Impact of pulsed stimulation on objective and subjective visual acuity measurements in nystagmus
Elisabeth V. Quanz, Khaldoon O. Al-Nosairy, Francie H. Stolle, Juliane Kuske, Sven P. Heinrich, Michael Bach, Michael B. Hoffmann

TL;DR
This study found that pulsed stimulation does not explain why visual acuity estimates from VAVEP are higher in people with nystagmus.
Contribution
The study clarifies that pulsed stimulation is not the cause of VAVEP overestimation in nystagmus.
Findings
VAPsych_Pulsed and VAPsych_Stat did not differ significantly in participants with nystagmus.
VAVEP estimates were significantly higher than both VAPsych_Pulsed and VAPsych_Stat.
Fixation instability was not correlated with differences in psychophysical visual acuity measurements.
Abstract
Quanz et al. (Sci Rep 14:16797, 2024) reported that participants with nystagmus had higher objective visual evoked potential visual acuity estimates (VAVEP) by 0.12 logMAR relative compared to standard psychophysical VA (VAPsych_Stat). The cause of this modest, but significant VAVEP overestimation remains unclear. Here we investigated its association with the pattern-pulse stimulation mode applied for steady state VEP recording for VAVEP estimation. Specifically, we tested whether psychophysical visual acuity to pulsed optotypes (VAPsych_Pulsed) also exceeds standard optotype VAPsych_Stat. Twelve participants with nystagmus were included in this analysis. VAVEP was determined for pattern-pulse steady-state VEP stimulation (Quanz et al. in Sci Rep 14:16797, 2024) using EP2000, psychophysical VA was determined to stationary (VAPsych_Stat) and to pulsed (VAPsych_Pulsed) Landolt-C…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
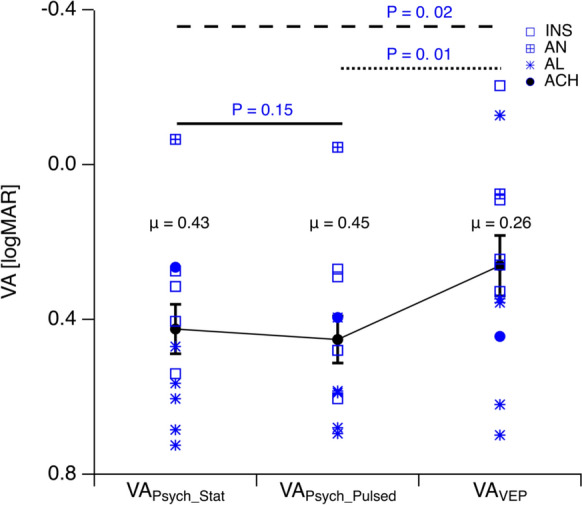 Figure 1
Figure 1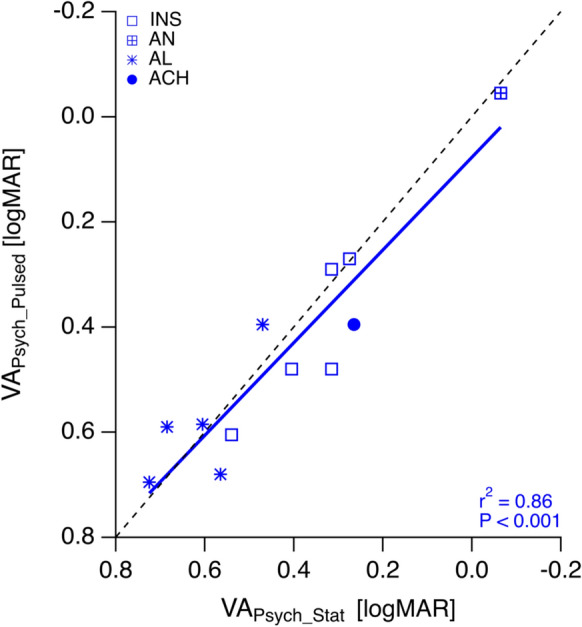 Figure 2
Figure 2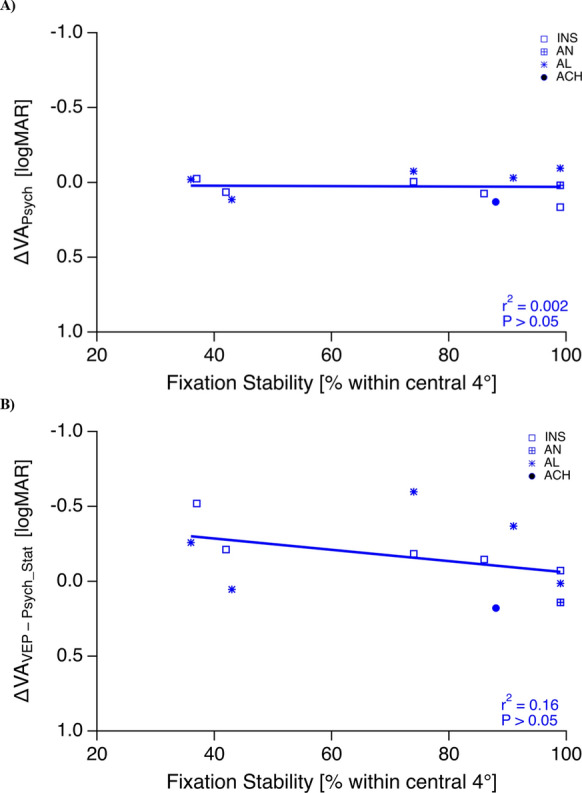 Figure 3
Figure 3- —https://doi.org/10.13039/501100001659Deutsche Forschungsgemeinschaft
- —Otto-von-Guericke-Universität Magdeburg (3121)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVestibular and auditory disorders · Visual perception and processing mechanisms · Multisensory perception and integration
Introduction
Objective estimation of visual acuity (VA) is of paramount importance in ophthalmology particularly when standard psychophysical VA (VA_Psych_) might be unfeasible or unreliable. Visual evoked potential based-assessment of visual acuity (VA_VEP_) is regarded to provide a relevant option to obtain objective VA estimates [1, 2]. Still, VEP-based VA estimation is facing challenges in certain conditions e.g., amblyopia [3, 4]. Recently, Quanz et al. [5] reported a small but significant VA_VEP_ overestimation in nystagmus, by on average 0.12 logMAR compared to VA_Psych_, that depended on the degree of fixation instability. In that study VA_VEP_ was estimated with pattern-pulse stimulation, VA_Psych_ with static optotypes. In fact, VEP responses to pulsed stimuli are less reduced by nystagmus-like stimulus movements than those to non-pulsed (pattern-reversal) stimuli [6]. This prompts the question whether the VA_VEP_ overestimation in nystagmus is due to the pulsed stimulation mode. For psychophysical grating acuity, pulsed and non-pulsed conditions have been compared and no difference has been found [7]. Critically, for optotype acuity, this has not yet been investigated. We aimed to fill this gap and tested the hypothesis whether pulsed optotypes yield better VA-values (VA_Psych_Pulsed_) than static (VA_Psych_Stat_), i.e., that the stimulation mode accounts for the mismatch of VA_VEP_ and the routinely acquired VA_Psych_Stat_.
Methods
This study included participants from Quanz et al. study [5], where a detailed record on the procedures is given. It followed the guidelines of the Declaration of Helsinki, and was approved by the Ethics Committee of the Faculty of Medicine, Otto-von-Guericke University, Magdeburg (153/18). All participants gave written informed consent.
Participants
For this study, we included data from 12 participants (mean and range of age: 39, 20 − 63y; only the individual’s eye with stronger fixation instability was included) with nystagmus from the Quanz et al. cohort [5], for whom also VA_Psych_Pulsed_ data were available, that had previously not entered analysis and publication. For patient characteristics see Table 1. Causes of nystagmus were idiopathic infantile nystagmus syndrome (INS; n = 5), albinism (AL; n = 5), achiasma (ACH; n = 1) or acquired nystagmus (AN; n = 1). Epilepsy, dizziness, and any eye diseases affecting visual function, e.g., diabetic retinopathy, were exclusion criteria.Table 1. Participant characteristicsIDGroupSexAge [years]Nystagmus TypeStereopsis*BCVA [logMAR]Eye†Fixation ± 2° [%]1INSf21J/HNo0.54OD422INSf42J/HNo0.41OD863INSm29P/HNo0.32OS374INSf56J/HNo0.32OS995INSm51J/HYes0.28OS746ANf42J/HYes-0.07OD997ALf23J/HNo0.47OD748ALm51J/HNo0.73OS919ALm63J/HNo0.69OS9910ALf20J/HNo0.61OS3611ACHm22J/HNo0.27OS8812ALm40J/HNo0.57OD43INS, idiopathic infantile syndrome (excluding albinism and achiasma); AN, acquired nystagmus (cause: hydrocephalus shunt surgery); AL, albinism; ACH, achiasma; f, female; m, male; J, jerk, P, pendular, H, horizontal; *Stereopsis test using Lang test; BCVA [logMAR], best corrected visual acuity in logarithmic minimal angle of resolution; Eye†, eye with stronger fixation instability; OD, right eye; OS, left eye
VAVEP estimation
Participants wore appropriate refractive correction, procedures followed ISCEV recommendations [1]. The VEP was recorded separately for each eye twice and averaged across repetitions. Freiburg Evoked Potential EP2000 allows for stimulation, recording and analysis of the VEP. Two monitors were used, one viewed by the participant and the other for data monitoring. VEP check-size dependence (size range: 0.048–0.8°) was determined for pattern-pulse steady-state (ss)- VEP stimulation (40 ms on/93 ms off, 7.5 Hz; 50 cd/m^2^ mean luminance and 40% contrast) at a viewing distance of 114 cm as described in Quanz et al. [5] using EP2000 [8]. Signals were 100 k-times amplified and band-pass filtered (0.3, 70.0 Hz low and high cut-off). Subsequently, responses were digitally filtered with a low-pass cutoff of 40 Hz. The VA_VEP_ estimation followed Bach et al. [9]. For each checksize, the spatial frequency was determined (SF [cpd] = 1/√2 × check size). The responses and their significance levels were calculated for each SF. VEP amplitudes and significance-levels at the stimulation frequency were determined with a Fourier-analysis based approach [10–12] and subjected to a heuristic algorithm to determine the spatial frequency limit for VA_VEP_ estimation. The previously published stepwise heuristic algorithm [9] was used to determine the upper SF limit (SF_0_) by extrapolating the log amplitude response to zero [5]. SF_0_ was converted to VEP acuity with an acuity-independent conversion factor [9] [decimal VA_VEP_ = SF_0_/17.6 cpd, which corresponds to logMAR VA_VEP_ = log (SF_0_/17.6 cpd)].
VAPsych estimation
Both best-corrected VA_Psych_Stat_ and VA_Psych_Pulsed_ were determined twice (18 trials per measurement) for testing at 114 cm using the Freiburg Vision Test (FrACT) with Landolt C optotypes [13]. Pulsed stimulus timing for VA_Psych_Pulsed_ was identical with the VEP pulsed mode (40 ms on / 93 ms off, 7.5 Hz; 102 cd/m^2^ mean luminance and 96% contrast).
Microperimetry – Fixation stability
The fixation stability within the central 4° was quantified using a fundus-controlled microperimeter (MP-1 microperimeter, Nidek, Padova, Italy). The fundus-motion was tracked at 25 Hz for an epoch of 30 s, where participants were asked to fixate a central target.
Analysis and statistics
Normality was confirmed with the Shapiro–Wilk test and consequently parametric statistical testing was applied. One-sided paired t-tests were employed to determine whether VA_Psych_Pulsed_ exceeded VA_Psych_Stat_ and VA_VEP_ exceeded VA_Psych_ estimates. Pearson correlation (r^2^) explored how ΔVA_Psych_ (VA_Psych_Pulsed_ – VA_Psych_Stat_) depended on fixation instability within the central 4°.
Results
An overview of the mean VAs, VA_Psych_Stat_, VA_Psych_Pulsed_, and VA_VEP_ is given in Fig. 1. We observed a significant overestimation of VA_VEP_ (0.26 ± 0.08 logMAR) compared to both VA_Psych_Stat_ (0.43 ± 0.06 logMAR, P = 0.02) and VA_Psych_Pulsed_ (0.45 ± 0.06 logMAR, P = 0.01). Notably, VA_Psych_Pulsed_ and VA_Psych_Stat_ did not differ significantly from each other (P = 0.15) and were highly correlated with each other (r^2^ = 0.86, P < 0.001, Fig. 2). Finally, neither did the difference between VA_Psych_Pulsed_ and VA_Psych_Stat_, nor that between VA_VEP_ and VA_Psych_Stat_ correlate with the degree of fixation instability (ΔVA_Psych_, r^2^ = 0.002, P = 0.89; ΔVA_VEP_—VA_Psych_Stat_, r^2^ = 0.16, P = 0.21, Fig. 3 A & B).Fig. 1. Overview of VAs. (INS: idiopathic infantile syndrome); AN, acquired nystagmus (cause: hydrocephalus shunt surgery); AL, albinism; ACH, achiasma; note inverted y-axis such that better VAs are at top. The average VA (μ) is also shown for each stimulus typeFig. 2Correlation of VA_Psych_Pulsed_ vs. VA_Psych_Stat_. Both VA measures were highly correlated. For abbreviations see Fig. 1. Dotted line indicates the line of identity; note inverted axes such that better VAs are at topFig. 3Correlation of fixation stability vs (A) ΔVA_Psych_ = VA_Psych_Pulsed_ − VA_Psych_Stat_ [logMAR] and (B) VA_VEP_ − VA_Psych_Stat_ [logMAR]. No significant correlations were observed. For abbreviations see Fig. 1a
Discussion
We found similar psychophysical visual acuities (VA_Psych_) for static and pulsed optotypes in nystagmus patients, and no dependence on the degree of fixation instability. It is concluded that the previously observed mismatch of VA_VEP_ and VA_Psych_ in nystagmus is not related to the difference in stimulation mode between standard psychophysical VA estimation (‘static’) and VEP based estimation (‘pulsed’).
While we are, to our knowledge, the first to compare psychophysical VA for static vs pulsed optotypes stimulation in nystagmus patients, there is a previous investigation of this issue for psychophysical grating acuity [7]. Dunn et al. report similar findings to the present study; they compared psychophysical static grating VA to tachistoscopically flashed (0.76 ms) patterns and failed to find a difference in nystagmus and healthy controls. Taken together, it appears that pulsed stimulation does not affect psychophysical VA estimates in nystagmus. The lack of comparison to healthy controls and small sample size are a limitation of the present study. Further, the generalizability of the findings across individual subtypes of nystagmus remains limited due to small sizes of subtypes, e.g., albinism. In conclusion, the stimulation time course does not appear to be an explanation of the VA_VEP_ overestimation in nystagmus. In search of an alternative explanation, it should be noted that VEP stimulation employs extended patterns, namely checkerboards, as opposed to optotype stimulation in VA_Psych_ measurements.
Taken together, our report indicates the need for further research into the mechanisms contributing to the slight, but significant VA_VEP_ overestimation in nystagmus given the absence of an effect of pulsed stimulation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bach M. Visual Evoked Potentials “EP 2000” – Computer system by Michael Bach. 2007. https://michaelbach.de/sci/stim/ep 2000/ (Accessed 8 Jan 2025)