The influence of oral health on sports performance: an interdisciplinary perspective
Karsten Hollander, Inbar Eshkol-Yogev, Astrid Zech, Jacopo Buti, Ian Needleman

TL;DR
This paper explores how oral health impacts athletic performance and suggests that better dental care can improve endurance, strength, and agility in athletes.
Contribution
The paper introduces the idea that oral health is a modifiable factor influencing sports performance, supported by interdisciplinary collaboration.
Findings
Poor oral health is linked to reduced performance metrics like VO2 max and agility.
Oral health issues may affect performance through inflammation, nutrition, and psychological factors.
Dentists should work with sports teams to improve athlete performance and recovery.
Abstract
Sports performance is a multifactorial concept determined by the interplay of physical, technical, tactical, and psychological factors. While its measurement is straightforward in metrical sports (e.g., athletics or swimming), it is more complex in team or aesthetic disciplines. In recent years, the role of oral health has gained attention as a potentially modifiable factor influencing athletic performance. This paper provides a comprehensive overview of how sports performance is defined and measured – particularly in explosive and endurance sports – and explores the impact of oral health on performance outcomes. Evidence from systematic reviews and observational studies shows consistent associations between poor oral health (e.g., periodontal disease, caries, malocclusion) and reduced objective performance metrics such as V̇O2 max, power output, speed, and agility, as well as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
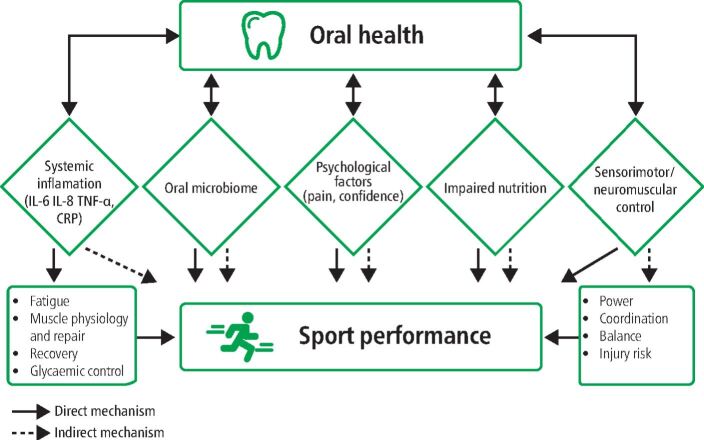 Figure 1
Figure 1- —MSH Medical School Hamburg - University of Applied Sciences and Medical University (5121)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Trauma and Treatments · Dental Health and Care Utilization · Muscle metabolism and nutrition
Introduction
Sports performance is determined by a complex interaction of physical, technical, tactical, and psychological skills that are further influenced by physiological, biomechanical and cognitive factors.^1^ For most athletes, maximising performance in their specific sport is fundamental to their training, preparation, and daily routines. While the requirements for optimal performance widely differ between the range of sports, athletes typically aim to have optimal performance in competitions. In metrical sports like athletics (track and field) or swimming, it is straightforward to quantify performance by time (e.g., sprint or marathon) or distance (e.g., jumping or throwing). In other sports, such as team or aesthetic disciplines, assessing performance is more complex. In team sports, success depends on a combination of individual physical performance, sport-specific skills, and tactical execution, with team outcomes not always reflecting individual achievement. In aesthetic sports, performance evaluation can vary substantially between disciplines – for example, in equestrian dressage, artistic impression and technical precision are judged, whereas in bodybuilding, assessment focuses on physique and muscular definition – highlighting the diverse criteria that extend beyond a single peak performance on a specific date. Therefore, this paper will focus on objective measures of physical performance.
The world-class and elite athletes (tiers 4 and 5 as defined by McKay et al.)^2^ are typically supported by an interdisciplinary team of coaches, exercise scientists, physiotherapists, nutritionists, psychologists and sports physicians.^3^^,^^4^ In this interdisciplinary approach, sports dentistry has developed an increasingly important role, contributing to overall health and well-being.^5^^,^^6^ For instance, a feasibility study in Great Britain Cycling, Rowing and a Premiership Rugby Union team demonstrated that a simple oral health intervention, delivered to athletes and support staff, was associated with improved oral health behaviours and reduced self-reported performance impacts.^7^
Therefore, our aim is to provide a comprehensive overview of what sports performance is, how it can be measured and how oral health influences sports performance. As sports performance is a broad field, we will focus on sports-specific skills, physical and psychological factors, as well as biomechanics in the context of explosive sports, characterised by short-duration, high-intensity efforts (e.g., sprinting, weightlifting), and endurance sports, which require prolonged, submaximal exertion supported by aerobic capacity (e.g., long-distance running, cycling). Then, we will elaborate on the (possible) mechanisms and outline how practice and sports dentistry research should incorporate performance measurements to further advance the knowledge in the areas of oral health and sports performance.
What is performance in sport and how is it measured?
Key components of sports performance
Sports performance is complex and strongly influenced by sport-specific skills and individual physical and psychological characteristics. While the main components of sports-specific skills refer to techniques and tasks that develop over a longer period of motor learning and practising, the physical and psychological characteristics are influenced by multiple modifiable and non-modifiable (e.g., anthropometric, hormonal) factors. Modifiable physical factors can be categorised into strength, power, speed, endurance, flexibility and agility, and typically adapt to adequate training stimuli.^8^ Most muscular and cardiorespiratory adaptations are temporary and require a well-coordinated interaction of regular (overload) exercising and recovery periods as well as hydration and nutrition.^9^^,^^10^^,^^11^^,^^12^^,^^13^ Psychological factors have been linked to athletic performance, including evidence of an association between psychopathology and performance outcomes.^14^ Furthermore, self-motivation, cognitive capacity, emotional intelligence, coping skills and mindfulness interventions have been shown to influence sports performance.^15^^,^^16^^,^^17^ In the context of sports-specific performance, biomechanics can determine the role of movement efficiency, for example, how efficiently the centre of mass can be transported by the musculoskeletal system from point A to B. Biomechanics analyses the mechanical principles of movement, while the sensorimotor system provides the sensory input and motor output that enable and refine these movements, making the two intrinsically interdependent in sports performance. It also analyses the underlying (inertia, velocity-based and reactive) forces associated with muscle strength-related and coordinative aspects of movement. Accordingly, sports biomechanics considers three-dimensional aspects of movements and forces and are quantified by kinematical, kinetical and spatiotemporal parameters.^18^
Analysing performance in metrical sport
Measuring metrical sports performance is quite straightforward as they are typically quantified by a metric number per unit. For example, in athletics, performances in all disciplines are measured in time or distance, and the respective values can even be compared with previous data, other athletes or norms (e.g., World Athletics score).^19^
However, analysing the effects of performance-related interventions (training, nutrition, materials) and underlying mechanisms of muscular, cardiorespiratory, or metabolic adaptations is more complex.^20^^,^^21^ Multiple objective and subjective (e.g., perceived exertion, fatigue or questionnaires) measures can be used and combined to analyse internal load as well as training-related changes for endurance, strength, speed and power.^22^
The spectrum of tests for endurance performance includes standard laboratory measurements such as the V̇O₂ max test on a (running, rowing, or cycling) ergometer to estimate endurance capacity or field-based tests (e.g., 20 m shuttle run test, Yo-Yo Intermittent Test).^23^^,^^24^ They can analyse subcategories of performance, such as aerobic (e.g., running economy) or anaerobic (e.g., lactate threshold, power tests) capacities.
Explosive strength and power performances can be measured through a variety of tests, including sprint and jumping tests. A standard test for muscle force capacities is the one-repetition maximum test, which is defined by the weight which can be lifted once over the full range of motion. Force-time curves of maximal or submaximal isokinetic dynamic or isometric muscle contractions can help to analyse explosive or endurance aspects of strength.^22^
Further crucial tests for athletes' performances are agility tests. These tests generally combine sprinting abilities with several change-of-direction manoeuvres and challenge the braking and generating forces of the body while maintaining momentum.^25^ These movements occur in team, racket and combat sports. The most used tests are the Agility T-Test and the Illinois Agility Test; although, a vast range of sport-specific tests can be found in the literature.^26^
What do we know about the effect of oral health on modifiable parameters of sports performance?
Associations between oral health and sports performance: evidence from systematic reviews and meta-analyses
A recent systematic review and meta-analysis involving 396 athletes has examined the link between athletic performance and periodontal diseases.^27^ They found moderate strength of evidence for a relationship between periodontitis and self-reported reduction in sports performance and concluded that although performance evaluations differed across studies, periodontal diseases significantly correlated with lower self-reported sports performance. In another review, Bramantoro et al. (2020)^28^ evaluated the relationship between oral health and objective performance tests, including athlete and non-athlete populations. Of the eleven high-quality studies included, ten reported statistically significant associations between oral health and modifiable performance outcomes (physical fitness, body balance, cardiorespiratory function, and cognitive function). Physical fitness was mainly associated with malocclusion, periodontitis, and periapical inflammation. Endodontic disease alone was not found to be associated with poor physical performance. The review supports the negative effect of poor oral health on physical fitness and performance. Ashley et al. (2015)^29^ investigated the oral health impact on sporting performance in athlete populations. The systematic review included 34 studies, and the methodological quality of the included studies was reported as generally low. High prevalence of oral diseases was found (dental caries 15–75%, dental erosion 36–85%, periodontal disease 15%). The negative impact of oral health or trauma on performance was reported in four studies (with range of 5−18%).
Oral health impacts parameters of aerobic, anaerobic and neuromuscular performance
Multiple studies support the hypothesis that poor oral health may adversely affect various dimensions of sports performance. Merle et al. (2022) explored interactions between signs of periodontal inflammation and systemic parameters in world-class and elite German athletes (tier 4 and 5),^2^ defined as members of German youth or senior national squads. They assessed sports performance using an ergometer and maximal aerobic capacity quantified by V̇O_2_ max (Table 1 ).^30^^,^^31^^,^^32^^,^^33^^,^^34^^,^^35^^,^^36^^,^ ^37^^,^^38^^,^^39^^,^^40^^,^^41^^,^^42^^,^^43^^,^^44^^,^^45^^,^^46^^,^^47^^,^^48^^,^^49^^,^^50^^,^^51^^,^^52^^,^^53^ The periodontal condition affected both V̇O_2_ max values and cycling ergometer performance: Athletes with signs of periodontitis (Periodontal Screening Index[PSI] ≥3) recorded a potentially important 5.7% lower mean V̇O_2_ max value compared to those with PSI ≤2 (55.9 ± 6.7 mL/min/kg versus 59.3 ± 7.0 mL/min/kg; p = 0.03). A similar trend was observed in ergometer tests, where better performance was achieved in athletes with a lower level of signs of periodontal inflammation (Papilla Bleeding Index (PBI) <0.42) who consistently reached higher maximal power on the cycling ergometer (5.0 ± 0.5 W/kg versus 4.4 ± 0.3 W/kg; p = 0.03). Potential associations were found between performance, body composition, blood parameters, and signs of periodontal inflammation.^30^Table 1 Summary of commonly used tests of modifiable factors (endurance, sprint, and power) of sports performance and their reported associations with oral healthTestDescriptionTest typeEvaluation with oral healthEnduranceV̇O_2_ max testMeasures maximal oxygen uptake via graded treadmill or cycle test with gas analysis^32^LabWorse periodontal health associated with lower VO_2_ max and relative load output in elite and world-class athletes^30^Lactate threshold testIdentifies the point where blood lactate rises sharply, useful for setting training zones^33^LabNo statistically significant association with periodontal status in elite and world-class athletes^30^Running economyMeasures oxygen consumption at submaximal speeds; indicates efficiency^34^^,^^35^LabNACritical speed testEstimates sustainable high-intensity running speed using multiple time trials^36^FieldNACooper 12-minute run testDistance covered in 12 minutes; estimates VO_2_ max^37^FieldNA1.5-mile run testEstimates VO_2_ max from time taken to run 1.5 miles (2.4 km)^38^FieldNAYo-Yo Intermittent TestAssesses endurance and recovery in high-intensity intermittent sports^39^FieldHighly-trained/national-level adolescent basketball players with poor oral hygiene presented a lower value at pre- and post-Yo-Yo Intermittent Recovery Test Level 1 compared to good oral hygiene group^40^Time Trials (e.g., 3 km, 5 km, 10 km…)Race-like trials that estimate race fitness and endurance capacity^41^FieldNABeep testProgressive shuttle run with increasing pace; estimates VO_2_max^42^FieldNASprint and powerLinear sprint testsMeasures acceleration and/or maximal sprinting speed; can be divided into splits (e.g., 5 m, 10 m, 20 m…) and start can be performed standing or flying^43^Field/labSpeed test results showed that athletes with better oral health (DMFT <4) outperform those with worse oral health (DMFT ≥4) in speed tests (10-, 20-, 30 m sprints) (p <0.05). Success rates dropped as DMFT values increased with longer completion times^31^Vertical jump test (CMJ, SJ), jump powerMeasures lower-body power using jump height or power; often with force plate or jump mat^44^^,^^45^Field/labHigher% PPD >4 was consistently correlated with lower CMJ height average in law enforcement workers^46^Standing long jumpMeasures horizontal explosive leg power,^47^ frequently used in youth^48^^,^^49^FieldNAWingate anaerobic test30-second all-out cycling test to measure anaerobic power and fatigue index^50^LabDental caries and a high DMF-T index value did not significantly affect athletic performance^51^Isokinetic dynamometryMeasures peak torque and muscle strength across joint angles^52^LabNAForce-velocity profiling (e.g., sprint force-velocity test)Analyses sprint mechanics to determine optimal power output^53^Field/labNACMJ, countermovement jump;,DMFT, Decayed Missing and Filled Teeth; NA, not applicable; PPD, probing pocket depth; SJ, squat jump
Similarly, Yapici et al. (2019)^31^ investigated the relationship between oral health and sporting performance in athletes (no tier stated) in Turkey. Little information was provided on the definition of athletes; although, they were reported as having a mean age of 20.4 years (± 1.3 years), training for 6–8 hours per week and actively involved in sport for 6.6 years (± 2.6 years). Oral health was evaluated by Decayed, Missing, Filled Teeth (DMFT), Significant Caries Index and Plaque Index. Sports performance included t-drill, zig-zag, lateral change of direction (LCD) and 505 tests to assess agility, as well as 10, 20 and 30 m short sprint tests to assess speed. Athletes with DMFT <4 performed better in the agility tests and speed tests than athletes with DMFT ≥4, with all tests showing statistically significant differences. Increased DMFT values were associated with extended times of agility and speed tests. A positive low to moderate correlation was found between DMFT and agility tests [t-drill test (r = 0.428), zig-zag test (r = 0.428), LCD test (r = 0.286) and 505 test (r = 0.529)], and speed tests [short sprint, 10 m (r = 0.309), 20 m (r = 0.336), 30 m (r = 0.449) (p <0.05)].
Oral health impacts wellbeing, sports participation, food intake and self-reported sports performance
Several cross-sectional studies have used self-reported questionnaires to evaluate the impact of oral health on daily activities, quality of life and sports performance among athletes (Table 2).^54^^,^^55^^,^^56^^,^^57^^,^^58^^,^^59^^,^^60^^,^^61^ The studies described in Table 2 were conducted in Nigeria, Brazil, Pakistan, the Netherlands, and the UK. The most common oral conditions assessed were dental caries (DMFT), periodontal health (Basic Periodontal Examination/Community Periodontal Index of Treatment Needs), and erosive tooth wear (Basic Erosive Tooth Wear Examination). The studies included athletes from various sports, such as table tennis, lawn tennis, badminton, cricket, cycling, baseball, basketball, and hockey, including the Olympic and Paralympic Games. However, descriptions of the athlete groups and tiers were inconsistently reported across studies. Overall, the prevalence of oral health conditions was consistently high, with dental caries reported up to 63.5%^57^ and gingivitis up to 77%.^56^ Across the reviewed studies, the impact of oral health on daily activities and self-reported sports performance was noted in most studies; although, the strength of evidence is limited by the use of unvalidated tools. Wide variation was found in the tools assessing athletes' perception and psychosocial and performance impact, with some studies using unvalidated self-administered questionnaires, while only a few were based on validated tools such as the Oral Health Impact Profile-14 or Oral Impact on Daily Performance.^62^^,^^63^ The impact on daily activities and performance included pain, difficulty eating or drinking, and effects on quality of life. More direct effects on sports performance and training included challenges participating in regular training and competition, performance affected in competitions, and a reduction in training volume. However, due to methodological limitations and the use of non-validated tools, the strength of evidence remains moderate to low.Table 2 Oral health impacts daily activities and self-reported sports performanceAuthor (year)CountryOral health conditions assessedPopulation, tier according to McKay et al. ^2^Self-reported sports performance****Validated (yes/no)Oral health outcomesEffect on sports performance and daily activityAzodo (2013),^54^NigeriaCaries, toothache, gingival bleeding and mouth ulcerAthletes participated in the 2011 Nigerian University Games (n = 226), tier 3Self-administered questionnaire(no)The prevalence of oral health problems was 28.3% (dental caries 53%). A total of 106 experienced toothache (46.9 %), gingival bleeding (36.3 %) and mouth ulcer (40.7 %)15.9% had experienced a dental problem during competitions, with 66.7 % reporting that the dental problem affected their performance in the competitionFrontera (2011),^55^BrazilOrofacial injury/trauma,mouth breathingBrazilian Basketball Confederation Championships (n = 388); tier 3Self-administered questionnaire(no)50% of athletes reported orofacial injuries, with dental trauma in 69.7%. The maxillary central incisors were the most affected, followed by soft tissue injuries (60.8 %), with lip injuries being the most prevalent22.3% related that an oral problem might cause them to stop training or playing, and 66% were aware that this could affect their physical strengthKhan et al. (2022),^57^PakistanDMFT, BPE, BEWEElite Pakistani athletes who competed in any sports (athletics, table tennis, lawn tennis, badminton, cricket, cycling, baseball, basketball, hockey) at college/university, at a national or international level (n = 104), tier 3 and 4Self-reported questionnaire fororal health and psychosocial and performance impact (no)Mean DMFT score was 2.7 ± 3.3, 63.5% had at least one carious tooth, BPE: 46.1% had gingivitis (BPE 1–2), and irreversible periodontitis (BPE score = 3–4) was present in more than a quarter of the athletes64.4% reported difficulty with at least one daily activity due to problems in their mouth, teeth or gums. 47.1% reported difficulty eating or drinking, with 42 (40.4%), 37 (35.5%), and 38 (36.5%) reporting that oral health problems led to difficulty in relaxing, participating in sports, and smiling without embarrassment, respectively. Regression analyses revealed a significant association between BPE and impact on both daily activities and sports performanceKragt (2019),^58^NetherlandsDMFT, BEWE, DPSIDutch elite athletes eligible for the Olympic and Paralympic Games in Rio de Janeiro 2016 (n = 116); tier 4 and 5OHIP-14 questionnaire(yes)In 43.0% of the athletes, clinical findings were reported with 19.8% dental decay, 21.6% with gingivitis and 0.9% with periodontitis. 15 % of all athletes had a DMFT score >10, which indicates poor oral health and 43% were in need for dental treatment3% of the athletes missed one training or competition due to their oral health. 27.3% reported oral health has impacted their quality of life.Although, 90% reported that their oral health has never affected their training, only 28.2 % of the athletes reported to have never problems with their mouthGallagher (2018),^56^UKICDAS, BEWE, BPEOlympic athletes (n = 352),256 athletes on podium potential/placement programmes for the 2016 Rio Olympic Games and 96 professional athletes; tier 4 and 5OIDP questionnaire^61^(yes)Caries and ETW were found in 49.1% and 41.4% of athletes, respectively. Gingival bleeding on probing or calculus (BPE 1/2) in 77.0% and pocket probing depths of ≥4 mm (BPE 3/4) in 21.6%. The odds of having caries in team sports were 2.4 times greater than endurance athletes. The odds of having erosion were two times greater in team sport than endurance sport110 (32.0 %) athletes reported an oral health-related impact on sport performance: oral pain (29.9 %), difficulty participating in normal training and competition (9.0 %), performance affected (5.8%) and reduction in training volume (3.8%). Other impacts were difficulty with eating (34.6%), relaxing (15.1%) and smiling (17.2 %). Several oral health problems were associated with performance impactsNeedleman (2016),^59^UKDental caries, BEWE, BPE, PUFA IndexProfessional soccer players(n = 187); tier 4 and 5Shortened global evaluation of impact of oral health on quality of life^61^36.9% players had dental caries, 53% dental erosion, Gingivitis in 80% and 5% had moderate-severe irreversible periodontal diseaseMore than 45% of footballers were bothered by their oral health with 19.6% reporting an impact on their quality of life and 6.9% reporting an impact on training or performance. Dentine caries had a highly statistically significant association with athlete-reported impactsNeedleman (2013),^60^UKDental caries, BEWE, BPE,Olympic athletes(n = 278); tier 4 and 5Shortened global evaluation of impact of oral health on quality of life^61^High levels of oral disease were observed, with dental caries affecting 55% of the athletes, dental erosion in 45%, gingivitis in 76%, and periodontitis in 15%More than 40% of athletes presenting to the clinic were bothered by their oral health with 28% reporting an impact on their quality of life and 18 % reporting an impact on training or performanceBEWE, Basic Erosive Wear Examination; BPE, basic periodontal examination; DMFT, Decayed, Missing, and Filled Teeth Index; ICDAS: International Caries Detection and Assessment System; OHIP-14, Oral Health Impact Profile-14; OHQoL, oral health-related quality of life; OIDP, oral impacts on daily performance; PUFA,:pulp, ulceration, fistula, abscess.Participant classification framework (tiers): tier 1 recreational; tier 2 trained/developmental; tier 3 highly trained, national level; tier 4 elite/international level; tier 5 world class^2^
What are the potential explanatory mechanisms?
Inflammatory pathways may impact recovery and reduce performance
Periodontitis is a chronic, multifactorial inflammatory disease associated with dysbiotic plaque biofilms, characterised by progressive destruction of the tooth-supporting apparatus.^64^ Due to the chronic inflammation, patients with severe periodontitis show increased markers of systemic inflammation, including high serum levels of C-reactive protein (CRP), tumour necrosis factor-alpha (TNF-α), moderate leukocytosis and high level of cytokines such as interleukin-6 (IL-6), IL-8 and IL-1 in comparison to healthy populations.^65^^,^^66^^,^^67^
Such raised systemic inflammation impairs glycaemic control. Conversely, reducing periodontal inflammation by standard, non-surgical periodontal therapy, lowers biomarkers of systemic inflammation and improves glycaemic control.^68^ Elevated cytokines (e.g., IL-6,^69^ TNF-α,^70^ CRP^71^) from oral infections may impair muscle physiology and repair,^72^ increase muscle fatigue,^73^ increase mild cognitive impairment,^74^ and affect endurance capacity.^75^ IL-6 is also known as an important signalling molecule during exercise, being released from working muscle fibres with increased exercise duration, intensity, and muscle glycogen depletion.^76^ Chronically elevated IL-6 levels were found to increase skeletal muscle fatigability and disrupt mitochondrial content and function independent of changes in fibre type and mass.^69^ Therefore, periodontitis can result in a prolonged recovery, leading to decreased performance.
Oral microbiome
The complexities of microbiome analysis are starting to be reported in relation to athlete performance. In relation to the gut, Veillonella genus has been associated with enhanced performance via lactate metabolism.^77^^,^^78^ In the mouth, limited data suggest differences in the oral microbiome between athlete and non-athlete populations; although, whether this is cause or effect is unknown.^79^ In relation to performance, attention has focused on influencing the presence of dietary nitrate-reducing bacterial species (for instance with probiotics), which can increase the efficiency of oxygen delivery and utilisation in muscle; although, the benefit is greatest in sub-elite athletes.^80^ Outside of sport, much attention has been given to the relationship between the oral microbiome and cognitive performance. Oral microbiomes associated with oral diseases such as periodontitis are associated with cognitive impairment.^81^^,^^82^^,^^83^ It is unclear if the effects of the oral microbiome on cognitive function are direct and/or mediated through inflammatory pathways. Since there are a number of distinct oral microbiomes (for instance, salivary, tongue, gingival crevice and periodontal pocket), it is important that these are fully described in studies.
Impaired nutrition
Optimising nutrition is a key strategy to improve recovery and performance.^84^^,^^85^ Poor oral health can negatively impact nutrition, for example, mediated by pain or discomfort while eating.^86^ Dental caries, periodontitis or ulcers can lead athletes to avoid certain foods (nuts, raw vegetables, or fruits with acidity) or choose highly processed food with reduced nutritional content. This can promote an imbalanced diet with reduced recovery capacities.^87^
Psychological factors
Self-confidence is important for optimal sports performance but may be reduced with noticeable dental issues (bleeding gums, missing teeth, bad breath).^88^ Furthermore, it has been shown that anxiety, depression, and attention deficit hyperactivity disorder may result in poor oral hygiene that could aggravate oral health and further reduce performance.^89^ In addition, chronic pain, for example, due to caries or periodontitis, can increase anxiety or reduce mood and decision-making capacity.^90^
Sensorimotor system
The sensorimotor system integrates afferent information from different sensors from the whole body and is involved in the execution of movements. Pain is a strong input into our sensory system and dental pain may influence sensorimotor control and may influence power in consideration of the role of periodontal mechanoreceptors.^91^ Furthermore, jaw mechanics and temporomandibular disorders have been shown to affect postural stability and performance.^92^^,^^93^ The discussed potential mechanisms are depicted in Figure 1.Fig. 1 Potential mechanisms linking oral health to sports performance
Current research gaps and future directions
Future research in sports dentistry should embrace an interdisciplinary approach, integrating expertise from dentistry, sports medicine, exercise science, and public health. This collaboration is essential to better understand and address the complex interactions between oral health and sports performance. Currently, many aspects of these relationships remain unclear, highlighting the need for more high-quality research to advance the field. To achieve this, studies must employ validated and reliable outcome measures that capture both sport-specific performance indicators and comprehensive oral health status. A clear and consistent definition of the athletic population under investigation, considering factors such as sport type, competitive level, and training load, is critical for comparability and relevance. Furthermore, co-producing research with athletes, coaches, and members of athlete medical and performance support teams will help ensure that study designs and outcomes reflect real-world needs and enhance the practical impact of findings.
Conclusion
Future efforts should focus on increasing awareness of oral health as a key component of overall athlete health, wellbeing and performance. This includes oral health screening protocols in athletes and exploring effective prevention strategies and embedding oral health education within broader athlete health promotion initiatives. Together, these directions can foster a more integrated, evidence-based approach to oral care in sports settings and may consequently further improve sports performance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1T M, O'Donoghue P, de Eira Sampaio A J. Routledge Handbook of Sports Performance Analysis. London: Routledge, 2013.
- 2Mc Kay A K A, Stellingwerff T, Smith E S et al. Defining training and performance caliber: a participant classification framework. Int J Sports Physiol Perform 2022; 17: 317–331.10.1123/ijspp.2021-045134965513 · doi ↗ · pubmed ↗
- 3Edouard P, Iatropoulos S, Velebova K et al. National medical teams during European Athletics championships from 2009 to 2024: composition, gender distribution, and influence on team performance. Sports Med Open 2025; DOI:10.1186/s 40798-025-00864-3.10.1186/s 40798-025-00864-3PMC 1208179940372657 · doi ↗ · pubmed ↗
- 4Burns A, Collins D. Interdisciplinary practice in performance sport: A scoping review of evidence of collaboration. Eur J Sport Sci 2023; 23: 1877–1891.10.1080/17461391.2023.220181237042174 · doi ↗ · pubmed ↗
- 5U M. What does a sports dentist do all day. Br Dent J 2025; 240; 04: 263-27010.1038/s 41415-025-9117-141760763 · doi ↗ · pubmed ↗
- 6Gallagher J, Ashley P, Needleman I. Oral health screening for sport. Br Dent J 2025; 240; 04: 223-22710.1038/s 41415-025-9005-8PMC 1294867241760757 · doi ↗ · pubmed ↗
- 7Gallagher J, Ashley P, Needleman I. Implementation of a behavioural change intervention to enhance oral health behaviours in elite athletes: a feasibility study. BMJ Open Sport Exerc Med 2020; DOI: 10.1136/bmjsem-2020-000759.10.1136/bmjsem-2020-000759 PMC 730479532577302 · doi ↗ · pubmed ↗
- 8Hughes D C, Ellefsen S, Baar K. Adaptations to endurance and strength training. Cold Spring Harb Perspect Med 2018; DOI: 10.1101/cshperspect.a 029769.10.1101/cshperspect.a 029769 PMC 598315728490537 · doi ↗ · pubmed ↗