Non-dilation endoscopic ultrasound-guided hepaticoduodenostomy and hepaticogastrostomy using a 7-Fr delivery system
Hidenobu Hara, Yoko Henta, Risa Katsumata, Hiroaki Matsumoto, Shiori Ito, Kouhei Yoshino, Shinya Sakita

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
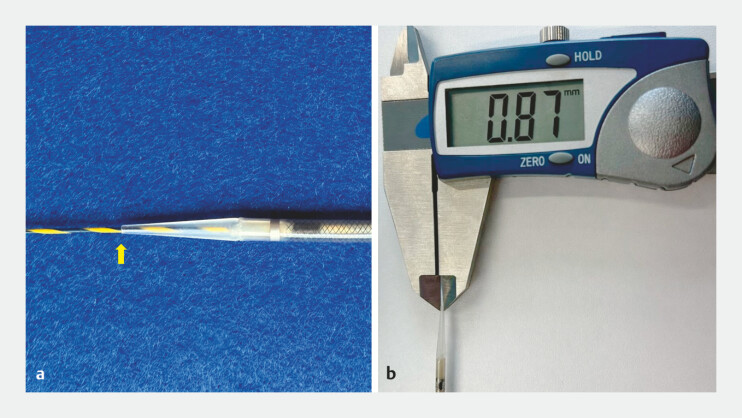 Fig. 1
Fig. 1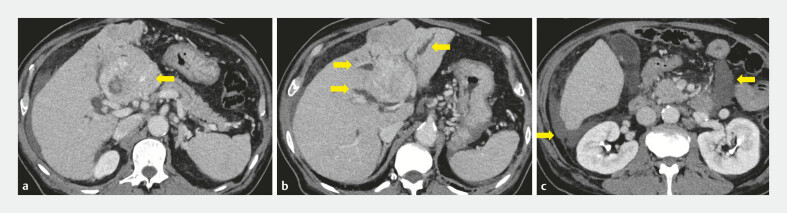 Fig. 2
Fig. 2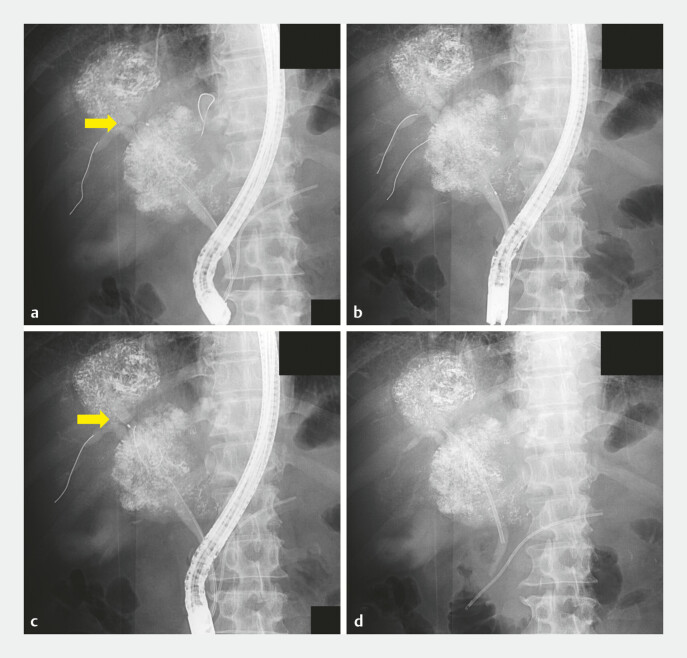 Fig. 3
Fig. 3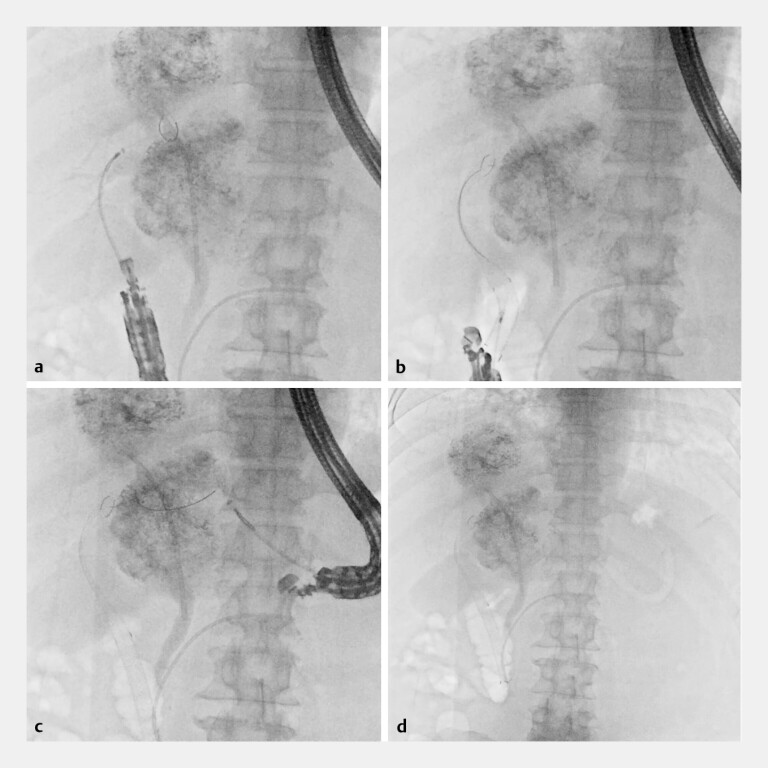 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Hepatocellular Carcinoma Treatment and Prognosis · Organ Transplantation Techniques and Outcomes
Transpapillary drainage may be inadequate for malignant hilar biliary obstruction with extensively separated ducts, and endoscopic ultrasound guided biliary drainage (EUS-BD) has been reported as salvage therapy 1 2 3 . 7-Fr slim-delivery self-expandable metal stents (SEMSs) have enabled non-dilation EUS-BD ( 4 5 ; Fig. 1 ). We report jaundice relief using non-dilation EUS-guided hepaticoduodenostomy and hepaticogastrostomy (EUS-HDGS) with a 7-Fr delivery partially covered SEMS system for hepatocellular carcinoma–related hilar obstruction.
7-Fr delivery partially covered slim-delivery self-expandable metal stents used in the procedure. a A 0.025-inch guidewire and the 7-Fr delivery catheter (arrow). b The ultra-tapered distal tip measures 0.87 mm (approximately 2.6 Fr).
A 68-year-old man with hepatitis C-related cirrhosis (Child-Pugh score, 11) and moderate ascites exhibited malignant hilar obstruction with separated ducts due to hepatocellular carcinoma. Because the tumor ruptured, emergency transarterial embolization was prioritized ( Fig. 2 ). Endoscopic retrograde cholangiopancreatography was attempted, and although guidewire access was achieved, device advancement, including a catheter, was impossible due to severe stenosis and marked ductal deviation. Therefore, an internal plastic stent (7 Fr, 9 cm) was placed only in the anterior sectoral duct ( Fig. 3 ). However, additional biliary drainage was required due to persistent jaundice, and EUS-HDGS was planned ( Video 1 ).
Pre-procedural contrast-enhanced computed tomography. a Intratumoral hemorrhage in hepatocellular carcinoma (arrow). b Malignant hilar biliary obstruction with separate intrahepatic ducts (arrow). c Moderate ascites due to cirrhosis (arrow).
Fluoroscopic images during endoscopic retrograde cholangiopancreatography. a Guidewires were advanced into B3 and B5; catheter advancement toward B3 was impeded by sharp angulation (arrow). b The guidewires were advanced into B5 and B6. c Catheter advancement into B6 was not possible (arrow). d An internal plastic stent was placed in the anterior sectoral duct, and the procedure was completed.
EUS-guided hepaticoduodenostomy and hepaticogastrostomy for hilar obstruction with separated ducts. EUS, endoscopic ultrasound.Video 1
From the duodenal bulb, B6 was punctured using a 19-gauge FNA needle, and a 0.025-inch guidewire was advanced into the intrahepatic duct. After bile aspiration and cholangiography, a partially covered SEMS (8 mm × 12 cm) with a 7-Fr delivery system was deployed without tract dilation ( Fig. 4 a, b ). B3 was similarly accessed from the stomach. A second partially covered SEMS (8 mm × 12 cm) was placed without tract dilation ( Fig. 4 c, d ). Postprocedural computed tomography confirmed appropriate stent positions. No adverse events occurred, and total bilirubin levels decreased by >50% by day 6.
Fluoroscopic images during endoscopic ultrasound-guided hepaticoduodenostomy and hepaticogastrostomy. a A 7-Fr delivery catheter was advanced from the duodenal bulb into B6 without tract dilation. b A partially covered SEMS (8 mm × 12 cm) was deployed from B6 to the duodenal bulb. c A 7-Fr delivery catheter was advanced from the stomach into B3 without dilation. d Partially covered SEMSs (8 mm × 12 cm) were deployed from B3 to the stomach. SEMS, self-expandable metal stent.
In patients with advanced cirrhosis and ascites, minimizing tract manipulation is desirable due to concerns regarding bleeding and bile leakage. A 7-Fr delivery system may facilitate non-dilation and multiroute EUS-BD for malignant hilar obstructions with separated ducts.
Endoscopy_UCTN_Code_TTT_1AS_2A
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hijioka S Nagashio Y Maruki Y Novel approach to bilateral biliary drainage: EUS-guided hepaticoduodenodenostomy plus hepaticogastrostomy in malignant hilar biliary obstruction Endosc Int Open 202513 a 2565820610.1055/a-2565-8206 PMC 1204304640309061 · doi ↗ · pubmed ↗
- 2Kuraoka N Hashimoto S Matsui S Outcomes of endoscopic ultrasound-guided biliary drainage in a general hospital for patients with endoscopic retrograde cholangiopancreatography-difficult transpapillary biliary drainage J Clin Med 2021104105411534575216 10.3390/jcm 10184105 PMC 8471391 · doi ↗ · pubmed ↗
- 3Hara H Hijioka S Nagashio YA novel method of bilateral biliary decompression by EUS-guided hepaticogastrostomy with bridging stenting using the partial stent-in-stent method for reintervention of multiple metal stent failure Video GIE 2024928628938887729 10.1016/j.vgie.2024.02.015PMC 11180363 · doi ↗ · pubmed ↗
- 4Oishi R Miwa H Endo K Endoscopic ultrasound-guided hepaticogastrostomy without tract dilation using a novel ultra-tapered slim-delivery metallic stent Endoscopy 202557 E 244E 24540112866 10.1055/a-2552-0373 PMC 11925640 · doi ↗ · pubmed ↗
- 5Miwa H Ishino Y Endo K Endoscopic ultrasonography-guided hepaticoduodenostomy using a novel self-expandable metallic stent with an ultra-tapered tip and a slim-delivery system Endoscopy 202557 E 437E 43840389252 10.1055/a-2590-8508 PMC 12088868 · doi ↗ · pubmed ↗