Biliary network linkage using a side-hole-modified metal stent for concurrent endoscopic ultrasound-guided hepaticoduodenostomy
Hiroki Koda, Kazuo Hara, Tomoki Ogata, Shin Haba, Takamichi Kuwahara, Nozomi Okuno, Shimpei Matsumoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
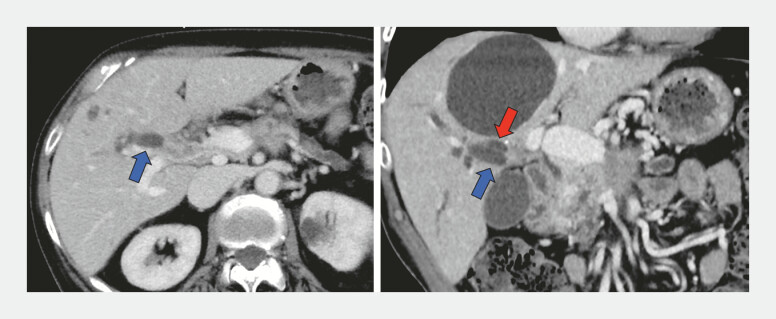 Fig. 1
Fig. 1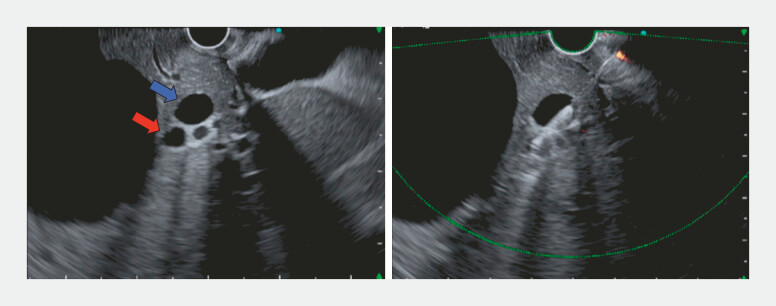 Fig. 2
Fig. 2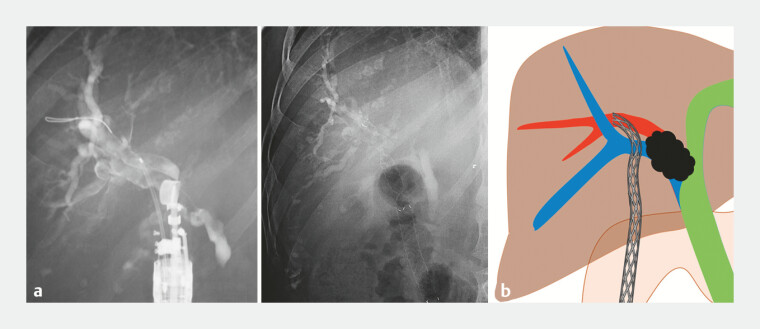 Fig. 3
Fig. 3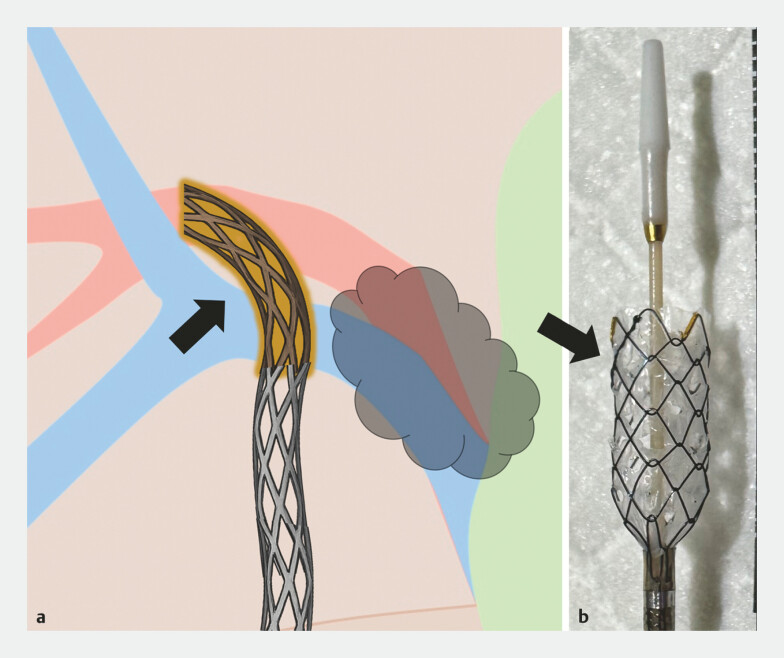 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Pancreatic and Hepatic Oncology Research
Endoscopic ultrasound (EUS)-guided stent bridging and related techniques enable the traversal of separated intrahepatic ducts in complex malignant hilar obstruction 1 2 3 . We refer to the intentional creation of a functional communication between anatomically separated ducts as EUS-guided biliary network linkage (EUS-BNL), a conceptual framework emphasizing the reconstruction of an internal drainage pathway. Side holes manually created on a fully covered self-expandable metal stent (FCSEMS) may help prevent occlusion of intrahepatic side branches during drainage 4 . In this case, such a modified FCSEMS enabled both BNL and EUS-guided hepaticoduodenostomy (EUS-HDS) to be achieved with the same single removable stent, facilitating reintervention ( Video 1 ).
An EUS-guided approach using a side-hole-modified fully covered metal stent to achieve EUS-guided biliary network linkage (EUS-BNL) and hepaticoduodenostomy with the same single stent, enabling multisegmental drainage in complex hilar obstruction. EUS, endoscopic ultrasound.Video 1
A 76-year-old woman presented with malignant hilar obstruction caused by peritoneal dissemination of pancreatic cancer, resulting in the complete separation of the right anterior and posterior ducts ( Fig. 1 ). Because further anatomic complexity was expected, EUS-HDS was selected as the primary drainage route. From the duodenal bulb, convex EUS (EG740UT; FUJIFILM) demonstrated both ducts aligned along the intended access path, enabling sequential traversal. A 19-gauge needle (EZ Shot 3 Plus; Olympus) was advanced through hepatic parenchyma to skewer both ducts ( Fig. 2 ). After cholangiography confirmed positioning, a guidewire was inserted into B7, and the tract was dilated using a drill dilator.
Computed tomography demonstrates the complete separation of the right anterior (blue arrow) and posterior (red arrow) segmental bile ducts caused by peritoneal dissemination from pancreatic cancer infiltrating the hepatic hilum.
The anterior (blue arrow) and posterior (red arrow) segmental bile ducts were skewered under EUS guidance to obtain sequential access for endoscopic ultrasound-guided biliary network linkage (EUS-BNL).
A single FCSEMS (HANAROSTENT Biliary Benefit, 8 mm × 12 cm) was deployed from the posterior duct into the duodenum, establishing interductal linkage consistent with the EUS-BNL concept ( Fig. 3 ). The side-hole-modified distal segment was positioned to overlap the anterior duct, providing drainage while the same stent concurrently served as the HDS stent ( Fig. 4 ). Because the stent is fully covered and removable, reintervention can be performed as needed.
A single metal stent placed via biliary skewering establishes interductal linkage consistent with the EUS-BNL concept and simultaneously serves as the hepaticoduodenostomy stent. a A fluoroscopic image. b Schematic illustration. EUS-BNL, endoscopic ultrasound-guided biliary network linkage.
The blurred segment (arrow) represents manually created side holes in the stent mesh, enabling the effective drainage of the anterior duct while using the same stent for concurrent EUS-HDS. a Schematic illustration. b An image showing the portion of the stent where multiple side holes were created. EUS-HDS, endoscopic ultrasound-guided hepaticoduodenostomy.
This case demonstrates that EUS-BNL offers an effective strategy for multisegmental drainage and that side-hole modification enables concurrent EUS-HDS with the same single stent in complex hilar obstruction.
Endoscopy_UCTN_Code_TTT_1AR_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ogura T Sano T Onda S Endoscopic ultrasound-guided biliary drainage for right hepatic bile duct obstruction: novel technical tips Endoscopy 201547727510.1055/s-0034-137811125264761 · doi ↗ · pubmed ↗
- 2Takeshita K Hijioka S Nagashio Y Comparison of stent patency between EUS-guided hepaticogastrostomy with bridging and endoscopic transpapillary biliary drainage for hilar obstruction Endosc Int Open 202412 E 875E 88638989254 10.1055/a-2333-7898 PMC 11236478 · doi ↗ · pubmed ↗
- 3Koda H Hara K Okuno NA novel technique of B 2-B 3 single-puncture bridging through liver parenchyma enabling endoscopic ultrasound-guided hepaticogastrostomy for rescue drainage Endoscopy 202557 E 936E 93740834896 10.1055/a-2663-8418 PMC 12367398 · doi ↗ · pubmed ↗
- 4Kuwabara R Hara K Haba S Multiple Self-Made Side Holes in a Fully Covered Metal Stent Prevent Intrahepatic Bile Duct Occlusion Following Endoscopic Ultrasound-Guided Hepaticogastrostomy: A Retrospective Study in Japan J Clin Med 202514377310.3390/jcm 1411377340507535 PMC 12156069 · doi ↗ · pubmed ↗