Robotic-assisted esophageal endoscopic submucosal dissection in a compact and extensive early Barrett’s cancer lesion
Giorgi Tvaradze, Mayo Tanabe, Kazuki Yamamoto, Stefan Groth, Ewerton Marques Maggio, Haruhiro Inoue, Stefan Seewald

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
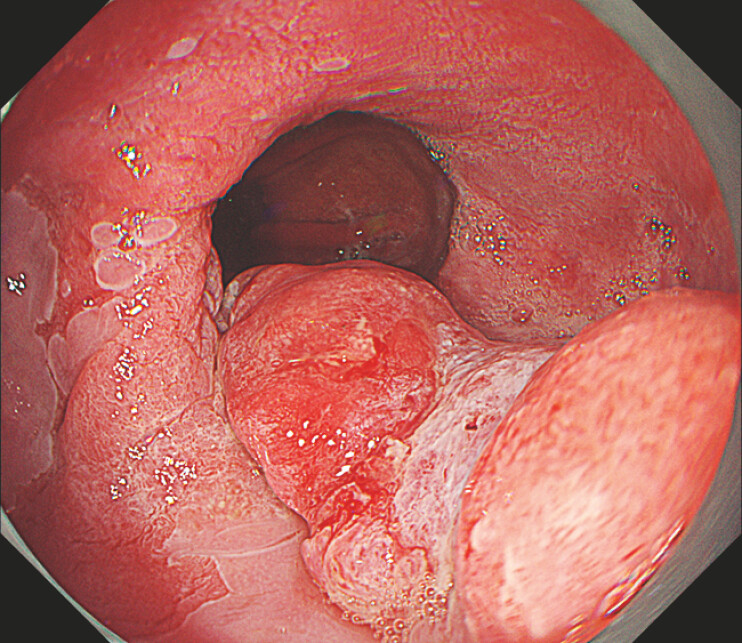 Fig. 1
Fig. 1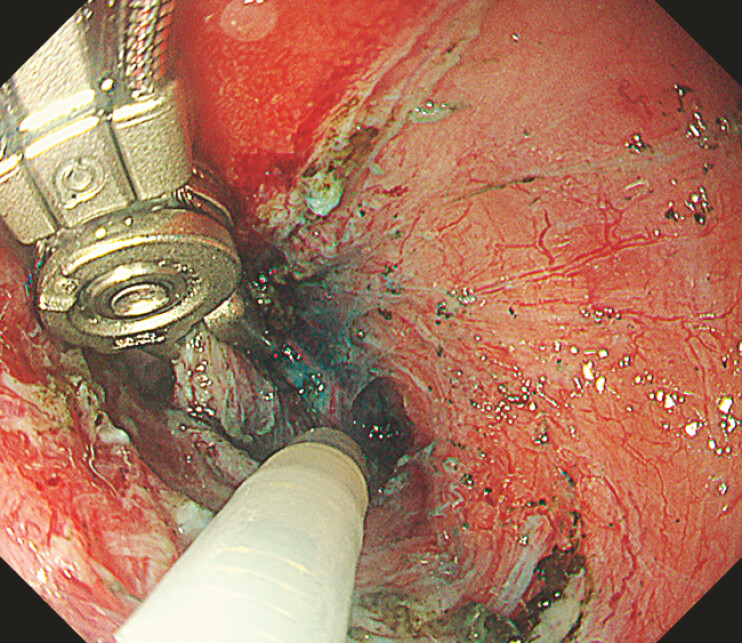 Fig. 2
Fig. 2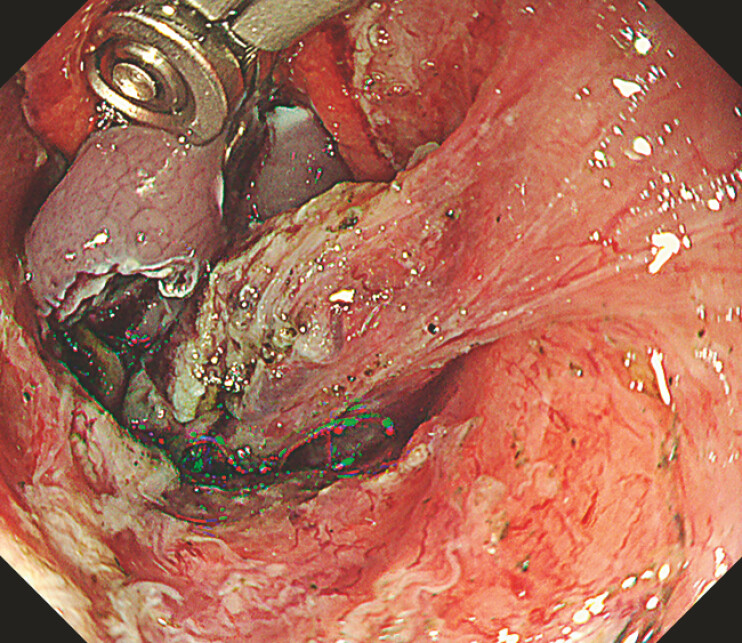 Fig. 3
Fig. 3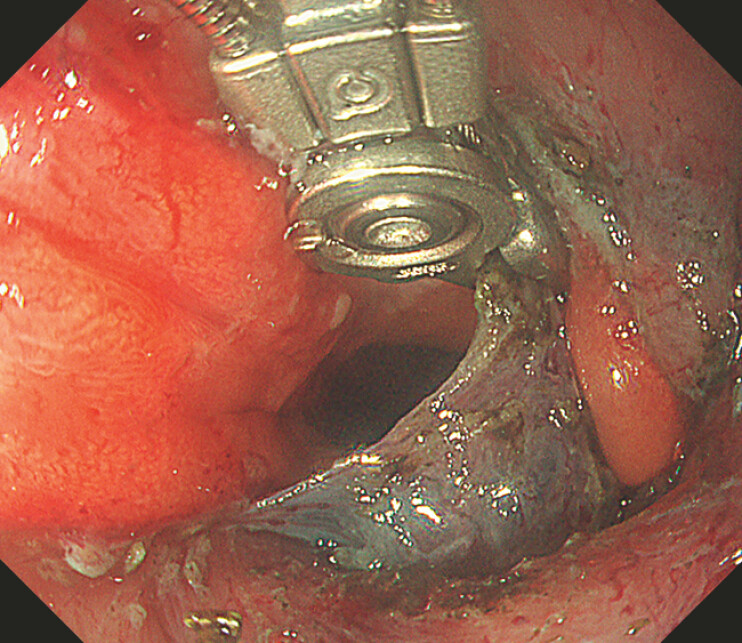 Fig. 4
Fig. 4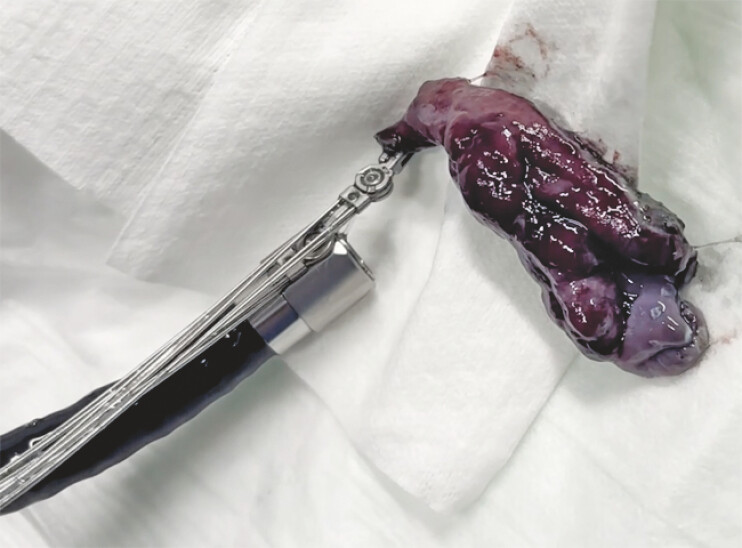 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes · Metastasis and carcinoma case studies
Endoscopic submucosal dissection (ESD) of large and compact esophageal lesions is technically demanding, especially in the later stages of the procedure 1 2 . The partially dissected specimen often becomes floppy and obscures the dissection field. This loss of visualization and traction limitation makes dissection challenging. Conventional traction methods provide only limited axis movements and cannot be easily repositioned 3 4 .
A novel EndoRobotics Alligator (ROBOPERA & TraCloser) device is designed for flexible multipoint traction. The device provides true four-axis independent movements, enabling multidirectional traction 5 . The operator can lift, rotate, pull, or push the lesion in multiple directions and reposition at any time, maintaining continuous exposure of the submucosal layer and preventing the partially dissected specimen from obstructing the field. This multidirectional control improves visualization, optimizes tissue tension and facilitates dissection ( Video 1 ).
We report the first case of an EndoRobotics Alligator-assisted esophageal ESD of an 11 cm early Barrett’s adenocarcinoma extending over 70% of the circumference, with a 5 cm compact component ( Fig. 1 ). The use of this novel device was authorized by the Institutional Review Board. After circumferential incision and completing dissection of 70% of the lesion, visualization and access to the dissection plane worsened. The alligator device was used at this later stage of the procedure ( Fig. 2 ) to lift the compact specimen in order to revisualize the dissection plane, maintain tension, and finalize the dissection ( Fig. 3 and Fig. 4 ). The lesion was successfully resected en bloc ( Fig. 5 ). R0 resection was histologically confirmed, and no intra- or post-procedural adverse events occurred.
An 11 cm Barrett’s adenocarcinoma lesion with a 5 cm compact component (0-Is + IIb Paris classification) and signs of deep submucosal invasion.
The alligator device grasping the partially resected lesion, which is currently obscuring the dissection plane.
After three-axis movements (grip, wrist, and arm movements), the lesion is lifted, the submucosa is exposed, and clear visualization of the submucosal dissection plane with adequate working space is achieved.
Repositioning of the alligator device with the application of the rotational movement (fourth axis movement) enables the visualization of the non-resected submucosal layer and allows safe continuation of the dissection.
Retrieval of the resected specimen using the alligator device.
Alligator-assisted esophageal endoscopic submucosal dissection in a compact and extensive early Barrett’s cancer lesion provides multidirectional tissue movement, enabling the excellent visualization of the dissection plane and robust, flexible, repositionable traction.Video 1
Alligator-assisted robotic traction is a valuable tool during esophageal ESD, particularly in challenging cases involving compact lesions. By providing dynamic multidirectional traction, it complements conventional ESD techniques and enhances visualization, stability, and dissection efficiency. This case demonstrates that integrating robotic traction into ESD enables a safer and more controlled tissue handling.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD Endoscopy_UCTN_Code_CCL_1AB_2AC_3AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Oyama T Tomori A Hotta K Endoscopic submucosal dissection of early esophageal cancer Endoscopy 20053711111410.1016/s 1542-3565(05)00291-016013002 · doi ↗ · pubmed ↗
- 2Jeon HJ Keum B Lee BA novel robotic arm–assisted endoscopic submucosal dissection platform with augmented traction for gastric neoplasms: a first-in-human prospective pilot study (with videos)Gastrointest Endosc 2025 Online ahead of print 10.1016/j.gie.2025.09.01240962233 · doi ↗ · pubmed ↗
- 3Sakamoto T Matsuda T Nakajima T Effective traction methods for endoscopic submucosal dissection Endoscopy 200941845850
- 4Inoue H Ikeda H Hosoya T Endoscopic submucosal dissection for esophageal neoplasms Endoscopy 20013368769011490385
- 5Fujiyoshi Y Shimamura Y Mosko JD Endoscopic submucosal dissection using a new super-soft hood and the multipoint traction technique Video GIE 2020527427710.1016/j.vgie.2020.03.01032642609 PMC 7332761 · doi ↗ · pubmed ↗