Effects of continuous and interval training on inflammatory and vascular adhesion markers in sedentary individuals with type 1 diabetes
Alberto Hermo-Argibay, Laura Brugnara, Serafín Murillo, Joan-Marc Servitja, Víctor M. Víctor, Anna Novials, Susana Rovira-Llopis

TL;DR
This study compares how continuous and interval training affect inflammation and adhesion markers in people with type 1 diabetes and healthy individuals.
Contribution
The study reveals how different exercise types influence inflammatory and adhesion molecules in type 1 diabetes and healthy populations.
Findings
HIIT increased IL-10 levels in individuals with T1D.
Continuous training reduced VCAM1 in healthy controls.
Baseline fitness levels correlate with adhesion molecule responses to training.
Abstract
This study evaluates and compares the effects of continuous and interval training on inflammatory and adhesion molecules in subjects with Type 1 diabetes mellitus (T1D) and healthy controls. Using Luminex X-MAP, serum inflammatory and adhesion molecules were measured in 50 non-obese, sedentary adults (78% women; mean age 34 years), including 27 with T1D and 23 healthy controls. Subjects with T1D exhibited a tendency towards decreased interleukin 10 (IL-10) levels and increased intercellular adhesion molecule (ICAM1) levels compared to controls. Exercise training, specifically high-intensity interval training (HIIT), increased IL-10 levels in the T1D group. Among controls, we observed a decrease in vascular cell adhesion molecule 1 (VCAM1) after continuous training, and in platelet selectin (P-selectin) after HIIT. The correlation studies revealed that subjects with higher baseline…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
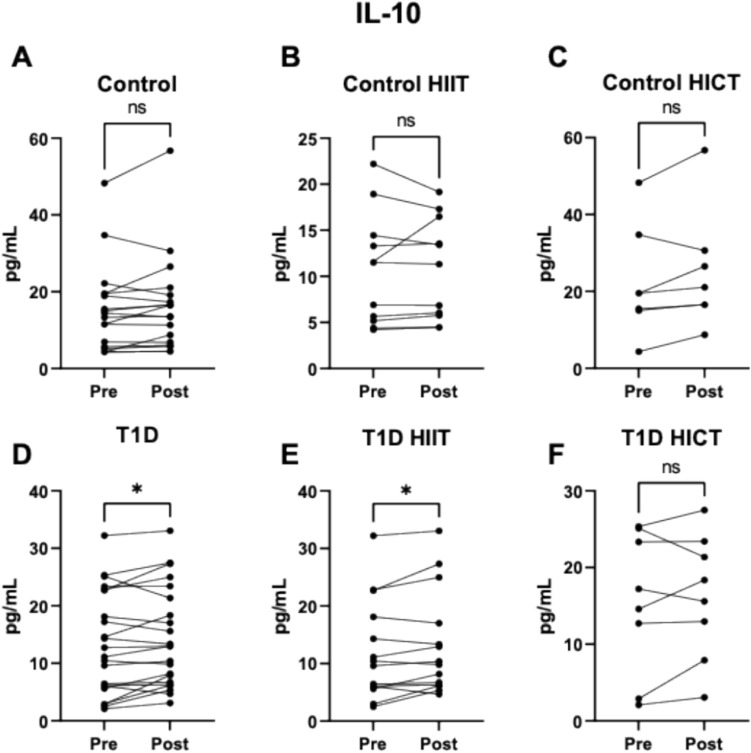 Figure 1
Figure 1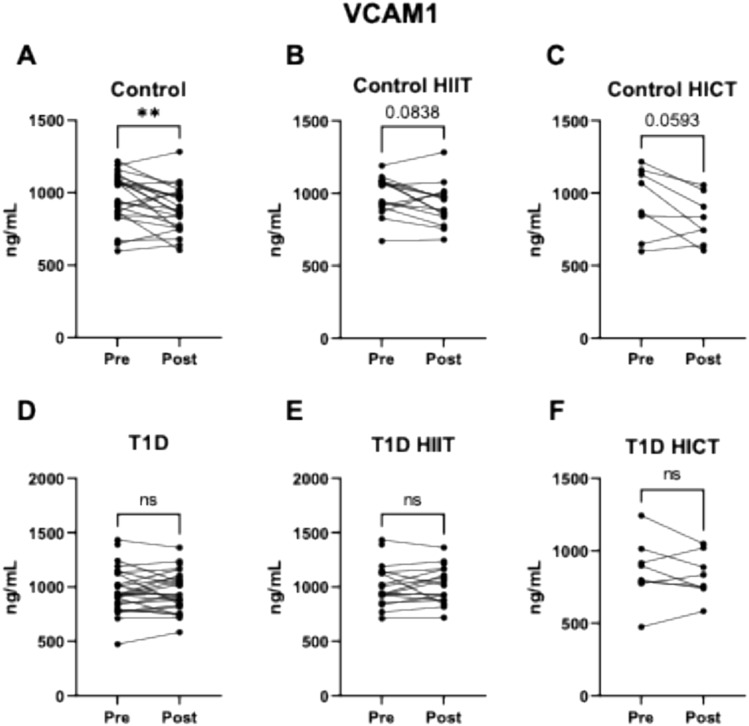 Figure 2
Figure 2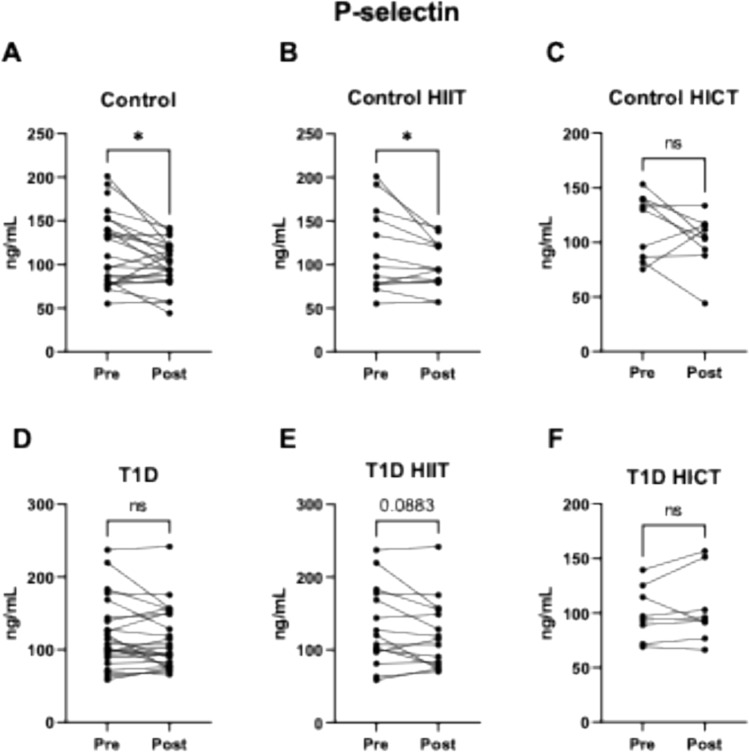 Figure 3
Figure 3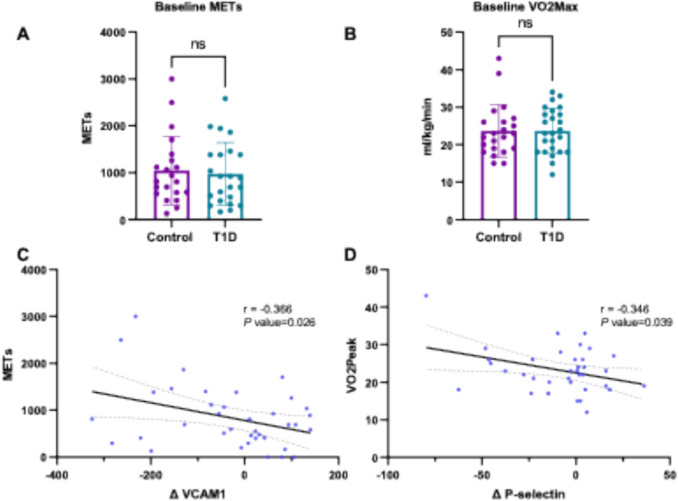 Figure 4
Figure 4- —http://dx.doi.org/10.13039/501100014849Conselleria de Cultura, Educación y Ciencia, Generalitat Valenciana
- —http://dx.doi.org/10.13039/501100015755Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas
- —http://dx.doi.org/10.13039/501100004587Instituto de Salud Carlos III
- —http://dx.doi.org/10.13039/501100013941Centro de Investigación Biomédica en Red Diabetes y Enfermedades Metabólicas Asociadas
- —Universitat de Valencia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsExercise and Physiological Responses · Cardiovascular and exercise physiology · Thermoregulation and physiological responses
Introduction
In type 1 diabetes mellitus (T1D), β-cells within the pancreatic islets of Langerhans are destroyed, resulting in the loss of insulin secretion (Delmastro and Piganelli 2011). This process is mediated by activation of the c-Jun N-terminal kinase (JNK) pathway by pro-inflammatory cytokines, which contributes to β-cell destruction (Kaneto et al. 2005). Additionally, β-cells secrete cytokines such as interleukin-1 beta (IL-1β), which, under normal conditions, promotes their proliferation (Maedler et al. 2002). However, in T1D, in conjunction with tumor necrosis factor-alpha (TNFα), IL-1β can induce apoptosis (Cnop et al. 2005). In addition, it has been demonstrated that TNFα and interleukin-6 (IL-6), both pro-inflammatory cytokines, play crucial roles in T1D progression and the regulation of insulin secretion (Atri et al. 2018).
Chronic low-grade inflammation and sustained hyperglycemia promote endothelial dysfunction, thereby disrupting vascular tone regulation and homeostasis (D.-R. Yang et al. 2024). This dysfunction leads to an imbalance that favors vasoconstriction and poor regulation of vascular smooth muscle (Bertoluci et al. 2008), contributing to the vascular complications that are a leading cause of morbidity and mortality in patients with T1D (James et al. 2014). Endothelial dysfunction also promotes atherogenesis and the development of subclinical atherosclerosis by activating signaling pathways in endothelial cells that increase the production of cellular adhesion molecules (CAMs), cytokines, and chemokines, resulting in the interaction of leukocytes with the vascular wall, to which they subsequently adhere. This process is mediated by selectins. In inflammatory processes, leukocyte recruitment begins when the movement of leukocytes through the blood flow slows and they begin to roll along the endothelial walls, eventually adhering to them and migrating through the endothelium towards the focus of infection (Leick et al. 2014). In this sense, a recent study by Canet et al. (2022) demonstrated that patients with T1D exhibit increased leukocyte–endothelial interactions, with a reduced rolling velocity over the vascular wall and a higher number of adhered leukocytes compared to a control group.
Maintaining high levels of physical activity is reported to benefit the quality of life of patients with T1D. Notably, it improves glucose metabolism regulation by increasing time in range and reducing fasting glucose levels (Riddell et al. 2023), as well as enhancing insulin sensitivity, lowering glycated hemoglobin, and improving lipid profiles (Salem et al. 2010). Additionally, it enhances metabolic flexibility and cardiorespiratory fitness (D ‘ hooge et al. 2011; Heyman et al. 2007; L. Roberts et al. 2002). These benefits indicate a lower risk of developing the cardiovascular diseases associated with diabetes (Wu et al. 2019). It is noteworthy that in T1D, muscle carnosine levels are increased and associated with a more atherogenic lipoprotein profile, which is especially relevant in subjects with T1D and low cardiovascular fitness (Brugnara et al. 2022). These findings highlight the beneficial effects of physical exercise and physical fitness status on vascular health and cardiometabolic risk factors.
Exercise also exerts an anti-inflammatory effect, such as that produced in muscle contractions in which IL-6 is released, which stimulates the production of anti-inflammatory cytokines, thus inhibiting TNFα activity and reducing inflammation (Petersen & Pedersen 2005). Notably, interleukin-10 (IL-10), the natural receptor antagonist IL-1Ra, interleukin-1 alpha (IL-1α), IL-1β, and interleukin-8 (IL-8) are involved in this anti-inflammatory response, with a potential inhibition of T-cell activation and nuclear factor kappa B (NF-κB) (Sharifinejad et al. 2022). Beneficial effects are also observed on adhesion molecules such as CAMs, resulting in reductions in intercellular adhesion molecule 1 (ICAM1), vascular cell adhesion molecule 1 (VCAM1), and platelet-selectin (P-selectin) levels (J. Yang et al. 2017).
In clinical research involving continuous aerobic exercise, the majority of interventions have traditionally been categorized as moderate-intensity continuous training (MICT) (Gao et al. 2025). However, according to contemporary intensity domain classifications, many of these protocols actually fall within the heavy-intensity domain, often slightly above the first lactate threshold (Iannetta et al. 2020). Therefore, it may be more appropriate to refer to them as heavy-domain intensity continuous training (HICT). This reclassification highlights the need for greater precision when describing exercise intensity domains in the scientific literature. In parallel, within high-intensity interval training (HIIT) interventions, a wide variety of modalities has been investigated. The most common approaches involve intervals lasting 30 s to 2 min, performed at intensities ranging from 85 to 110% of the peak power output (PPO) attained during a maximal oxygen uptake (VO₂max) test, or at 85–95% of maximal heart rate (Gao et al. 2025; Tschakert and Hofmann 2013).
HIIT has been gaining increasing attention in exercise intervention studies, positioning itself as an effective strategy for improving aerobic capacity (Opazo-Díaz et al. 2024). Despite numerous studies in the literature, it remains unclear whether interval and/or continuous training exert beneficial effects on circulating cardiovascular disease markers in healthy subjects and individuals with T1D, such as pro- and anti-inflammatory cytokines and CAMs, particularly because individuals engaging in the same level of physical activity show differences in physical capacities (Murillo et al. 2024). In the present study, we have explored differential training-induced effects on inflammatory cytokines and CAMs depending on the type of training (interval/continuous) and the target population (healthy/T1D).
Methods
Study design
Almost all participants in this study were selected from a cohort of a previous study by Murillo et al. (2022). Training sessions took place in the laboratory of Exercise and Diabetes at IDIBAPS-Hospital Clínic Barcelona, where blood samples were also collected. These samples were subsequently processed at the Translational Research Unit of Endocrinology and Metabolism of the University Hospital Doctor Peset.
Participants
The present study included 50 sedentary participants, 27 of whom had T1D. Inclusion criteria for the T1D group required a diagnosis of at least 6 months, an age between 18 and 50 years, hemoglobin A1c below 9.5%, and no regular physical exercise in the preceding 3 months. Participants with T1D had a mean time since diagnosis of 18.8 ± 9.7 years. The exclusion criteria included advanced diabetic complications (with the exception of non-proliferative retinopathy), musculoskeletal injuries, pregnancy, or any condition limiting the ability to perform physical exercise. The remaining 23 participants were healthy individuals, with an effort made to ensure a similar age and sex distribution to that of the T1D group.
Measurements
VO₂max and PPO were determined using a ramp incremental test on a cycle ergometer. The test began with a 5-min warm-up at low intensity (40 watts), followed by continuous increments of 15 watts every minute until volitional exhaustion. Participants were instructed to maintain a cadence between 60 and 80 revolutions per minute. Maximum strength was assessed via a one-repetition maximum leg press test. Body composition was evaluated using an iDXA Lunas (GE Healthcare). Blood samples were collected for analysis. All initial measurements were repeated 48 to 72 h after the last training session. Blood samples were sent to the Endocrinology and Nutrition Translational Research Unit at University Hospital Doctor Peset (Valencia, Spain) for analysis. The physical activity level and the Metabolic Equivalents of Task (METs) of the subjects have been determined using the International Physical Activity Questionnaire (IPAQ).
Training protocol
The exercise program consisted of three sessions per week on alternate days over 3 weeks (a total of nine sessions), with each group following a specific exercise regimen performed on a cycle ergometer (Wattbike PRO, Nottingham, UK). The HICT group engaged in continuous training within the heavy-domain intensity for 30 min at 65–70% of VO₂max. The HIIT group performed high-intensity interval training, consisting of 10 repetitions of 30 s at 100–120% of PPO, interspersed with 2-min intervals of active recovery at 40–50% VO₂max. Both regimens included a 5-min warm-up and a 5-min cool-down.
Immunoassays
Serum levels of inflammatory mediators, IL-6, IL-1β, and TNFα, anti-inflammatory mediators such as IL-10, as well as those of myeloperoxidase (MPO) and the adhesion molecules VCAM1, ICAM1, and P-Selectin, were quantified using Luminex® with xMAP technology (Luminex®200, Luminex Corporation™, Austin, TX, USA). Milliplex® kits (Merck KGaA, Darmstadt, Germany), specifically the “Human Cardiovascular Disease Magnetic Bead Panel 2” and “Human High Sensitivity T Cell Magnetic Bead Panel,” were used for quantification. The analyses were performed in duplicate, with intra- and inter-assay coefficients of variation of < 5.0% and < 15%, respectively.
Statistical analysis and data representation
Data analysis was conducted using SPSS® 20.0 (IBM SPSS™ Statistics, Chicago, USA). The Shapiro–Wilk test was employed to check the normality of population distribution. Parametric data are presented as mean ± standard deviation. Qualitative data are expressed as percentages. A student’s t-test was used for comparing parametric data between independent groups (control vs. T1D) and paired t-tests were employed for dependent groups (pre- vs. post-intervention). Bivariate Pearson correlation was used for correlation analysis. A 95% confidence interval was applied for all tests, and differences were considered significant at p < 0.05. A tendency was assumed for p values between 0.1 and 0.05. Data were analyzed and represented using GraphPad Prism® v.9.0.2 (GraphPad Software™, Boston, MA, USA).
Results
Cohort characteristics
In the present study, we assessed a total of 50 sedentary subjects comprised of patients with T1D (27) and healthy controls (23). There were no significant differences between the groups regarding anthropometric parameters and body composition at the start of the exercise intervention (Table 1). The following fitness-related parameters were also similar between controls and subjects with T1D: VO_2_max, METs, external load relative to VO_2_max and maximum weight lifted in the leg press. Table 1. Anthropometric and fitness-related parameters and serum levels of cytokines and adhesion molecules in the study population at baselineControlT1Dp-valueSample size**2327–**Sex (% women)86.9%70.4%–Age (years)31.5 ± 6.935.9 ± 9.30.071Body mass (kg)63.9 ± 12.170.3 ± 14.30.112BMI (kg/m^2^)23.0 ± 3.525.2 ± 4.30.07Fat (%)31.7 ± 7.132.7 ± 7.40.667Lean mass (kg)41.7 ± 7.6444.9 ± 8.90.203Visceral adipose tissue (g)290.3 ± 316.6444.8 ± 441.90.203METs1048 ± 726794 ± 7020.820VO_2_max (ml·kg·min)23.7 ± 7.023.7 ± 6.00.999Peak power output relative to body mass (W/kg BM)2.1 ± 0.62.0 ± 0.60.391Maximum weight lifted in leg press relative to body mas (kg/kg BM)2.29 ± 0.532.13 ± 0.770.473ICAM1 (ng/mL)69.59 ± 14.7279.71 ± 21.570.059MPO (ng/mL)204.4 ± 141.8210.5 ± 148.10.771P-selectin (ng/mL)117.94 ± 42.25117.13 ± 51.260.922VCAM1 (ng/mL)966.3 ± 176.0967.3 ± 214.50.933IL-10 (pg/mL)20.00 ± 14.7313.38 ± 8.890.078IL-1β(pg/mL)2.99 ± 1.632.84 ± 1.370.659IL-6 (pg/mL)2.70 ± 1.542.68 ± 1.440.703TNFα (pg/mL)12.54 ± 5.3012.50 ± 2.510.905The results are expressed as mean ± standard deviation or as a percentage.BMI body mass index, BM body mass, ICAM1 intercellular adhesion molecule 1, IL interleukin, METs metabolic equivalents, MPO myeloperoxidase, TNFα tumor necrosis factor alpha, VCAM1 vascular cell adhesion molecule 1, VO_2_max maximal oxygen uptake
After the 3-week exercise intervention, significant changes were observed in the subjects’ anthropometric and fitness characteristics (Table 2). In short, HIIT increased relative strength in both groups, improved VO_2_max and PPO relative to body mass (W/kg) in healthy subjects and decreased total fat and increased lean mass in T1D, whereas HICT increased PPO relative to body mass (W/kg) in both groups and increased relative strength among subjects with T1D. Table 2. Effect of the exercise intervention according to the group and protocol usedControlT1DHIITHICTHIITHICTPrePostP valuePrePostP valuePrePostP valuePrePostP valueBody mass (kg)66.8 ± 13.063.0 ± 18.1ns64.0 ± 12.763.9 ± 12.8ns72.0 ± 16.272.2 ± 16.2ns68.1 ± 12.568.8 ± 12.2nsBMI (kg/m)23.2 ± 3.919.83 ± 9.13ns23.4 ± 3.423.3 ± 3.4ns25.3 ± 4.825.4 ± 4.9ns25.4 ± 4.425.6 ± 4.1nsFat (%)30.9 ± 8.729.5 ± 8.9ns32.7 ± 5.032.3 ± 4.9ns32.4 ± 8.131.7 ± 8.00.00634.0 ± 6.934.0 ± 7.0nsLean mass (kg)42.2 ± 6.442.8 ± 6.5ns43.0 ± 9.7043.26 ± 9.68ns45.5 ± 9.846.1 ± 9.80.0142.9 ± 6.643.4 ± 6.6nsVisceral fat (g)306.0 ± 386.9317.5 ± 373.8ns268.1 ± 238.5289.6 ± 249.8ns533.7 ± 510.0526.8 ± 515.7ns383.1 ± 341.7377.0 ± 351.1nsVo_2_max (ml/kg/min)24.2 ± 8.427.9 ± 6.70.00223.9 ± 4.124.6 ± 4.7ns23.62 ± 5.6224.7 ± 5.0ns23.8 ± 6.924.3 ± 4.8nsPeak power output relative to body mass (W/kg)2.28 ± 0.722.49 ± 0.710.0171.75 ± 0.292.15 ± 0.330.0012.19 ± 0.582.29 ± 0.48ns1.49 ± 0.341.67 ± 0.370.004Relative strength (kg/kg body weight)1.93 ± 0.302.24 ± 0.450.0192.49 ± 0.952.79 ± 1.20ns2.09 ± 0.312.28 ± 0.340.0232.16 ± 0.752.32 ± 0.830.013The result is expressed as mean ± standard deviation. ns P value > 0.05 when compared using a paired samples t-test Data is presented as mean ± standard deviationBMI body mass index, VO_2_max maximal oxygen uptake*. P* values indicates significant differences versus baseline
Inflammation and adhesion molecules
To analyze the inflammatory status of the subjects and the impact of exercise on this condition, we quantified the presence of key molecules involved in the inflammatory response: IL-10, an anti-inflammatory marker, and the pro-inflammatory cytokines IL-1β, IL-6, and TNFα. A comparison at pre-intervention between patients with T1D and controls showed a trend toward lower levels of IL-10 in patients with T1D (mean difference of 6.62 ± 3.67, p = 0.078) (Table 1). No significant differences were observed in the levels of IL-1β, IL-6, and TNFα between T1D and controls.
Upon analyzing the impact of training, we did not detect significant changes in the control population in terms of IL-10 levels in response to HIIT or HICT training (Fig. 1A–C). However, a significant increase in IL-10 levels was observed in patients with T1D (7.5% increase; p = 0.042) (Fig. 1D). When analyzed by training modality, this increase was specifically observed in the T1D group that underwent the HIIT program (8.8% increase; p = 0.044) (Fig. 1E), while no significant change was detected in the T1D group following HICT (Fig. 1F). These results indicate that changes in IL-10 levels occurred only in response to HIIT, not to continuous training.Fig. 1. Effect of exercise on the anti-inflammatory molecule IL-10 in: A. Control group (both exercise protocols). B. Control group HIIT protocol. C. Control group HICT protocol. D. T1D Group (both exercise protocols). E. T1D group HIIT protocol. F. T1D group HICT protocol. ns p > 0.05. * p < 0.05 when compared using a paired Student’s t-test. Abbreviations: IL-10: Interleukin 10. T1D: Type 1 Diabetes. HICT: Heavy-domain Intensity Continuous Training. HIIT: High-Intensity Interval Training. Preference for color: online only
To evaluate the potential impact of exercise on the initial stages of atherosclerosis, we quantified circulating levels of molecules involved in leukocyte-endothelium interactions. Specifically, we measured P-selectin (which facilitates leukocyte attraction to the endothelium), MPO (a pro-oxidant enzyme released by leukocytes), and the adhesion molecules ICAM1 and VCAM1 (which mediate leukocyte rolling, adhesion, and migration). A comparison between the two pre-intervention groups revealed a trend toward higher ICAM1 levels in patients with T1D (mean 69.59 ± 14.72 control group vs mean 79.71 ± 21.57 T1D group, ng/mL, p = 0.059) (Table 1).
A significant reduction in VCAM1 levels was observed in the control group (8.4% decrease; p = 0.009) (Fig. 2A). When analyzed by training modality, reductions were observed in both subgroups, although these did not reach statistical significance: 5.8% in the HIIT group (p = 0.0838) and 13.1% in the HICT group (p = 0.0593) (Fig. 2B–C). No significant changes in VCAM1 levels were detected in participants with T1D, regardless of training modality (Fig. 2D–F).Fig. 2. Effect of exercise on the adhesion molecule VCAM1 in: A. Control group (both exercise protocols). B. Control group HIIT protocol. C. Control group HICT protocol. D. T1D Group (both exercise protocols). E. T1D group HIIT protocol. F. T1D group HICT protocol. ns p > 0.05. # indicates a trend (p > 0.05 and < 0.1). * p < 0.05. ** p < 0.01 when compared using a paired Student’s t-test. Abbreviations: IL-10 Interleukin 10, T1D Type 1 Diabetes, HICT Heavy-domain Intensity Continuous Training, HIIT High-Intensity Interval Training. Preference for color: online only
Regarding P-selectin, a significant reduction was observed in the control group (13.1% decrease; p = 0.010) (Fig. 3A), specifically in those who performed HIIT (14% reduction; p = 0.044) (Fig. 3B), while no change was observed in the HICT group (Fig. 3C). Among participants with T1D, no significant changes in P-selectin levels were found when data from both training modalities were pooled (Fig. 3D). However, a non-significant trend towards reduction was observed in the T1D subgroup that performed HIIT (Fig. 3E), but not in those who performed HICT (Fig. 3F).Fig. 3. Effect of exercise on the adhesion molecule P-selectin in: A Control group (both exercise protocols). B Control group HIIT protocol. C Control group HICT protocol. D T1D Group (both exercise protocols). E T1D group HIIT protocol. F T1D group HICT protocol. ns p > 0.05. # indicates a trend (p > 0.05and < 0.1)* p < 0.05. ** p < 0.01 when compared using a paired Student’s t-test. Abbreviations: IL-10 Interleukin 10, T1D Type 1 Diabetes, HICT Heavy-domain Intensity Continuous Training, HIIT High-Intensity Interval Training. Preference for color: online only
Correlations between inflammation and vascular adhesion markers and fitness and physical activity parameters
No significant differences were observed between groups at baseline in METs or VO₂max (Fig. 4A–B). To explore potential associations between baseline physical activity or fitness and molecular responses to training, bivariate correlation analyses were conducted across all participants, regardless of training modality or clinical status. A significant negative correlation was found between baseline METs and the change in VCAM1 levels pre- to post-intervention (r = –0.366; p = 0.026) (Fig. 4C). Additionally, a significant negative correlation was observed between baseline VO₂max and the change in P-selectin levels (r = –0.346; p = 0.039) (Fig. 4D).Fig. 4. Relationship between physical activity and fitness levels at baseline and changes in adhesion molecules. A. Comparison between control and T1D subjects ‘ METs at baseline. B. VO_2_max at baseline in controls and subjects with T1D. C. Correlations between the exercise-induced changes in VCAM1 (Δ) and baseline METs. D. Correlation between exercise-induced changes in P-selectin (Δ) and baseline VO_2_max. Δ indicates post – pre values. Abbreviations: METs Metabolic equivalents, VCAM1 Vascular cell adhesion molecule 1, P-selectin Platelet Selectin, VO2max maximal oxygen uptake. Preference for color: online only.
Discussion
Our results showed that patients with T1D had lower concentrations of IL-10 and a tendency toward higher concentrations of ICAM1, indicating a reduced anti-inflammatory capacity and an increased risk of atherosclerosis (Carlos and Harlan 1994). HIIT has been shown to enhance the anti-inflammatory capacity of IL-10 in patients with T1D, where this capacity typically declines as the disease progresses (dos Santos Haber et al. 2023). IL-10 is crucial for reducing the presence of antigens and the production of pro-inflammatory cytokines (Saraiva et al. 2019), and its decrease contributes to the inflammatory profile in patients with T1D, exacerbating the interaction between the immune system and pancreatic β cells (Cnop et al. 2005). The myokines released by the muscle have been shown to have an anti-inflammatory effect, and the amount of myokines released is related to the intensity of the exercise (Pedersen 2017; Scheffer and Latini 2020). However, previous studies suggest that strenuous exercise may have the opposite effect, potentially increasing inflammation (Balan and Locke 2011), indicating that the benefits of exercise depend on its modality, frequency, intensity, and duration. These findings suggest that HIIT may contribute to improving the anti-inflammatory profile in individuals with T1D, which could be of relevance in the context of disease progression. Additionally, this increase in IL-10 was observed significantly only in patients with T1D, suggesting that these exercise protocols, especially HIIT, may play a “restorative” role in the levels of this cytokine. This may explain why control subjects, who started with higher baseline IL-10 levels, did not show a significant increase after training.
Regarding adhesion molecules, no significant differences were found between control subjects and subjects with T1D, although there was a tendency for higher ICAM1 levels. These results differ from the current literature (Gogitidze Joy et al. 2010; Iannantuoni et al. 2020), which reports that patients with T1D present higher levels of adhesion molecules such as P-selectin, VCAM1, and ICAM1. Such discrepancies could potentially be related to differences in disease management across cohorts, including factors like glycemic control or time in range, among others, which were not assessed in our study but may influence inflammatory and endothelial markers. This hypothesis is supported by previous studies showing that glycemic control and glucose variability can modulate endothelial function and the expression of adhesion molecules (Cacace et al. 2025).
Physical exercise can protect against the risk of atherosclerosis by reducing the levels of adhesion molecules VCAM1 and ICAM1 (Palmefors et al. 2014). Moreover, exercise improves blood pressure and arterial stiffness (Park et al. 2020), which are closely related to the risk of atherosclerosis. In our study, exercise in the control group reduced P-selectin and VCAM1 concentrations, with specific effects depending on the type of training. HIIT decreased P-selectin levels, while HICT tended to reduce VCAM1 levels. These results suggest that exercise intensity and/or duration may influence the regulation of these molecules, potentially aiding in the prevention of atheroma plaque formation (Krieglstein and Granger 2001).
A systematic review by Palmefors et al. (2014) summarized studies about the effects of physical activity or exercise on cytokines, chemokines, adhesion molecules, CRP or angiogenic factors, and ranked them based on the quality of evidence. Interestingly, this analysis showed that the evidence for a reduction in VCAM1 is moderate, high for ICAM1, and insufficient for P-selectin. Similar to our finding of limited reductions in adhesion molecules, Madsen et al. (2015) found no significant differences in adhesion molecules after an 8-week low volume HIIT intervention in either controls and subjects with type 2 diabetes, despite functional and structural vascular improvements (Madsen et al. 2015). Studies showing greater reductions in these molecules typically involve longer or more frequent training sessions (Adamopoulos et al. 2001; Roberts et al. 2006). This suggests that prolonged or frequent exercise protocols could lead to a general reduction in these molecule levels. Other studies that found profound effects of this type of training on inflammatory and adhesion molecules were performed in subjects with underlying pathologies involving endothelial dysfunction, such as chronic heart failure (Larsen et al. 2001; Niebauer et al. 2005). Our population with T1D consists of young, non-obese subjects with absence of any cardiovascular diseases, therefore, baseline levels of cardiovascular disease biomarkers (such as inflammatory and adhesion molecules) are not as elevated as in the aforementioned studies (Larsen et al. 2001; Niebauer et al. 2005). This could, at least in part, explain the similar levels of inflammation and adhesion molecule levels between controls and T1D and the lack of effect of the different exercise training interventions in patients with T1D.
Our study reveals that subjects’ baseline physical fitness and activity levels may be important factors determining the degree of improvement in adhesion molecule levels, which are cardiovascular disease biomarkers. Those subjects with greater baseline VO_2_max achieve greater reduction in P-selectin levels with training. In addition, in subjects that were more physically active before the training period (greater metabolic equivalent units), levels of VCAM1 were further reduced by training. In this sense, Bellos et al. (2023) showed that total physical activity, estimated as daily time spent stepping, was negatively associated with VCAM1, ICAM1 and endothelial-leukocyte adhesion molecule in a cohort of subjects with and without diabetes. Independently of adhesion molecule levels, interaction between peripheral blood mononuclear cells and endothelial cells improved after a 20-min treadmill exercise at 65–70% peak oxygen consumption in healthy subjects (Mills et al. 2006). Interestingly, this occurred only in those subjects considered fit, in terms of median VO_2_max levels, and not in less-fit subjects (Mills et al. 2006). Therefore, being physically active and having a good physical fitness seem to predispose individuals to achieve greater benefits on the vascular system.
This study has some limitations. The control and T1D groups were not strictly matched for age and sex, and there was a trend toward higher BMI and body mass in the control group, which could have influenced some of the results. Additionally, the short duration of the intervention may have limited the magnitude of detectable changes in certain biomarkers. Another limitation is the absence of C-reactive protein measurement, a widely used and sensitive marker of systemic inflammation, which could have provided complementary information to the cytokine and adhesion molecule data.
Nonetheless, our findings suggest that exercise-induced changes in circulating pro- and anti-inflammatory cytokines and CAMs may vary depending on the type of training and the population studied. Furthermore, the baseline physical activity and fitness levels appear to be associated with individual variability in response to exercise in terms of cardiovascular disease-related markers. Future studies are needed to address the specific immune cell responses and adaptations triggered by HIIT and HICT training that improve vascular health, potentially preventing cardiovascular diseases.