Population frequencies of thiopurine-related pharmacogenes in healthy individuals from Kosovo
Flaka Pasha, Dunja Urbančič, Gordana Gosheva, Bukurije Zhubi, Safete Maliqi Qormemeti, Shaip Krasniqi, Irena Mlinarič-Raščan

TL;DR
This study identifies genetic variations in a Kosovo population that influence how people respond to thiopurine drugs, which could help improve personalized treatment strategies.
Contribution
The study reports population-specific frequencies of thiopurine-related pharmacogenes in healthy individuals from Kosovo, highlighting unique genetic profiles.
Findings
The MTHFR 677T variant (rs1801133) was significantly more frequent in the Kosovo population (49.8%) compared to global and European averages.
TPMT*3A and TPMT*3C variant frequencies were 2.0% and 0.1%, respectively, in the studied population.
NUDT15 rs116855232 was present at a frequency of 0.8%, and PACSIN2 rs2413739 had a minor allele frequency of 48.8%.
Abstract
Personalized thiopurine therapy is among the most established examples of pharmacogenomics translated into clinical practice. Variants in TPMT (rs1800462, rs1800460, rs1142345) and NUDT15 (rs116855232) are recognized clinical predictors of thiopurine efficacy and toxicity. Additional variants in genes such as PACSIN2 (rs2413739), ITPA (rs1127354) and MTHFR (rs1801133 and rs1801131), also contribute to variability in drug response. Here we characterize the frequency of the pharmacogenetic variants involved in thiopurine metabolism in a healthy population of Kosovo. We genotyped 299 healthy blood donors for polymorphisms. Among TPMT variant alleles, TPMT*3A was observed at a frequency of 2.0%, and the TPMT*3C at 0.1%. Notably, the MTHFR 677T variant (rs1801133) was significantly more frequent in the Kosovo population (49.8%) compared with the global and European frequencies. The minor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
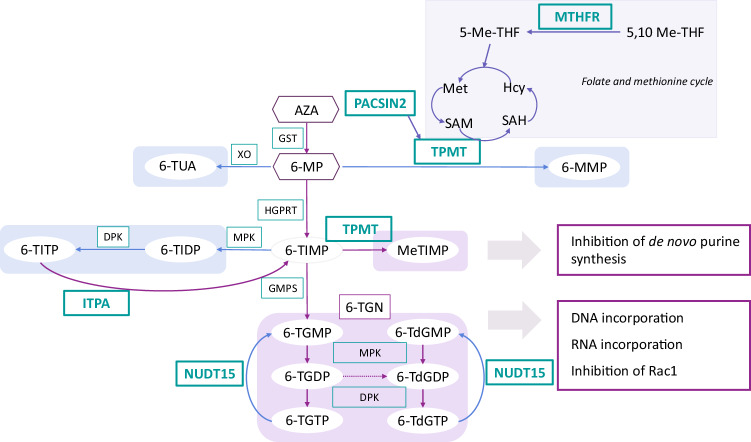 Figure 1
Figure 1- —https://doi.org/10.13039/501100004329The Slovenian Research and Innovation Agency (ARIS)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Lymphoblastic Leukemia research · Folate and B Vitamins Research · Retinoids in leukemia and cellular processes
Introduction
Genetic inheritance plays a crucial role in determining individuals’ response to therapy, influencing either favorable treatment outcomes or therapeutic failure accompanied by adverse effects^1^. Pharmacogenomics investigates how interindividual genetic variations impact patients’ response to therapy, aiming to enhance drug efficacy, while mitigating therapy-associated adverse effects^2^. In the field of pharmacogenomics and precision medicine, thiopurines have undergone comprehensive research and are now one of the best examples of its implementation into clinical practice^3^.
Thiopurines (6-mercaptopurine (6-MP), 6-thiogunanine (6-TG) and azathioprine (AZA)) are purine antimetabolites^4^ and immunosuppressant drugs^5^, frequently prescribed in the maintenance phase of acute lymphoblastic leukemia (ALL)^6^, for glucocorticoid-sparing remission maintenance of inflammatory bowel diseases^7^ and autoimmune disorders^8^, and in post-organ transplantation care^9^. Thiopurines are prodrugs that require metabolic activation to exert their clinical effects^10^. Mainly through incorporation into DNA and RNA^11^, active metabolites of thiopurines, 6-thioguanine nucleotides (6-TGNs), induce S-phase arrest and trigger programmed cell death^12^. The efficacy and safety of thiopurine treatment is influenced by thiopurine S-methyltransferase (TPMT), an enzyme that deactivates thiopurines by S-methylation toward the inactive metabolite 6-methylmercaptopurine (6-MMP), utilizing S-adenosyl methionine (SAM) as a methyl donor^13,14^. Four genetic variants in the gene encoding TPMT, namely *TPMT 2, *3A, *3B and 3C, have been recognized to contribute to reduced TPMT enzymatic activity in individuals^15^. Patients who are wild-type homozygotes (TPMT1/1) exhibit normal TPMT enzyme activity, while heterozygotes and variant homozygote individuals for TPMT2, *3A, *3B and *3C alleles show intermediate and low enzyme activity, respectively^16^. Decreased enzymatic activity of TPMT leads to higher concentration of 6-TGNs, greater cytotoxicity and higher risks of life-threatening adverse effects such as myelotoxicity^17^, secondary neoplasms^18^ and superimposed infections^19^.
Diverse thiopurine response among individuals cannot solely be attributed to TPMT polymorphisms (Fig. 1). Another important pharmacogene in thiopurine treatment already implemented into clinical practice is nudix hydrolase 15 (NUDT15)^20^. Because of its efficient hydrolysis of deoxyguanosine triphosphate (dGTP), NUDT15 is a crucial enzyme in purine nucleotide homeostasis. As active metabolites of thiopurines are analogs of dGTP, genetic polymorphisms in NUDT15 that decrease enzyme activity (NUDT153*, *2, *9 and *14) cause reduced 6-TGN levels and decreased thiopurine toxicity^21^. In addition, the genetic polymorphism rs2413739 (T > C) in PACSIN2 also influences TPMT activity. In pediatric patients, wild-type genotype was associated with lower TPMT activity and increased patients’ risk of gastrointestinal and hematologic toxicity^22^. Furthermore, inosine triphosphate pyrophosphatase (ITPA) catalyzes the pyrophosphohydrolysis of inosine triphosphate (ITP) to inosine monophosphate (IMP), preventing the accumulation of ITP and 6-thioxanthosine triphosphate into cells, rescuing them from apoptosis and reducing the risk of myelotoxicity and hepatotoxicity in patients treated with thiopurines. Studies have shown that the presence of at least one nonfunctional ITPA allele (either the 94C>A or IVS2+21A>C variant) is linked to a longer event-free survival compared with patients with the wild-type ITPA genotype. Moreover, patients with at least one nonfunctional ITPA allele had a reduced risk of experiencing early relapse or bone marrow relapse^23^. Lastly, single-nucleotide polymorphisms (SNPs) in MTHFR (rs1801133 and rs1801131) lead to reduced enzyme activity and have been recognized to increase 6-MP toxicity in patients with ALL. MTHFR catalyzes the formation of 5-methylenetetrahydrofolate, facilitating the conversion of homocysteine to methionine and thereby restoring the methylation potential of the cell. By reducing the availability of methionine and consequently SAM, genetic polymorphisms in MTHFR may decrease the methylation of thiopurines^14,24^.Fig. 1. Overview of key enzymes contributing to interindividual variability in the thiopurine response.5-Me-THF, 5-methyltetrahydrofolate; 5,10 Me-THF, 5,10-methylenetetrahydrofolate; 6-MeTIMP (6-methyl thioinosine monophosphate), 6-MMP, 6-methylmercaptopurine; 6-MP, 6-mercaptopurine; 6-TdGDP, 6-thio-deoxyguanosine diphosphate; 6-TdGMP, 6-thio-deoxyguanosine monophosphate; 6-TdGTP, 6-thio-deoxyguanosine triphosphate); 6-TG, 6-thioguanine; 6-TGDP, 6-thioguanosine diphosphate; 6-TGMP, 6-thioguanosine monophosphate; 6-TGN, 6-thioguanine nucleotide; 6-TGTP, 6-thioguanosine triphosphate; 6-TIDP, 6-thioinosine diphosphate; 6-TIMP, 6-thioinosine monophosphate; 6-TITP, 6-thioinosine triphosphate; 6-TUA, 6-thiouric acid; AZA, azathioprine; DNA, deoxyribonucleic acid; DPK, diphosphokinase; GMPS, guanosine monophosphate synthetase; GST, glutathione S-transferase; HGPRT, hypoxanthine-guanine phosphoribosyl transferase; Hcy, homocysteine; ITPA, inosine triphosphate pyrophosphatase; Met, methionine; MPK, monophosphokinase; MTHFR, methylenetetrahydrofolate reductase; NUDT15, nudix hydrolase 15; PACSIN2, protein kinase C and casein kinase substrate in neurons 2; RNA, ribonucleic acid; SAH, S-adenosylhomocysteine; SAM, S-adenosyl methionine; TPMT, thiopurine S-methyl transferase; XO, xanthine oxidase.
Genotyping for common and clinically relevant genetic polymorphisms related to thiopurine metabolism and folate cycle before application of thiopurines can thus mitigate adverse thiopurine effects, without compromising the disease relapse rate^25^. Guidelines from the Clinical Pharmacogenetics Implementation Consortium (CPIC), the Dutch Pharmacogenetics Working Group, and the Canadian Pharmacogenomics Network for Drug Safety recommend pre-emptive genotyping for variant alleles when there is a well-established functional impact; a global minor allele frequency (MAF) >1% or a MAF >1% in a specific population; availability of reference materials; feasibility of testing using standard laboratory methods; or a well-documented association between the variant allele and drug response^26^. According to CPIC and Dutch Pharmacogenetics Working Group guidelines, only genetic polymorphisms in TPMT and NUDT15 are currently recommended to be assessed before treatment^15^. Based on genotype, normal metabolizers for TPMT and NUDT15 should start with standard thiopurine doses, while intermediate metabolizers should receive 30–80% or 50–80% of standard AZA/6-MP or 6-TG dose, respectively. Poor metabolizers diagnosed with malignancies should initiate 6-MP at doses reduced tenfold and administered three times weekly, whereas in nonmalignant conditions, alternative treatments to AZA should be considered^27^.
Despite the well-documented association between genetic markers and thiopurine metabolism, their integration into clinical practice poses notable challenges^28^, including the absence of pre-emptive genotyping services in certain healthcare systems. Therefore, we aim to set the basis of genetic testing for individuals undergoing thiopurine therapy in Kosovo, by developing a framework for pharmacogenetic testing for TPMT, NUDT15, MTHFR, ITPA and PACSIN2 polymorphisms. As one of the requirements for implementing genetic polymorphism testing into clinical practice is a MAF greater than 1% in the general or a specific population, this study explores the frequency of genetic polymorphisms previously reported as (potential) biomarkers for thiopurine treatment in a healthy population from Kosovo. This study provides valuable insights into the genetic landscape within the Kosovo population and highlights both similarities and unique characteristics that contribute to enriching the map of human genetic variation worldwide.
Materials and methods
Study population
This study includes 299 healthy blood donors, randomly selected from the National Center for Blood Transfusion at the University Clinical Center of Kosovo. Inclusion criteria comprised age between 18 and 65 years, weight over 50 kg, hemoglobin levels within the reference range, normal blood pressure, no high-risk behaviors and no prior travel to areas endemic for malaria or Zika virus. The study was conducted in accordance with the Declaration of Helsinki, for studies involving humans. The study was approved by the Ethics Committee of the Faculty of Medicine, University of Prishtina ‘Hasan Prishtina’ (approval no. 4095, dated 31 May 2019) and by the University Clinical Center of Kosovo (approval no. 1429, dated 3 June 2019). Informed written consent, including the demographic questionnaire, was obtained from all participants involved in the study. From each study participant, 3–5 ml of whole venous blood was collected.
DNA isolation and genotyping
DNA was isolated from 200 µl of whole blood from each participant using the spin protocol for DNA purification, following the manufacturer’s instructions (QIAGEN QIAamp DNA Mini Kit).
Genetic polymorphisms in TPMT, PACSIN2, ITPA and MTHFR were determined by TaqMan SNP genotyping assay (Thermo Fisher Scientific, Applied Biosystems), following the manufacturers’ instructions. For quantitative PCR, we used the LightCycler 480 system (Roche). SNPs and part numbers of all TaqMan SNP genotyping assays are listed in Table 1.Table 1. The list of analyzed SNPs, their rs numbers, nucleotide changes and TaqMan Assay IDs.rs numberGene symbolNucleotide changeTaqMan assay IDrs1800462TPMTc.238G>C (2)C_12091552_30rs1800460TPMTc.460G>A (3B)C_30634116_20rs1142345TPMTc.719A>G (3C)C_19567_20rs2413739PACSIN2c.IVS2+21A>GC___2503304_20rs1127354ITPAc.94C>AC__27465000_10rs1801133MTHFRc.677C>TC___1202883_20rs1801131MTHFR*c.1298A>CC____850486_20rs number, reference SNP cluster ID.
Genetic polymorphisms in NUDT15 were determined by Sanger sequencing of exon 1 and exon 3, as the most relevant NUDT15 genetic variants lie within these regions. The procedure followed essentially the same protocol as previously reported^29^, with primers listed in Table 2. Samples were sequenced by Microsynth AG.Table 2. Primer pairs used for sequencing of exon 1 and exon 3 of NUDT15.PrimerSequence (5′–3′)NUDT15 exon1 forwardCAAAGCACAACTGTAAGCGACNUDT15 exon1 reverseCACACCTCACAGACGAACTCNUDT15 exon3 forwardCAAGCAAATGCAAAGCATCACNUDT15 exon3 reverseGGCTGAAAGAGTGGGGGATA
Statistical analysis
Sequences were determined using Finch TV software (Geospiza)^30^. Distributions of genotypes and possible deviations from the Hardy–Weinberg equilibrium were assessed by Fisher’s exact test. Differences between Kosovo, global and European allelic frequencies of SNPs were analyzed using Fisher’s exact test or chi-square test. The threshold for significance was set at P < 0.05.
Results
Population characteristics
To assess the distribution of genetic polymorphisms related to thiopurine treatment in the population of Kosovo, we collected blood samples from 299 consenting healthy blood donors. The mean age of the healthy blood donor cohort was 37 years. Among the 299 participants, 84% (n = 252) were male and 16% (n = 47) were female. The vast majority, 99% (n = 297), identified as Kosovars by nationality, while two participants identified as Turk (n = 1, 0.003%) and Egyptian (n = 1, 0.003%) minorities. Other ethnic groups were not represented in this study cohort. The donors were recruited from all regions of Kosovo, with 41% from Prishtina, 8% from Podujeva, 5% each from Gjilan, Peja, and Prizren, and the remaining participants from other cities, each contributing less than 5%.
Regarding blood types, group 0 was the most prevalent, accounting for 44% (n = 130) of the cohort, followed by type A at 39% (n = 118), type B at 12% (n = 37) and group AB at 5% (n = 14).
Frequencies of genetic variants in TPMT, ITPA, PACSIN2, MTHFR and NUDT15 in Kosovo population
To determine the frequency of the most relevant genetic polymorphisms in the genes implicated in thiopurine metabolism and folate cycle, we used TaqMan genotyping for variants in TPMT (rs1800462, rs1800460 and rs1142345), ITPA (rs1127354), PACSIN2 (rs2413739) and MTHFR (rs1801133 and rs1801131) and Sanger sequencing for NUDT15. All 299 individuals in our study were genotyped for SNPs in TPMT, MTHFR, PACSIN2 and ITPA. A subpopulation of donors (N = 184) was tested for NUDT15. In Table 3, we present the frequencies of alleles and genotypes for each gene in detail.Table 3. Allele and genotype frequencies of polymorphisms influencing thiopurine metabolism and folate cycle among 299 healthy blood donors from Kosovo.GeneAllele and SNP IDNucleotide changeMajor > minor alleleN^a^Major allele homozygote (N)Heterozygote (N)Minor allele homozygote (N)MAFHWE (P value)TPMT**TPMT2,* rs1800462NC_000006.11:g.18143955C>GC > G277277000>0.9999TPMT3A*, rs1800460, rs1142345NC_000006.11:g.18139228C>T NC_000006.11:g.18130918T>CC > T T > C2992871200.02>0.9999TPMT3C*, rs1142345NC_000006.11:g.18130918T>CT > C2992861300.001>0.9999MTHFRrs1801133NC_000001.10:g.11856378G>AG > A29980140790.4980.748rs1801131NC_000001.10:g.11854476T>GT > G299156122210.2740.9663PACSIN2rs2413739NC_000022.10:g.43397036C>TC > T29784136770.4880.6116ITPArs1127354NC_000020.10:g.3193842C>AC > A2992752400.04>0.9999NUDT15rs45465203NC_000013.10:g.48612214G˃AG ˃ A1841374520.1330.8781rs61973267NC_000013.10:g.48619942G˃AG ˃ A1841562620.0820.912rs79687000NC_000013.10:g.48612157C˃TC ˃ T184179500.021>0.9999rs377238223NC_000013.10:g.48612050C˃GC ˃ G184183100.003>0.9999rs746071566NC_000013.10:g.48611920GAGTCG[2]delGAGTCG184183100.003>0.9999NUDT153*, rs116855232NC_000013.11:g.48045718C>TC > T184182110.0080.6229The threshold for significance was set to p < 0.05.^a^The number of the individuals successfully assessed.HWE Hardy–Weinberg equilibrium, MAF minor allele frequency.
No significant deviation from Hardy–Weinberg equilibrium was observed for any of the investigated genetic polymorphisms (P = 0.6116-0.999; Fisher’s exact test). In the Kosovo population, we observed the following MAFs for alleles in the TPMT, PACSIN2, ITPA and MTHFR genes. The TPMT2* allele was not detected (MAF of 0%). The TPMT3A* allele, a diplotype of TPMT3B* and TPMT3C*, was found in 12 heterozygous individuals with a frequency of 2.0%. The TPMT3C* allele alone was identified in one heterozygous individual, at a frequency of 0.1%. For the PACSIN2 rs2413739 variant, the MAF was 48.8%, while for the ITPA rs1127354 variant the MAF was 4%. For the MTHFR gene, the rs1801133 variant had a MAF of 49.8%, and the rs1801131 variant was observed at a frequency of 27.4%.
We identified six variants in NUDT15 by Sanger sequencing of exon 1 and exon 3. The identified variants were NUDT15 rs45465203 with a MAF of 13.3%, followed by rs61973267 (8.2%), rs79687000 (2.1%), rs116855232 (0.8%), rs377238223 (0.4%) and rs746071566 (0.4%).
Comparison of Kosovo population with general global and European populations
To assess similarities and differences in the MAFs of polymorphisms associated with thiopurine metabolism, we compared data from the Kosovo population with global and European reference populations using the gnomAD database and applied the Fisher’s exact test or chi-square test, as appropriate^31^. We present our findings in Table 4.Table 4. Comparison of minor allele frequencies (MAFs) (%) for common polymorphisms related to thiopurine metabolism, between global, European and Kosovo population.PharmacogeneTPMT^b^NUDT15ITPAPACSIN2**MTHFRLevel of evidence (CPIC/PharmGKB)^a^A/1AA/1AA/1ANANANAA/1ANAA/1ANA/3NA/3NA/4NAMAF (%)rs1800462rs1800460rs1142345rs45465203rs61973267rs79687000rs746071566rs377238223rs116855232rs1127354rs2413739rs1801133rs1801131Kosovo population0.02.02.113.38.22.70.270.270.804.048.849.827.4Global population0.213.54.311.96.42.80.590.00471.27.542.631.830.3P value for Kosovo versus global population0.63730.05950.01450.42100.23310.99280.73010.01750.80590.00160.0027<0.00010.1343European population0.254.24.613.16.82.20.280.00550.257.344.033.731.3P value for Kosovo versus European population0.6520.0113****0.00510.87730.17090.4817>0.99990.02050.06920.00220.0088<0.0001****0.0446The threshold for significance (in bold) was set to P < 0.05.^a^Level of evidence for thiopurines were retrieved from CPIC guidelines and ClinPGx database^32^. CPIC levels (gene–drug evidence): A, strong actionable; B, moderate; C/D, limited. ClinPGx (that is, PharmGKB) levels (variant–drug evidence)^33^: 1A, guideline-supported/actionable; 1B–2B, moderate; 3–4, preliminary. NA, no level of evidence or clinical guideline available.^b^TPMT2* corresponds to rs1800462; TPMT3A* to the haplotype of rs1800460 and rs1142345; and TPMT3C* to rs1142345.
We observed significant differences between Kosovo and global/European populations, especially in frequencies of MTHFR polymorphisms; however, the MAFs of certain other polymorphisms in the Kosovo population, particularly those of ITPA, PACSIN2 and TPMT, also showed significant deviations from global and/or European populations.
The global and European MAF for the TPMT rs1800462 variant is 0.2%, with no statistically significant differences compared with the Kosovo population, in which no carriers of this variant were detected. Similarly, there were no significant differences in the MAF of the TPMT rs1800460 variant between Kosovo (MAF of 2%) and global (3.5%), while there was a significant difference (P = 0.0113) with the European population (4.2%). By contrast, for the TPMT rs1142345 variant, the global population MAF is 4.3% and the European population MAF is 4.6%, whereas the Kosovo population MAF was slightly lower at 2.1%, representing a statistically significant difference (P = 0.0145 and 0.0051, respectively).
Furthermore, the MAFs for the NUDT15 rs45465203, rs61973267, rs79687000, rs116855232 and rs746071566 variants in the Kosovo population were not statistically different from those in the European population. The NUDT15 variant rs377238223 showed a statistically significant deviation in allele frequency in the Kosovo population; however, this finding was based on a single individual and may represent a chance occurrence.
We also examined the MAF for the ITPA rs1127354 variant in the Kosovo population, which was 4%. This was significantly lower than the MAF of this variant in the global (7.5%) and the European (7.3%) population, with P values of <0.0016 and <0.0022, respectively. In addition, the MAF for the PACSIN2 rs2413739 variant in the Kosovo population was significantly higher compared with the global population (P < 0.0027) and European population (P < 0.0088).
When comparing MAFs of MTHFR rs1801131, no statistically significant differences were observed between the Kosovo population (27.4%) and the global population (30.3%). However, a slight but statistically significant difference was found when compared with the European population (P = 0.0446). By contrast, the MAF of the MTHFR rs1801133 variant (677C>T) in the Kosovo population was 49.8%, which is significantly higher (P < 0.0001) than the MAF in both the global population (31.8%) and the European population (33.7%). Notably, this frequency is comparable to that reported for the Italian population (46.7%), with no statistically significant difference observed.
Discussion
This study presents a comprehensive analysis of genetic polymorphisms associated with thiopurine metabolism and the folate pathway in a healthy population of Kosovo, evaluating the allele frequencies of pharmacogenes relevant to thiopurine therapy in this population. The findings provide essential information to guide healthcare practitioners and policymakers in establishing and optimizing pre-emptive genotyping services in Kosovo.
We genotyped 299 healthy blood donors from the National Center for Blood Transfusion of Kosovo and assessed the cohort for 7 genetic polymorphisms in 4 different genes, that is, TPMT, ITPA, PACSIN2 and MTHFR, and additionally identified six genetic variants in NUDT15. These specific variants were selected on the basis of established evidence of their association with thiopurine efficacy and toxicity^26^. Among the investigated variants, TPMT and NUDT15 polymorphisms are supported by high-level evidence for clinical implementation in thiopurine pharmacogenomics (Table 4). By contrast, the evidence for PACSIN2, ITPA and MTHFR variants is limited to individual clinical reports suggesting possible effects on thiopurine dosing or toxicity, while the additional NUDT15 variants were identified by sequencing in this study and have no previous association with thiopurine treatment.
The most clinically relevant TPMT variants, TPMT3C* and TPMT3A*, were found at low frequencies in the Kosovo population. Although the TPMT3A* allele is the most common TPMT-activity-affecting variant in the European population, the Kosovo population had a MAF of 2.0%, which is lower than that reported in other European cohorts (2.7–4.5%)^32,33^. The TPMT3C* allele, which is more prevalent in East Asian and African populations, was rare (0.1%), aligning with findings from other Eastern European countries such as Poland (0.1%), Sweden (0.2%) and Bulgaria (0.2%)^34–36^.
In contrast to the TPMT3A* allele, NUDT15 polymorphisms showed frequencies consistent with reports from non-Finnish European populations and global population. Two individuals carried the clinically important NUDT153* variant (rs116855232), and one carried rs746071566, a microsatellite insertion previously reported not to be associated with thiopurine-induced myelosuppression^37^. The Kosovo MAF for rs61973267 was similar to that of other European populations, including Finnish (6.1%), British (8.8%) and Spanish (5.1%) cohorts^38^.
The MAF of the ITPA rs1127354 variant, associated with thiopurine-related adverse effects^39^, was significantly lower in Kosovo population than in global and broader European datasets. However, the MAF remained above 1%, supporting the consideration of this variant in pharmacogenomic screening. Although current evidence is insufficient to support the routine inclusion of PACSIN2 rs2413739 in pre-emptive testing guidelines, the slightly higher MAF observed in the Kosovo population highlights its potential relevance and supports further investigation into its clinical utility in thiopurine pharmacogenomics^40^.
A particularly interesting result was the high frequency of MTHFR rs1801133 (c.677C>T; p.Ala222Val) variant, with a MAF of 49.8%, which is significantly higher than the MAF in global (31.8%) and European populations (33.7%), including Finnish (27.3%)^41^ and British (32.4%) subpopulations^42^. Higher MTHFR C677T allele frequencies have been previously reported in Hispanic/Latin American populations (CLM, MXL, PEL and PUR), in certain regions of China (CHB) and in specific parts of Italy (TSI)^43,44^. The comparison analysis across populations with relatively high MAFs (>45%) for MTHFR rs1801133 showed that the Kosovo population exhibits a similar frequency of the MTHFR 677T allele (Supplementary Table 1). When extended to all polymorphisms investigated, correlation analysis indicated that the Kosovo population is most similar to other European populations, particularly those from Southern Europe (for example, Toscani Italians), while also sharing allelic trends with Latin American groups and the Finnish population (Supplementary Table 1). The MTHFR 677 variant leads to a thermolabile MTHFR enzyme with considerably reduced MTHFR activity—about 60% in heterozygous and as low as 10% in variant homozygous individuals^45–47^. Reduced MTHFR activity disrupts the efficiency of one-carbon metabolism, which is crucial for cell differentiation and growth^48^. This genetic polymorphism is thus strongly associated with elevated homocysteine levels, as well as increased susceptibility to congenital birth defects, such as neural tube defects^49^ and congenital heart defects^50^. Given the high MAF of the MTHFR rs1801133 variant observed in the Kosovo population, not only could there be an increased risk of impaired thiopurine methylation, but public health strategies should also consider targeted folate supplementation programs—particularly for women of reproductive age—to mitigate the risk of folate-related birth defects^51^.
Some limitations of our study should be acknowledged. The results are obtained from a specific healthy blood donor sample cohort and may not fully represent all subpopulations in Kosovo, especially those with diverse ethnic backgrounds. Given that the frequency of SNPs can differ across ethnic groups, future studies should include multiple ethnic groups to validate the broader applicability of our results. In addition, our cohort consisted predominantly of males (84%), which may not fully capture gender differences in the population, despite the absence of X-linked SNPs. Therefore, future studies with more ethnically diverse populations, incorporating a wider array of genetic and nongenetic factors, would not only improve the robustness of allele frequency estimates but also enhance the clinical utility of pharmacogenomic recommendations.
Conclusion
This study represents an important first step in characterizing the pharmacogenetic variation related to thiopurine metabolism in a healthy population of Kosovo. By providing allele frequency data for key variants in TPMT, NUDT15, ITPA, PACSIN2 and MTHFR, these findings offer essential insights into the genetic landscape of Kosovo population. They reveal important implications for the development of personalized thiopurine treatment strategies. Although advancements in pharmacogenomics and precision medicine are evident globally, successful integration of pre-emptive approaches into the healthcare system in Kosovo will require overcoming barriers such as limited awareness, a lack of trained personnel, costs and accessibility of services, and the need for infrastructure to support continuous patient monitoring. The study lays the groundwork for future efforts for the implementation of pharmacogenomic data into clinical decision-making in Kosovo, aiming to enhance patient safety and treatment efficacy.
Supplementary information
Supplementary Table 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Urbančič D., Pasha F., Šmid A. & Mlinarič-Raščan I. Personalization of thiopurine therapy: Current recommendations and future perspectives. Acta Pharm.74, 335-381 (2024).10.2478/acph-2024-003039279525 · doi ↗ · pubmed ↗
- 2Finch TV. Digital World Biologyhttps://digitalworldbiology.com/Finch TV (accessed 14 September 2024).
- 3Gareth, J. et al. Association of Genetic variants in nudt 15 with thiopurine-induced myelosuppression in patients with inflammatory bowel disease. JAMA 321, 773–785 (2019).10.1001/jama.2019.0709 PMC 643987230806694 · doi ↗ · pubmed ↗
- 4rs 61973267 (SNP) - Population genetics - Homo_sapiens - Ensembl genome browser 112. Ensemblhttps://www.ensembl.org/Homo_sapiens/Variation/Population?db=core;r=13:48045306-48046306;v=rs 61973267;vdb=variation;vf=813468842 (accessed 14 September 2024).
- 5rs 1801133 (SNP) - Population genetics - Homo_sapiens - Ensembl genome browser 112. Ensemblhttps://www.ensembl.org/Homo_sapiens/Variation/Population?db=core;r=1:11795821-11796821;v=rs 1801133;vdb=variation;vf=122492 (accessed 14 September 2024).