Autoimmune gastritis masquerading as subepithelial squamous infiltration: a case report
Han Wang, Ziyuan Yu, Zhenyu Chen, Xudan Yang, Xiaogang Liu, Xiao Hu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
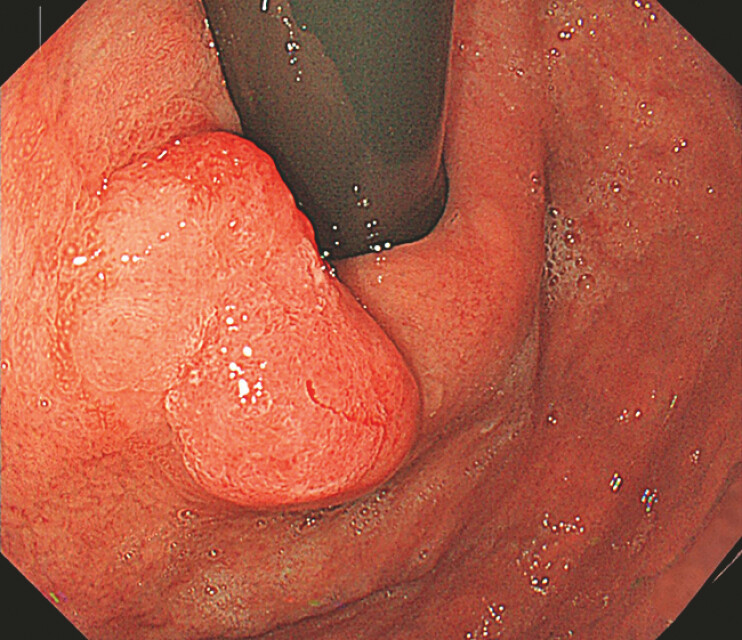 Fig. 1
Fig. 1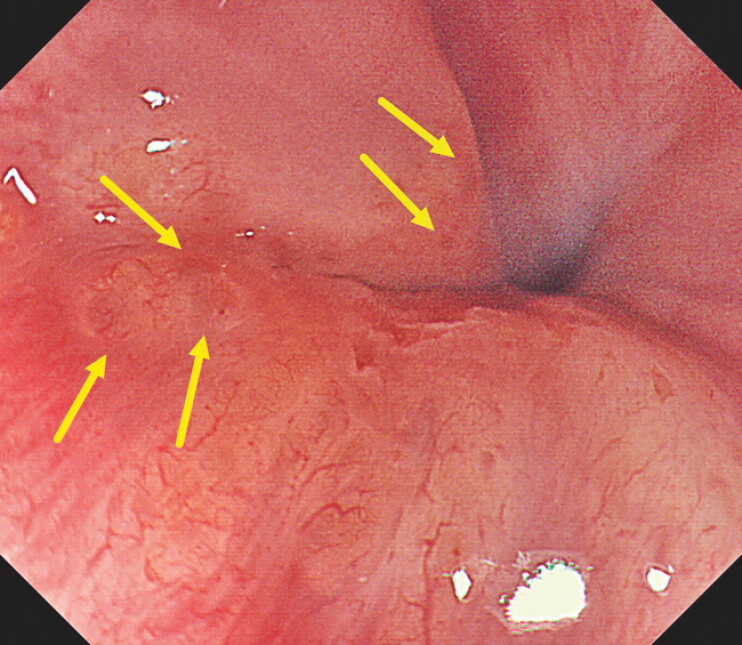 Fig. 2
Fig. 2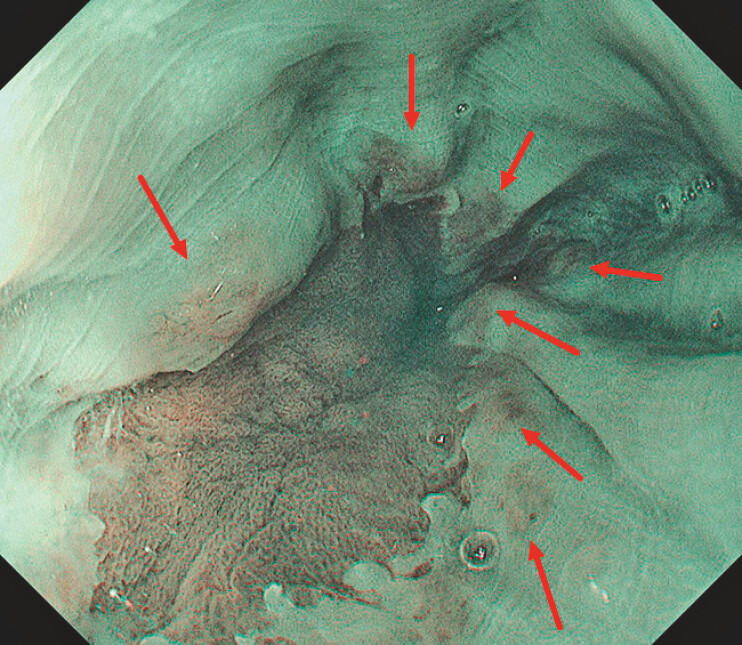 Fig. 3
Fig. 3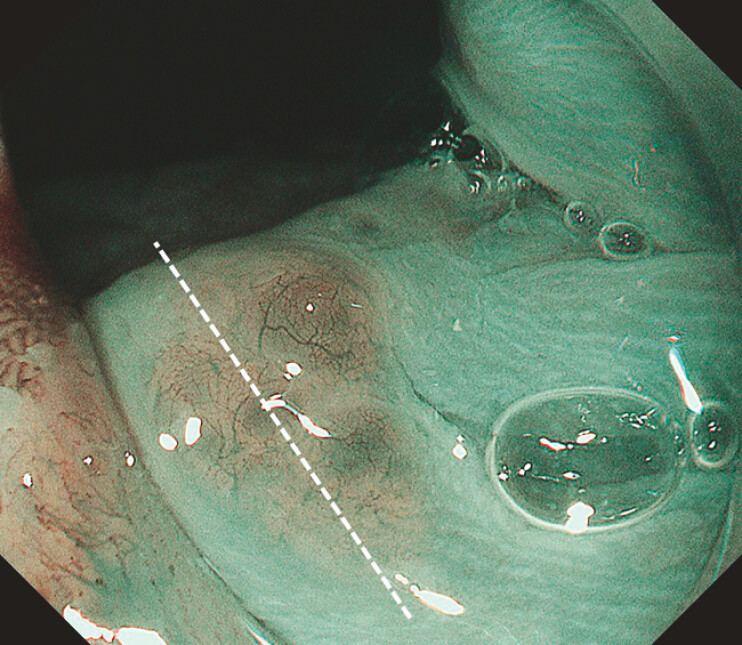 Fig. 4
Fig. 4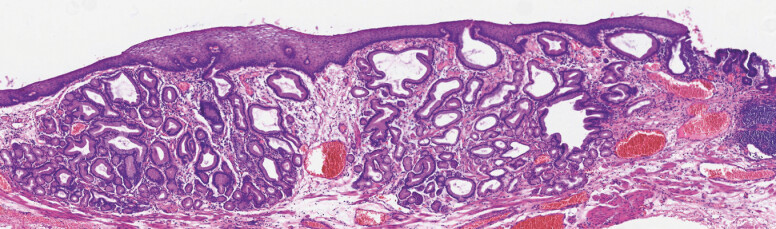 Fig. 5
Fig. 5- —Sichuan Science and Technology Program, The Natural Science Foundation of Sichuan Province (Youth Fund Project)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMicroscopic Colitis · Helicobacter pylori-related gastroenterology studies · Vasculitis and related conditions
Autoimmune gastritis (AIG) is a chronic immune-mediated disorder with parietal cell destruction, causing hypochlorhydria, hypergastrinemia and the risk of gastric neoplasia 1 2 . Multiple endoscopic signs (corpus-predominant atrophy, sticky mucus and the cast-off skin appearance [CSA]) have been described; yet, a specific endoscopic marker remains unestablished 3 4 .
We present the case of a 70-year-old man with prior Helicobacter pylori ( H. pylori ) eradication. The gastric mucosa exhibits corpus-predominant atrophic gastritis, with a visible vascular pattern, flattened folds in the body and fundus and CSA in the body. Serology confirmed autoimmune gastritis (anti-parietal cell antibody (APCA): 82.97 U/mL, anti-intrinsic factor antibody (AIFA): 6.9 IU/mL, gastrin: 189 pg/mL, pepsinogen I/II: 0.4, and vitamin B12 <83 pg/mL). A type 0-IIa lesion (suspected dysplastic lesion) was observed on the greater curvature of the gastric cardia ( Fig. 1 ). Above the squamocolumnar junction (Z-line), circumferential yellowish granular elevations were observed, with some translucent “bubble-like” appearances on the white light image (WLI; Fig. 2 ), thinning of the squamous epithelium and brownish color on NBI ( Fig. 3 ), and fine reticular microvessels on ME-NBI ( Fig. 4 ). These were initially interpreted as subepithelial squamous infiltration of tumor. Endoscopic submucosal dissection en bloc resection yielded a 3.2 cm × 1.5 cm well-differentiated tubular/papillary adenocarcinoma (tub2>tub1> pap, intestinal phenotype, pT1b). However, the pathology of granulations above the Z-line showed markedly hyperplastic and dilated esophageal cardia glands in lamina propria ( Fig. 5 ), expressing MUC6 and MUC5AC ( Video 1 ).
A type 0-IIa lesion at the cardia, measuring approximately 1.5 cm × 3.0 cm, which pathologically confirmed as well-differentiated tubular/papillary adenocarcinoma.
Yellowish granular elevations at the gastroesophageal junction (GEJ) and the translucent “bubble-like” appearance on the white light image (WLI) (indicated by yellow arrows).
Yellowish granular elevations appear brownish on NBI (indicated by red arrows).
ME-NBI shows the fine reticular vascular structure and the translucent “bubble-like” appearance.
Slide of the white dashed line in Fig. 4 , HE × 20, showing focal thinning of the squamous epithelium and glandular structures in the lamina propria of the esophageal mucosa.
Autoimmune gastritis masquerading as subepithelial squamous infiltration.Video 1
To validate this finding, we retrospectively analyzed endoscopic records from 20 AIG cases (sequential AIG cases at our institution from May 1 to Nov 30, 2025, with positive APCA/AIFA and histological confirmation) and 20 non-AIG cases (randomly selected from age- and sex-matched patients undergoing gastroscopy in the same period with negative APCA/AIFA). The manifestation was observed in all 20 AIG cases (100%) but absent in controls ( P <0.001, Fisherʼs exact test; Video 1 ). This unreported manifestation may be represented as a suggestive endoscopic marker of AIG. While this finding was strongly associated with AIG in our study cohort, we acknowledge that the cardia gland hyperplasia might represent a consequence of hypochlorhydria rather than AIG itself, and further prospective studies are needed to validate its specificity.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Waldum HL Fossmark R Role of autoimmune gastritis in gastric cancer [J]Clin Transl Gastroenterol 201910 e 0008010.14309/ctg.000000000000008031517647 PMC 6775339 · doi ↗ · pubmed ↗
- 2Lenti MV Rugge M Lahner E Autoimmune gastritis Nat Rev Dis Primers 202065610.1038/s 41572-020-0187-832647173 · doi ↗ · pubmed ↗
- 3Song M Latorre G Ivanovic-Zuvic D Autoimmune diseases and gastric cancer risk: a systematic review and Meta-Analysis Cancer Res Treat 20195184185010.4143/crt.2019.15131048663 PMC 6639229 · doi ↗ · pubmed ↗
- 4Kamada T Watanabe H Furuta T Diagnostic criteria and endoscopic and histological findings of autoimmune gastritis in Japan J Gastroenterol 20235818519510.1007/s 00535-022-01954-936855000 PMC 9998601 · doi ↗ · pubmed ↗