient associations, medical associations, pharma, etc∙ Published government conference materialsExclusion Criteria∙ Studies not involving patients with schizophrenia or their caregivers∙ Interventions or observations not related to schizophrenia∙ Studies that do not provide data on epidemiology, clinical management, society and welfare, humanistic, or economic outcomes∙ Study design other than described in the inclusion criteria
Data extraction
The data extraction involved reviewing English and Japanese literature from the specified databases and gray literature. The search strategy of databases, with PubMed as a representative example, is outlined in Supplementary Table S2. The review followed PRISMA guidelines, beginning with defining the review’s scope and consensus on search terms. Searches were implemented systematically, and titles and abstracts were screened for relevance. Articles deemed relevant underwent a full-text review, and data were extracted in alignment with the review objectives to ensure the collection of comprehensive and reliable evidence.
For gray literature, conference abstracts were screened like databases, through review of titles and abstracts, followed by data extraction. Other gray literature and stakeholder activities were identified by hand-searching official websites, capturing government, academic, and organizational efforts over the past 5 years to reflect the multifaceted impact of schizophrenia in Japan. These outcomes included epidemiology, clinical management, societal welfare, humanistic outcomes, and economic impact. Each piece of evidence was reviewed and categorized into the most relevant area to facilitate thematic analysis.
Results
Identified data
From database searches, 156 articles were included in the analysis. Additionally, 110 gray literature articles were identified through conference proceedings (n = 73) and other sources (n = 37). The PRISMA flow of the study selection process is shown in Fig. 1. The selected studies are summarized in Tables 2–4. A complete list of all extracted references is provided in Supplementary Document S1. Searches across 15 organizations identified 746 activities related to schizophrenia, as presented in Table 5.Table 2. Summary of published studies stratified by outcome of interest (n = 156).No.^a^Author, yearStudy designTarget populationStudy settingOutcome (category)Outcome (sub-category)1Tsukahara et al. 2023Retrospective observationalPatientHospital(s)EpidemiologyRisk factor2Iwasaki et al. 2023QualitativeCaregiverHospital(s)Clinical managementADL3Sato et al. 2023Quantitative cross-sectionalPatientHospital(s)Clinical managementHealth literacy4Arai et al. 2023Retrospective observationalPatientHospital(s)Clinical managementRisk factor5Yasui-Furukori et al. 2023Retrospective observationalPatientHospital(s)Clinical managementTreatment option6Onitsuka, 2023Quantitative cross-sectionalPatientHospital(s)Clinical managementType of treatment drugs available7Tsuboi et al. 2023Quantitative cross-sectionalCaregiverCommunity-dwellingHumanisticBurden8Hayakawa et al. 2022Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications9Watanabe et al. 2022Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications10Hagane et al. 2022Quantitative cross-sectionalPatientHospital(s)EpidemiologyRisk factor11Nakagawa et al. 2022Prospective observationalPatientCommunity-dwellingClinical managementADL12Kashiwagi et al.^19^Mixed methodPatientDatabase/literatureClinical managementHospitalization rate, Duration of Hospitalization13Higuchi et al. 2022Retrospective observationalPatientDatabase/literatureClinical managementPrescribed drugs14Okada et al. 2022Quantitative cross-sectionalPatientBoth of hospital(s) and community-dwellingClinical managementSocial function15Shimada et al. 2022Quantitative cross-sectionalPatientHospital(s)Clinical managementSocial function16Uchino et al. 2022SurveyPatientHospital(s)Society and welfareAwareness17Baba et al.^5^Quantitative cross-sectionalPatientNDHumanisticHRQoL, WPAI18Ishii et al.^48^QualitativePatientHospital(s)HumanisticQoL19Konishi et al. 2021Retrospective observationalPatientDatabase/literatureEpidemiologyIn-hospital morbidity.20Takahashi et al.^15^Quantitative cross-sectionalPatientDatabase/literatureEpidemiologyMortality21Hori et al. 2021Retrospective observationalPatientHospital(s)Clinical managementCognitive impairment22Kitamura et al. 2021InterventionalBothHospital(s)Clinical managementHospitalization rate23Numata et al. 2021QualitativeCaregiverHospital(s)Clinical managementMedication behavior24Maki et al., 2021Quantitative cross-sectionalCaregiverHospital(s)Clinical managementNursing care25Usami et al. 2021Mixed methodBothHospital(s)Clinical managementNursing care26Toyoda et al. 2021Retrospective observationalPatientDatabase/literatureClinical managementPrescribed drugs27Imazu et al. 2021Retrospective observationalPatientDatabase/literatureClinical managementSide effects/Adverse events28Inagaki et al. 2021SR/Meta-analysisPatientDatabase/literatureClinical managementSide effects/Adverse events29Sato et al. 2021Retrospective observationalPatientBoth of hospital(s) and community-dwellingClinical managementSocial function30Ichinose et al. 2021Retrospective observationalPatientNDClinical managementTreatment option31Koreki et al. 2021Quantitative cross-sectionalPatientHospital(s)Clinical managementType of treatment drugs available32Matsuzaki et al. 2021Retrospective observationalPatientHospital(s)Clinical managementType of treatment drugs available33Arikawa et al.^47^Retrospective observationalPatientHospital(s)Society and welfareFinancial Support34Yasuma et al. 2021Quantitative cross-sectionalCaregiverNDHumanisticBurden35Nagata et al. 2021QualitativePatientCommunity-dwellingHumanisticPRO36Uju et al. 2020Prospective observationalPatientHospital(s)EpidemiologyComorbidities/Complications37Uju et al. 2020Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications38Takahashi et al. 2020Other reviews/reportsPatientDatabase/literatureEpidemiologyComorbidities/Complications39Nishio et al. 2020Retrospective observationalPatientHospital(s)EpidemiologyRisk factor40Inoue et al. 2020SurveyPatientHospital(s)EpidemiologySuicide41Takahashi et al. 2020Quantitative cross-sectionalPatientHospital(s)Clinical managementAdherence, other relevant items42Hosoi et al.^34^SR/Meta-analysisPatientDatabase/literatureClinical managementADL43Nagai et al.^44^Quantitative cross-sectionalPatientHospital(s)Clinical managementDAI-10 score44Ogawa et al. 2020SurveyPatientHospital(s)Clinical managementDuration of hospitalization45Ichimura et al. 2020Retrospective observationalPatientHospital(s)Clinical managementOther relevant items46Hayashi et al. 2020InterventionalPatientHospital(s)Clinical managementPsychiatric rehabilitation47Iwata et al. 2020Retrospective observationalPatientDatabase/literatureClinical managementType of treatment drug available48Kamei et al. 2020SurveyPatientHospital(s)Clinical managementType of treatment drugs available49Iwamoto et al. 2020QualitativeCaregiverHospital(s)Society and welfarePeer supporter50Yoshida et al. 2020QualitativePatientCommunity-dwellingSociety and welfarePeer supporter51Shimada et al. 2020Retrospective observationalPatientBoth of hospital(s) and community-dwellingEconomicHospitalization costs52Kasahara-Kiritani, 2020Economic evaluation studyPatientNDEconomicTotal costs53Toriyama et al. 2019Retrospective observationalPatientNDEpidemiologySide effects/Adverse events54Kaneko et al. 2019Quantitative cross-sectionalPatientHospital(s)Clinical managementFunctional Capacity55Nakamura et al. 2019Economic evaluation studyPatientNDClinical managementHospitalization rate56Doi et al. 2019Retrospective observationalPatientHospital(s)Clinical managementType of drugs57Sugawara et al.^49^Quantitative cross-sectionalPatientHospital(s)Clinical managementType of treatment drugs available58Shiosawa et al. 2019Quantitative cross-sectionalCaregiverCommunity-dwellingSociety and welfarePeer supporter59Araki et al. 2019SurveyCaregiverHospital(s)Society and welfarePeer supporter60Kunizuka et al.^37^Retrospective observationalPatientHospital(s)HumanisticCognitive impairment61Watanabe et al. 2019SurveyPatientHospital(s)HumanisticPRO62Sugawara et al. 2018SR/Meta-analysisPatientDatabase/literatureEpidemiologyComorbidities/Complications63Hattori et al.^11^Retrospective observationalPatientHospital(s)EpidemiologyMortality64Tanimoto et al. 2018Retrospective observationalPatientHospital(s)EpidemiologySuicide attempt65Ebisu et al. 2018Retrospective observationalPatientHospital(s)Clinical managementDuration of hospitalization66Matsumoto et al. 2018QualitativeCaregiverHospital(s)Clinical managementNursing care67Haga et al.^17^Retrospective observationalPatientHospital(s)Clinical managementTreatment option, risk factor68Inada et al. 2018Retrospective observationalPatientHospital(s)Clinical managementType of treatment drugs available69Maki et al. 2018QualitativeCaregiverHospital(s)Society and welfarePeer supporter70Matsumoto et al. 2018QualitativeCaregiverCommunity-dwellingSociety and welfareSupport71Fujino et al. 2018SurveyPatientHospital(s)HumanisticCognitive impairment72Kageyama et al., 2018SurveyCaregiverCommunity-dwellingHumanisticCRO73Kageyama et al, 2018SurveyCaregiverCommunity-dwellingHumanisticPRO74Kasuga et al. 2018QualitativePatientCommunity-dwellingHumanisticPRO75Sugawara et al. 2018QualitativePatientHospital(s)HumanisticPRO76Kamiura et al.^60^Economic evaluation studyPatientNDEconomicICER77Sruamsiri et al., 2018Economic evaluation studyCaregiverDatabase/literatureEconomicProductivity78Omi et al. 2017Retrospective observationalPatientHospital(s)Clinical managementDuration of hospitalization79Uchida et al. 2017Quantitative cross-sectionalPatientHospital(s)Clinical managementDuration of hospitalization80Cheung et al.^18^Retrospective observationalPatientDatabase/literatureClinical managementHospitalization rate, ER visit81Hatano et al. 2017SurveyPatientHospital(s)Clinical managementSide effects/Adverse events82Miyauchi et al. 2017Retrospective observationalPatientHospital(s)Clinical managementType of treatment drugs available83Narita et al. 2017Mixed methodPatientCommunity-dwellingSociety and welfareCommunity medicine84Niimura et al.^46^Quantitative cross-sectionalPatientBoth of hospital(s) and community-dwellingSociety and welfareSocial welfare service85Fujino et al.^36^SurveyPatientHospital(s)HumanisticCognitive impairment86Kiriyama et al. 2017Mixed methodBothHospital(s)HumanisticPRO87Setoguchi et al. 2017SR/Meta-analysisPatientDatabase/literatureHumanisticPRO88Fujimoto et al. 2017SurveyPatientCommunity-dwellingHumanisticPRO89Nakamura et al.^61^Economic evaluation studyPatientHospital(s)EconomicTotal costs90Sado et al.^31^Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications91Sugai et al.^16^Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications92Sugai et al.^16^Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications93Ishikawa et al.^13^Retrospective observationalPatientHospital(s)EpidemiologyMortality94Sugawara et al. 2016Quantitative cross-sectionalPatientHospital(s)EpidemiologyRisk factor95Yoshida et al.^51^Quantitative cross-sectionalPatientBoth of hospital(s) and community-dwellingEpidemiologyRisk factor96Tarutani et al. 2016SurveyPatientHospital(s)Clinical managementAdherence97Shimada et al. 2016Retrospective observationalPatientHospital(s)Clinical managementHospitalization rate98Takeuchi et al, 2016Quantitative cross-sectionalBothHospital(s)Clinical managementOther relevant items99Akiyama et al. 2016Other reviews/reportsPatientHospital(s)Clinical managementSocial function100Hashimoto et al. 2016Quantitative cross-sectionalPatientHospital(s)Clinical managementType of treatment drugs available101Kageyama et al., 2016SurveyCaregiverCommunity-dwellingHumanisticCRO102Niimura et al.^53^QualitativePatientHospital(s)HumanisticPRO103Iinuma et al. 2016Mixed methodPatientHospital(s)HumanisticPRO104Kawanabe et al. 2016SurveyPatientHospital(s)HumanisticQoL105Hashimoto et al. 2016Other reviews/reportsPatientHospital(s)EconomicMedicine costs106Ito et al. 2015Quantitative cross-sectionalPatientBoth of hospital(s) and community-dwellingEpidemiologyComorbidities/Complications107Kanzaki et al. 2015Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications108Sugai et al. 2015Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications109Nakamura et al. 2015SurveyPatientHospital(s)EpidemiologyComorbidities/Complications110Ikeda et al. 2020Prospective observationalPatientHospital(s)Clinical managementDuration of hospitalization111Tachimori et al. 2015Retrospective observationalPatientHospital(s)Clinical managementDuration of hospitalization112Kuwabara et al.^21^Retrospective observationalPatientDatabase/literatureClinical managementHospitalization rate113Takahashi et al. 2015Prospective observationalPatientHospital(s)Clinical managementHospitalization rate (remission)114Sumiyoshi et al. 2015Quantitative cross-sectionalPatientHospital(s)Clinical managementSocial function115Sasamoto et al. 2015QualitativeCaregiverHospital(s)Society and welfareMultidisciplinary support116Yamada^42^SurveyPatientHospital(s)Society and welfareStigma117Sasaki et al. 2015Mixed methodPatientHospital(s)HumanisticPRO118Nagasawa et al. 2015Mixed methodPatientHospital(s)HumanisticPRO119Kimbara et al.^12^Retrospective observationalPatientHospital(s)EpidemiologyComorbidities/Complications120Imai et al. 2014Other reviews/reportsPatientHospital(s)EpidemiologyComorbidities/Complications121Sugawara et al. 2014Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications122Suzuki et al. 2014Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications123Harada et al. 2014Other reviews/reportsPatientHospital(s)EpidemiologySuicide attempt124Ikeshita et al. 2014Retrospective observationalPatientHospital(s)EpidemiologySuicide attempt125Ishii et al. 2014Other reviews/reportsPatientHospital(s)EpidemiologySuicide attempt126Teraishi et al, 2014SurveyPatientHospital(s)EpidemiologySuicide attempt127Sugibayashi et al.^20^Quantitative cross-sectionalPatientHospital(s)Clinical managementADL128Arai^14^SurveyBothHospital(s)Clinical managementNursing care129Ochiai et al. 2014Retrospective observationalPatientDatabase/literatureClinical managementPrescribed drugs130Omi et al. 2014SurveyPatientHospital(s)Clinical managementSocial function131Inoue et al. 2014Retrospective observationalPatientHospital(s)Clinical managementSocial function132Tamura et al.^54^QualitativePatientHospital(s)HumanisticPRO133Nakamura et al. 2014Quantitative cross-sectionalPatientCommunity-dwellingHumanisticQoL134Inamura et al. 2013Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications135Suzuki et al. 2013Retrospective observationalPatientHospital(s)EpidemiologyComorbidities/Complications136Suzuki et al. 2013Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications137Umene-Nakano et al. 2013Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications138Inamura, 2013Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications139Sugawara et al.^50^Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications, HRQoL140Saito et al.^32^Retrospective observationalPatientHospital(s)EpidemiologyRisk factor141Kimura et al. 2013Retrospective observationalPatientHospital(s)EpidemiologySuicide attempt142Saito et al.^32^Retrospective observationalPatientHospital(s)Clinical managementADL143Tanioka et al. 2013Retrospective observationalPatientHospital(s)Clinical managementDuration of hospitalization144Sato et al. 2013QualitativePatientHospital(s)Clinical managementDuration of hospitalization145Tamasato, 2013QualitativePatientHospital(s)Clinical managementNursing care146Onose et al. 2013QualitativePatientHospital(s)Clinical managementSocial and personal recovery147Takahashi et al. 2013Prospective observationalPatientHospital(s)Clinical managementType of treatment drugs available148Okumura et al. 2013Retrospective observationalPatientDatabase/literatureClinical managementType of treatment drugs available149Kurosawa et al. 2013Retrospective observationalPatientDatabase/literatureClinical managementType of treatment drugs available150Yoshimura, 2013QualitativeCaregiverHospital(s)Society and welfarePeer supporter151Iwasaki et al. 2013QualitativeCaregiverCommunity-dwellingSociety and welfarePeer supporter152Kagawa et al. 2013QualitativeCaregiverHospital(s)Society and welfarePeer supporter153Fujita et al. 2013InterventionalPatientHospital(s)HumanisticHealth state utitlities154Koyama, 2013Mixed methodPatientCommunity-dwellingHumanisticPRO155Kikuchi, 2013QualitativePatientCommunity-dwellingHumanisticPRO156Sado et al.^59^Economic evaluation studyPatientNDEconomicTotal costsNA not applicable, ND no data, ADL activities of daily living, CRO caregiver-reported outcome, DAI-10 drug attitude inventory-10, ER emergency room, HRQoL health-related quality of life, ICER incremental cost-effectiveness ratio, PRO patient-reported outcome, QoL quality of life, WPAI Work Productivity and Activity Impairment.^a^Note: All literature sources referenced in this table can be found in Supplementary Document S1.Table 3. Summary of conference abstracts stratified by outcome of interest (n = 73).No.^a^Author, yearStudy designTarget populationStudy settingOutcome (category)Outcome (sub-category)157Kamei et al. 2023Retrospective observationalPatientHospital(s)EpidemiologyComorbidities/Complications158Goto et al.^27^QualitativePatientCommunity-dwellingClinical managementBurden of treatment159Ida et al. 2023Retrospective observationalPatientHospital(s)Clinical managementManagement of comorbidities/complications160Mochizuki et al. 2023QualitativePatientCommunity-dwellingClinical managementNursing care161Narita et al. 2023Retrospective observationalPatientHospital(s)Clinical managementPrescription162Matsuda et al. 2023Retrospective observationalPatientHospital(s)Clinical managementPrescription163Takagi et al. 2023Quantitative cross-sectionalCaregiverCommunity-dwellingHumanisticCRO164Watabe, 2023Quantitative cross-sectionalCaregiverCommunity-dwellingHumanisticCRO165Nakai et al. 2023QualitativePatientCommunity-dwellingHumanisticPRO166Tsutsumi et al. 2022Retrospective observationalPatientHospital(s)EpidemiologyComorbidities/Complications167Fukushima et al. 2022SurveyPatientNDClinical managementHCRU168Nakamura et al. 2022SurveyPatientNDClinical managementPrescription169Shimada et al. 2022Quantitative cross-sectionalPatientHospital(s)Clinical managementSocial function170Takemura et al. 2022Other reviews/reportsPatientHospital(s)Clinical managementTreatment option171Kobatake et al. 2022Other reviews/reportsPatientDatabase/literatureSociety and welfareSelf-stigma172Hiyama et al. 2022QualitativeCaregiverCommunity-dwellingSociety and welfareSupport173Nishi et al. 2022Quantitative cross-sectionalPatientCommunity-dwellingHumanisticPRO174Fukuda et al. 2022Quantitative cross-sectionalPatientCommunity-dwellingHumanisticPRO175Suzuki et al. 2022Quantitative cross-sectionalPatientHospital(s)HumanisticPRO176Watanabe et al. 2022Quantitative cross-sectionalPatientHospital(s)HumanisticPRO177Yokota et al. 2021Retrospective observationalPatientHospital(s)EpidemiologyComorbidities/Complications178Hirota et al. 2021Retrospective observationalPatientNDClinical managementBurden of treatment179Taniguchi et al.^29^Retrospective observationalPatientNDClinical managementBurden of treatment180Kida et al.^22^Retrospective observationalPatientHospital(s)Clinical managementManagement of comorbidities/complications181Ono et al. 2021Retrospective observationalPatientHospital(s)Clinical managementMaternal-fetal management182Suzuki et al. 2021QualitativeCaregiverHospital(s)Clinical managementNursing care183Arai et al. 2021QualitativeCaregiverHospital(s)Clinical managementNursing care184Kimura^56^Other reviews/reportsCaregiverDatabase/literatureClinical managementNursing care185Nishiyama et al. 2021Retrospective observationalPatientHospital(s)Clinical managementPrescription186Furuhata et al.^26^SurveyPatientHospital(s)Clinical managementPrescription187Moriwaki et al.^39^Retrospective observationalPatientNDClinical managementRelationship between COVID-19 and mental illness188Hanawa et al.^40^Retrospective observationalPatientNDClinical managementRelationship between COVID-19 and mental illness189Inagawa et al. 2021InterventionalPatientNDClinical managementTreatment option190Funai et al. 2021InterventionalPatientHospital(s)Clinical managementTreatment option191Inuyama et al. 2021Retrospective observationalPatientNDClinical managementTreatment option192Kojima et al.^55^QualitativeCaregiverCommunity-dwellingHumanisticCRO193Kimura et al.^56^QualitativeCaregiverNDHumanisticCRO194Koyama et al. 2021Quantitative cross-sectionalPatientHospital(s)HumanisticPRO195Ogata et al. 2021Quantitative cross-sectionalPatientBoth of hospital(s) and community-dwellingHumanisticPRO196Yamaguchi et al. 2021Quantitative cross-sectionalPatientHospital(s)HumanisticPRO197Ishii, 2020Prospective observationalPatientHospital(s)Clinical managementBurden of treatment198Sugai et al.^23^Prospective observationalPatientHospital(s)Clinical managementManagement of comorbidities/complications199Inakuma et al.^24^Retrospective observationalPatientHospital(s)Clinical managementManagement of comorbidities/complications200Akasaka et al. 2020Quantitative cross-sectionalPatientNDClinical managementManagement of comorbidities/complications201Kobayashi et al. 2020Retrospective observationalPatientHospital(s)Clinical managementMaternal-fetal management202Aoki et al. 2020Retrospective observationalPatientNDClinical managementTreatment option203Tanaka, 2020Retrospective observationalPatientHospital(s)Clinical managementTreatment option204Kitamura et al. 2019SurveyPatientHospital(s)EpidemiologyComorbidities/Complications205Matsui et al. 2019Retrospective observationalPatientDatabase/literatureEpidemiologyComorbidities/Complications206Onda et al. 2019SurveyPatientHospital(s)EpidemiologyComorbidities/Complications207Sugai et al. 2019Quantitative cross-sectionalPatientHospital(s)EpidemiologyComorbidities/Complications208Takahashi et al. 2019SurveyPatientNDClinical managementHCRU209Masaki et al. 2019SurveyPatientHospital(s)Clinical managementHCRU210Fukuda et al. 2019Quantitative cross-sectionalPatientHospital(s)Clinical managementHCRU211Suzuki et al. 2019Retrospective observationalPatientHospital(s)Clinical managementLifestyle management212Fujiwara et al. 2019Prospective observationalPatientHospital(s)Clinical managementLifestyle management213Kusumi et al.^25^Prospective observationalPatientDatabase/literatureClinical managementManagement of comorbidities/complications214Ono et al. 2019Quantitative cross-sectionalPatientHospital(s)Clinical managementManagement of comorbidities/complications215Otake et al. 2019Quantitative cross-sectionalPatientHospital(s)Clinical managementManagement of comorbidities/complications216Arai et al. 2019QualitativeCaregiverHospital(s)Clinical managementNursing care217Ishii, 2019QualitativeCaregiverHospital(s)Clinical managementNursing care218Kikuchi et al. 2019Retrospective observationalPatientHospital(s)Clinical managementPrescription219Ozeki et al. 2019Retrospective observationalPatientNDClinical managementPrevention of relapse220Watabe, 2019InterventionalCaregiverHospital(s)Clinical managementTreatment option221Naganuma et al. 2019Other reviews/reportsPatientHospital(s)Clinical managementTreatment option222Sakayori et al. 2019SurveyPatientHospital(s)Clinical managementTreatment option223Kusuno, 2019Other reviews/reportsPatientCommunity-dwellingSociety and welfareAccessibility to treatment of mental health224Nemoto et al. 2019Prospective observationalPatientNDSociety and welfareSocial function225Imaeda et al. 2019QualitativePatientBoth of hospital(s) and community-dwellingSociety and welfareSupport226Yabuta^57^QualitativeCaregiverCommunity-dwellingHumanisticCRO227Fujisawa^58^QualitativeCaregiverCommunity-dwellingHumanisticCRO228Moriguchi et al. 2019Quantitative cross-sectionalPatientCommunity-dwellingHumanisticPRO229Nakamura et al. 2019Quantitative cross-sectionalPatientCommunity-dwellingHumanisticPRONA not applicable, ND no data, COVID-19 Coronavirus Disease 2019, CRO caregiver-reported outcome, HCRU healthcare resource utilization, PRO patient-reported outcome.^a^Note: All literature sources referenced in this table can be found in Supplementary Document S1.Table 4. Summary of other source stratified by outcome of interest (n = 37).No.^a^Author/Publisher, yearType of literatureData sourceTarget populationOutcome (category)Outcome (sub-category)230MHLW, 2023Government statisticsMHLWPatientClinical managementNumber of hospitalized patients231NFAFMJ, 2023ReportNFAFMJCaregiverHumanisticCRO232MHLW, 2023Government statisticsMHLWPatientEconomicMedical fee233MHLW, 2022Government statisticsMHLWPatientEpidemiologyPatient population234MHLW, 2022Government statisticsMHLWPatientEpidemiologyPatient population235MHLW, 2022Government statisticsMHLWPatientEpidemiologyPatient population236MHLW, 2022Government statisticsMHLWPatientEpidemiologyPatient population237MHLW, 2022Government statisticsMHLWPatientClinical managementMedical fee238MHLW, 2022Government statisticsMHLWPatientClinical managementNumber of hospitalized patients239MHLW, 2023Government statisticsMHLWPatientClinical managementNursing care240MHLW, 2022Government statisticsMHLWPatientClinical managementTreatment rate241MHLW, 2022Government statisticsMHLWPatientClinical managementTreatment rate242MHLW, 2022Government statisticsMHLWPatientEconomicMedical fee243MHLW, 2021Government statisticsMHLWPatientClinical managementHCRU244MHLW, 2021Government statisticsMHLWPatientClinical managementHCRU245MHLW, 2021Government statisticsMHLWPatientClinical managementHCRU246MHLW, 2021Government statisticsMHLWPatientClinical managementHCRU247MHLW, 2021Government statisticsMHLWPatientClinical managementHCRU248MHLW, 2021Government statisticsMHLWPatientClinical managementMedical fee249MHLW, 2021Government statisticsMHLWPatientClinical managementNumber of hospitalized patients250MHLW, 2021Government statisticsMHLWPatientEconomicMedical expenses251MHLW, 2021Government statisticsMHLWPatientEconomicMedical fee252MHLW, 2020Government statisticsMHLWPatientClinical managementHCRU253MHLW, 2020Government statisticsMHLWPatientClinical managementHCRU254MHLW, 2020Government statisticsMHLWPatientClinical managementHCRU255MHLW, 2020Government statisticsMHLWPatientClinical managementHCRU256MHLW, 2020Government statisticsMHLWPatientClinical managementHCRU257MHLW, 2020Government statisticsMHLWPatientClinical managementHCRU258MHLW, 2020Government statisticsMHLWPatientClinical managementMedical fee259MHLW, 2020Government statisticsMHLWPatientClinical managementNumber of hospitalized patients260MHLW, 2020Government statisticsMHLWPatientClinical managementNursing care261MHLW, 2020Government statisticsMHLWPatientEconomicMedical expenses262MHLW, 2020Government statisticsMHLWPatientEconomicMedical fee263MHLW, 2019Government statisticsMHLWPatientClinical managementMedical fee264MHLW, 2019Government statisticsMHLWPatientEconomicMedical expenses265MHLW, 2018Government statisticsMHLWPatientClinical managementMedical fee266MHLW, 2018Government statisticsMHLWPatientEconomicMedical expensesCRO caregiver-reported outcome, HCRU healthcare resource utilization, MHLW Ministry of Health, Labor, and Welfare, NFAFMJ The National Federation of Associations of Families with the Mental Illness in Japan.^a^Note: All literature sources referenced in this table can be found in Supplementary Document S1.Table 5. Overview of stakeholder activities.StakeholderType of activities, hit numbers (%)Academic/ResearchEducation/TrainingPublicationInformation/CommunicationPolicy/AdvocacyCommunity support and servicesTotalJapanese Society of Schizophrenia Research001180019Japanese Society of Psychiatry and Neurology0000000Japan Academy of Psychiatric and Mental Health Nursing60070013Japanese Society for Social Psychiatry0020002Japanese Society of Neuropsychopharmacology013110015Japanese Association for Emergency Psychiatry3010004National Center of Neurology and Psychiatry2940250058Evidence-based Information site on community lives for people with mental illness040220026Health and Global Policy Institute0001102Ministry of Health, Labor, and Welfare (MHLW)110071320150The National Federation of Associations of Families with Mental Illness in Japan10082011Porque (Organization of Persons with Psychosocial Disabilities)014352042COMHBO (Community Mental Health and Welfare Organization)000100010Smile Navigator000140014Kokoro-share0007007Note: Academic/Research: overall academic and research activities, including research, conferences, presentations, and other activities promoting collaboration between organizations. Education/Training: overall activities related to education and training, including school education. Publication: overall activities of publishing printed materials, like association journals. Information/Communication: overall activities related to providing information, including outreaching, hosting lectures, and organizing symposiums. Policy/Advocacy: overall activities related to policy, including advocacy and activities targeting specific policies. Community support and services: overall activities related to support, such as building networks, disability welfare services, community life support, counseling support, and work support.
Characteristics of included studies
Most studies focused on patients (n = 132), followed by caregivers (n = 19) and both (n = 5). Clinical burden was most common (n = 66), followed by epidemiology (n = 41), humanistic burden (n = 27), societal and welfare burden (n = 15), and economic burden (n = 7). Publications were from 2013 to 2017 (n = 79) and 2018 to 2023 (n = 77). Since the peak in 2013 (n = 23), the number of publications has shown a declining trend. In gray literature, conference abstracts mainly targeted patients (n = 60), focusing on clinical management (n = 46), humanistic burden (n = 16), epidemiology (n = 7), and societal and welfare burden (n = 4). Publication years ranged from 2019 to 2023. Other sources also targeted patients (n = 35), addressing clinical management (n = 24), economic burden (n = 8), epidemiology (n = 4), and humanistic burden (n = 1).
Epidemiology
A self-reported online survey from the National Health and Wellness Survey reported a prevalence of 0.59%, primarily among individuals aged 18–64 (89.3%)^5^. Five studies reported data on mortality^11–15^. A single-center study by Hattori et al. followed up 59 patients (mean age 64.9) for 10 years; 11 died (mean age 70.6)^11^. Kimbara et al. examined 134 inpatients (mean age 63); 12 died over 5 years, nearly half (n = 7) from pneumonia^12^. Ishikawa et al. used data from the Japanese Diagnosis Procedure Combination (DPC) database to assess schizophrenia and cancer stages in acute hospitals; the 30-day in-hospital mortality rate of cancer patients with schizophrenia was 4.2%^13^. Arai’s dual-center study reported that all 16 patients with schizophrenia and cancer died within a year of the diagnosis; diagnoses were at advanced stages^14^. Takahashi et al. reported in-hospital mortality rates of 12.9% (acute myocardial infarction: AMI) and 5.8% (pulmonary embolism) among schizophrenia patients using DPC data^15^.
Comorbidities or complications, such as obesity, hypertension, depression, congestive heart failure, and type 2 diabetes mellitus, were consistently highlighted. A multi-center study found hypertension in 30.5% of outpatients and 19.9% of inpatients; diabetes in 16.8% and 7.1%, respectively^16^. A single-center study by Haga et al. identified pneumonia risk factors: age, underweight status, smoking habit, use of atypical antipsychotics, and high doses^17^. A database study by Cheung et al. on medical information from acute care hospitals in Japan reported that 17.2% of 45,201 schizophrenia patients were also diagnosed with depression^18^.
Clinical management burden
The database study by Cheung et al. (study period between July 2013 and June 2015) reported a mean of 2.0 hospitalizations among 45,201 schizophrenia patients^18^. Similarly, Kashiwagi et al. analyzed data from the Cognitive Genetics Collaborative Research Organization database (study period: October 2005 and October 2019) and found patients with a violence history had a mean of 2.3 hospitalizations vs. 1.2 without violence^19^. Furthermore, hospitalization duration varied widely, from 20.7 days to 13,833.5 days. Sugibayashi et al. reported a mean of 3242.1 days among 8379 inpatients (4452 males, 2691 over 65 years old)^20^. A database study by Kuwabara analyzed 657 patients (222 males) from MDV; the mean index hospitalization was 84.3 days^21^.
Studies on comorbidities and complications often explored links between antipsychotic drug prescription and comorbidities and complications^22–25^. Sugai et al. found that increased prescriptions worsened body mass index, systolic blood pressure, low-density lipoprotein cholesterol, and fasting blood sugar values. They also examined prescribing practices and medication adherence^23^. Furuhata et al. found multiple sleep medications were associated with age, polypharmacy, and mood stabilizers^26^. Other studies involved medication adherence, challenges of isolation and physical restraint in psychiatric wards, and challenges in physical comorbidity wards^27–30^.
Six studies reported activities of daily living (ADL)^20,31–35^. A single-center study found that among 770 patients, 513 had mild, 137 moderate, and 81 severe ADL disorders^31^. In another single-center study, Saito et al. found that 17.6% of 272 schizophrenia patients with dysphagia were “independent” in daily activities^32^.
Three studies examined cognitive impairment^36–38^. A multi-center study by Fujino et al. reported that the average cognitive impairment score of patients was −16.3, lower than the pivotal score of −10, significantly lower than healthy controls. The score was calculated as the difference between the current Full-Scale Intelligence Quotient (IQ) assessed by the Wechsler Adult Intelligence Scale - Second Edition and the premorbid IQ estimated using the Japanese Adult Reading Test - 25^36^. A single-center study by Kunizuka et al. found a composite z-score of −2.1 using the Brief Assessment of Cognition in Schizophrenia-Japanese version^37^. Hori et al. found composite z-scores of −0.7, −1.1, −1.5, and −1.8 among patients with 0, 1, 2, and 3 hospitalizations, respectively^38^.
According to three gray literature articles, the COVID-19 pandemic had notable impacts on schizophrenia patients. Moriwaki et al. reported increased self-harm and suicidal ideation among hospitalized patients in 2020, although treatment outcomes remained stable and hospitalization duration shortened^39^. Hanawa et al. identified schizophrenia among suicide attempt diagnoses related to COVID-19-related anxiety and economic stress^40^. Fukushima et al. reported that in an acute psychiatric ward, a 23% increase in discharged schizophrenia patients in 2020 (from 92 to 113), while the average stay decreased by about 10 days to 58 days^41^.
Society and welfare burden
Yamada assessed self-stigma using the Perceived Devaluation Discrimination (PDD) scale developed a self-reported scale with 12 items to evaluate perceived stigma, discrimination, stereotyping, and social rejection^42,43^. The scale ranges from 12 to 60, with higher scores indicating lower levels of stigma. Among 97 inpatients, the mean PDD score was 30.5, lower than those reported in two other studies (mean scores: 32.6 and 31.5). Nagai et al. conducted a cross-sectional study on VAGUS to assess schizophrenia awareness among 148 outpatients, reporting a mean score of 6.6 (standard deviation of 1.5)^44^. VAGUS is a standardized tool to assess how emotional conditions might influence behavior and decision-making, consisting of 10 self-report and five clinician-rated questions^45^. A cross-sectional study by Niimura et al. using a patient survey reported a financial burden. Among 21,101 patients with less than 80 days of hospitalization, 19.4% received public assistance. Similarly, among 21,167 patients with over 80 days of hospitalization, 19.1% used public assistance^46^. A single-center study by Arikawa et al. reported that 151 out of 437 schizophrenia patients used medical expenses for services and support for disabilities. The study mentioned that financial support improves persistence of outpatient treatment for patients with schizophrenia^47^.
Humanistic burden
Among six studies^5,48–52^, four quality of life (QoL) assessment tools were identified: EuroQol 5-Dimension (EQ-5D), the Japanese version of the Schizophrenia Quality of Life Scale (JSQLS), MOS 36-Item Short-Form Health Survey (SF-36) v2, and SF-12v2. Baba et al. evaluated Health-related Quality of Life (HRQoL) of schizophrenia patients using SF-12v2, EQ-5D Index, and EQ-5D VAS, dividing patients based on their Patient Health Questionnaire-9 (PHQ-9) scores (<10 vs. ≥10). Patients with PHQ-9 < 10 showed high HRQoL, with EQ-5D VAS scores of 67.8, while those with PHQ-9 ≥ 10 had moderate HRQoL with EQ-5D VAS scores of 44.3. SF-12v2 scores indicated slightly below average physical functioning for both groups, with better mental health for those with PHQ-9 scores < 10^5^. Another study by Ishii et al. with 50 patients used JSQLS to evaluate QoL, with a mean of 45.0 for psychosocial, 47.3 for motivation and energy, and 34.9 for symptoms and side effects scales^48^. The study also reported the finding that depressive symptoms are key predictors of subjective QoL, highlighting the importance of addressing depression to improve overall well-being in schizophrenia patients.
A qualitative study by Niimura et al. involving 18 discharged patients identified challenges such as “separating life as an inpatient from community life,” including dissatisfaction with inpatient care and a lack of ability to coordinate post-discharge life. Patients reported dissatisfaction with the admission process and treatment in protection rooms, and challenges in managing life after discharge^53^. Another qualitative study by Tamura et al. with three patients assessed the impact of clozapine treatment, identifying themes like anxiety about a new medication, the hardship of frequent outpatient visits, and joy of symptom attenuation post-treatment^54^. Qualitative studies also highlighted difficulties faced by caregivers, particularly parents and siblings, in supporting patients. Parents struggled to accept their child’s illness and were anxious about their child’s job continuity despite regular employment^55–58^.
Economic burden
An economic evaluation study estimated the cost of schizophrenia in 2008 from a societal perspective. Direct, indirect, and total costs were Japanese yen (JPY) 770.0 billion (US dollars [USD] 5.1 billion), JPY 2.0 trillion (USD 13.2 billion), and JPY 2.8 trillion (USD 18.3 billion), respectively^59^. Direct costs included social services and healthcare under health insurance, involuntary admission, medical care, and supervision act costs. Indirect costs included morbidity costs (e.g., loss of income due to hospitalization and hospital visits) and mortality costs (future income lost due to early death due to a certain illness). Inpatient and outpatient costs were JPY 602.8 billion (USD 4.0 billion) and 148.0 billion (USD 1.0 billion), respectively^59^. Kamiura et al. estimated the cost-effectiveness of oral medication by hazard ratios for hospitalization compared to LAI. They found the largest reduction of incremental cost-effectiveness ratios between hazard ratios of 1.1 and 2.0^60^. Baba et al. assessed the productivity loss of schizophrenia patients using the Work Productivity and Activity Impairment (WPAI) tool. The mean total activity impairment was 22.8 for PHQ-9 scores <10 and 53.6 for scores ≥10, indicating moderate to significant impairment^5^. Nakamura et al. estimated productivity losses due to unemployment or premature death, totaling JPY 3990 million (USD 26.3 million). 4146 patients’ labor was lost due to unemployment, and 151 patients due to premature death^61^. For caregivers, Sruamsiri et al. analyzed productivity losses among caregivers. Using the WPAI questionnaire with 171 caregivers, they found absenteeism at 4.7% and presenteeism at 25.0%, resulting in per capita annual productivity costs of JPY 2.4 million (USD 16.0 thousand), with presenteeism accounting for 97% (JPY 2.4 million [USD 15.6 thousand]). They also calculated annual productivity losses due to job resignation for caregiving at JPY 1.3 million (USD 8.6 thousand), leading to a total annual productivity loss of JPY 2.4 million (USD 15.8 thousand)^62^.
The economic outcomes reported in Japanese yen are accompanied by their equivalent values in USD in parentheses, calculated using the exchange rate as of February 28, 2025, which represents the conversion rate at the time of writing this manuscript. The rate applied for conversion was 1 JPY = 0.0066 USD.
Stakeholder activities
Stakeholder activities were categorized into six main types: academic and research activities, education and training, publication, information and communication, policy and advocacy, and community support and services. The Ministry of Health, Labour, and Welfare (MHLW) was the most active organization, with 150 activities, predominantly in policy and advocacy. Efforts also included research on clozapine and medical fees. The National Center of Neurology and Psychiatry was the second-most active organization, with 58 activities focused on academic research, information dissemination, and other areas. Also, they led educational efforts for psychiatrists through the Effectiveness of GUIdeline for Dissemination and Education in psychiatric treatment (EGUIDE) project. The Japanese Society of Neuropsychopharmacology primarily disseminated information and updated treatment guidelines. The Organization of Persons with Psychosocial Disabilities (Porque) was engaged in community-building initiatives and combating stigma through public relations and support activities. For example, they published newspaper articles and appeared on television to raise awareness. Other organizations demonstrated limited activity with the least number of activities. Overall, the more active organizations prioritized policy, research, and communication, while activities related to community support and education were less frequent, indicating potential areas for development.
Discussion
This review identified various psychiatric burdens in Japan, including epidemiological, clinical management, societal welfare, humanistic, and economic perspectives. Although some stakeholder activities address these challenges, many gaps still remain.
Based on the characteristics of the included studies, despite the clinical and societal importance of schizophrenia, Japanese literature remains limited. Notably, publications declined over the past decade, suggesting reduced research attention. While clinical management and epidemiology were well represented, humanistic, societal, and economic burdens were underreported. Similarly, gray literature, including conference abstracts and other sources, was not plentiful. These trends highlight the need for renewed focus and sustained research efforts to capture the multifaceted burden of schizophrenia in Japan.
Schizophrenia’s prevalence in Japan (0.6%^5^) is comparable to global rates (0.3–0.6%^2,63–65^). Additionally, a systematic review by Saha et al. demonstrated that the mortality gap between schizophrenia patients and the general population is worsening globally, underscoring the need for targeted interventions^66^. Reported mortality data^11–15^ appears higher than the global average (~2.5%^67^), possibly due to study populations with comorbid conditions such as cancer and AMI, or emergency admissions. These patients have a higher mortality risk compared to general schizophrenia patients. Comorbidities, such as hypertension, diabetes, and depression, further complicate health and contribute to disease burden^16–18^. In Australia, national surveys by Morgan et al. emphasized the importance of integrating mental health services with physical healthcare to address comorbidities and improve patient outcomes^68^. To address these issues in Japan, more epidemiological research is needed to inform public health strategies, early interventions, and equitable healthcare policies.
In addition to physical health issues, suicide is a major contributor to mortality in schizophrenia. Several studies in this review addressed suicide and suicide attempts, underscoring the importance of suicide prevention in this population. While motives were not detailed in the reviewed literature, previous research has identified hallucinations and delusions as common triggers, along with social factors such as living alone and unemployment^69^. These findings highlight the need for both clinical and social support strategies to reduce excess mortality.
Clinical management of schizophrenia presents challenges due to the complex treatment regimens, long-term hospitalization, and medication side effects. Functional impairments, such as those related to ADLs and cognitive dysfunction, also added to the clinical management burden. However, stakeholder activities targeting these were limited in this review. Holistic care and expanded insurance coverage for cognitive assessments and counseling are needed to close these gaps. Clinical guidelines help standardize care, but implementation remains inconsistent. This is a global issue—despite their benefits, full adoption of guidelines is still challenging in the US and Europe^3,70,71^. The search of stakeholders’ activities revealed that, in Japan, the EGUIDE project has promoted guideline use by training psychiatrists. A multi-center study showed higher rates of key prescribing indicators, suggesting education improves practice^72^. Ongoing efforts like EGUIDE are essential to strengthen care quality.
The COVID-19 pandemic had measurable impacts on individuals with schizophrenia, as shown in gray literature. These included increased self-harm and suicidal ideation, shorter hospital stays, and an increase in discharge cases. Such findings highlight the vulnerability of this population during public health crises. To mitigate these effects, healthcare service and policy adaptations are essential. In Japan, early intervention of healthcare services for psychosis is still developing, with efforts focused on reducing the duration of untreated psychosis and building community-based networks for early detection and support^73^. Additionally, telemedicine has shown promise in improving treatment adherence and reducing relapse rates among patients with schizophrenia, especially during periods of restricted access to in-person care^74^. Strengthening these healthcare services could help maintain continuity of care and reduce the burden on patients, caregivers, and healthcare systems during future crises.
The stigma influences patients’ willingness to seek treatment and social integration, hindering access to public assistance and increasing emotional and social toll. Welfare support was insufficient, with stakeholders providing additional support. Although stigma is a global issue, New Zealand progressed through nationwide anti-stigma campaigns like “Like Minds, Like Mine,” which could guide Japan^75^. In Japan, patient organizations advocate through media or events. Kutcher et al. suggested stigma reduction requires context-specific, developmentally appropriate mental health literacy integrated into schools and communities^76^. Adopting similar strategies in Japan could help improve care access and welfare services.
Strengthening caregiver support systems and ensuring healthcare continuity during crises are essential. The review found that family members bear a disproportionate caregiving burden, risking mental health issues. Stakeholders’ activities were identified to address these challenges. According to Chien and Norman, mutual support groups for caregivers have been shown to reduce stress and improve coping mechanisms^77^. However, in the review, the burden during disasters/pandemics was identified but not addressed by stakeholder activities. The caregiver’s burden is especially relevant given the earlier discussion on COVID-19’s impact on patients, which likely also intensified the caregiving burden on families. Community-based disaster preparedness programs in the Philippines implemented programs that specifically address vulnerable populations^78^, could be adapted to Japan’s disaster-prone environment.
The economic burden of schizophrenia is substantial. Indirect costs, such as productivity loss from hospitalization or outpatient visits, and future income lost from premature death, exceed direct costs^59^. Despite this, our review did not identify any stakeholder activities addressing productivity losses or healthcare-related costs. Mitigating economic burden requires sustainable and comprehensive healthcare systems with public funding and insurance. Assessment of national and regional healthcare cost management is critical, as in the US case, where the economic burden of schizophrenia has been extensively documented, with estimates including both direct healthcare costs and indirect societal costs such as lost productivity^79,80^.
Limitations and strengths of research
This review leverages gray literature, often excluded from traditional literature reviews, thereby adding unique value by capturing a broader range of real-world evidence and activities. While hand searches for gray literature may introduce bias or overlook less publicized initiatives, this approach ensures a more comprehensive understanding of the current landscape. Although limited to 2013–2023, focusing on recent developments ensures that the findings are highly relevant to current healthcare policies. The research does not aim to evaluate the effectiveness of interventions by stakeholders’ activities for schizophrenia but instead highlights existing initiatives and identifies gaps between stakeholders’ activities and unmet needs, serving as a foundation for future intervention studies. Further research with broader methodologies like implementation science is necessary for a comprehensive understanding of patient circumstances and healthcare policies, but this review provides critical groundwork for future studies to address these gaps.
Conclusions
This review revealed the multifaceted and complex burden of schizophrenia from epidemiological, clinical, societal, welfare, humanistic, and economic perspectives. Policy recommendations include enhancing early diagnosis, standardizing treatment protocols, increasing public health funding, and improving welfare support systems to reduce the overall burden of schizophrenia. Effective strategies require collaborative approaches, including community-integrated care frameworks, multidisciplinary teams, and inclusive social welfare systems. However, the limited evidence underscores the need for evidence-based strategies, requiring further research, such as longitudinal studies and real-world data analyses, to monitor trends and evaluate healthcare interventions. These efforts will ensure that future strategies are grounded in robust evidence and tailored to the needs of patients and caregivers.
Supplementary information
Table S1, Table S2, and Document S1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Health Data Exchange (GH Dx). [cited 12 December 2024]. Available from: https://vizhub.healthdata.org/gbd-results/ (2021).
- 2World Health Organization. World Mental Health Report: Transforming Mental Health for All (World Health Organization, 2022).
- 3Keepers, G. A. et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Vol. 177, 868–872 (American Psychiatric Association Publishing, 2020).10.1176/appi.ajp.2020.17790132867516 · doi ↗ · pubmed ↗
- 4Galderisi, S. et al. Schizophrenia—Time to Commit to Policy Change (Oxford Health Policy Forum, 2024).
- 5Notice from the Director of the Regional Medical Planning Division, Medical Policy Bureau, Ministry of Health, Labour and Welfare. Medical system for diseases, businesses, and home healthcare. [cited 2025 Apr 4]. Available from: https://www.mhlw.go.jp/content/001103126.pdf (2023).
- 6Notice from the Director of the Medical Policy Bureau of the Ministry of Health, Labour and Welfare. 8th Medical Care Plan. [cited 2025 Apr 4]. Available from: https://www.mhlw.go.jp/content/001108169.pdf (2023).
- 7Occupational Health Division, Department of Safety and Health, Labour Standards Bureau, Ministry of Health, Labour and Welfare. The mental health policy for workplaces—guidelines for improvement of preservation of worker’s mental health. [cited 2025 Apr 4]. Available from: https://www.mhlw.go.jp/content/001579077.pdf (2025).
- 8Japanese Society of Psychiatry and Neurology. The Vision of Psychiatric Care and Health Welfare in Japan. [cited 2025 Apr 4]. Available from: https://www.jspn.or.jp/uploads/uploads/files/activity/20230520.pdf (2023).