Rechallenge With Cisplatin After an Acute Coronary Event
Zehra Jaffery, Rick L. Jobski, Richard S. Siegel, Anju Nohria

TL;DR
A young man with testicular cancer safely resumed cisplatin treatment after a heart-related complication with careful monitoring and team coordination.
Contribution
This case demonstrates that cisplatin rechallenge is feasible after an acute coronary event with multidisciplinary care.
Findings
Cisplatin-induced myocardial infarction can resolve with antiplatelet and anticoagulant therapy.
Multidisciplinary evaluation enables safe cisplatin rechallenge in select patients.
Close surveillance and optimized medical management are critical for successful rechallenge.
Abstract
Testicular cancer is the most common malignancy in young men, and cisplatin-based chemotherapy provides excellent long-term survival. However, cisplatin-associated cardiovascular toxicity spans a broad spectrum, and evidence guiding rechallenge after an acute coronary event is limited. A 24-year-old man with testicular cancer and no cardiovascular risk factors developed chest pain and elevated troponins early in his cisplatin therapy. Coronary angiography revealed a nonocclusive left anterior descending artery thrombus. After treatment with antiplatelet and anticoagulant therapy, the thrombus resolved, and he subsequently underwent a carefully monitored cisplatin rechallenge. Given cisplatin's curative benefit, a multidisciplinary team—including cardiology, oncology, and pharmacy—assessed the risks and benefits of continuing therapy. With close surveillance and optimized medical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
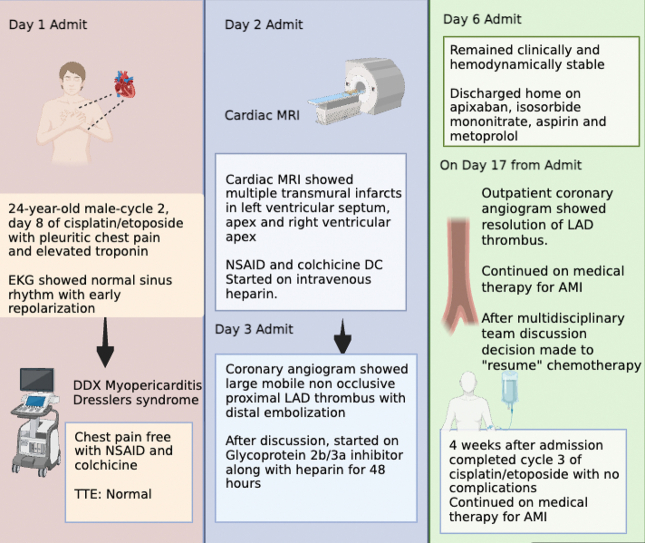 Figure 1
Figure 1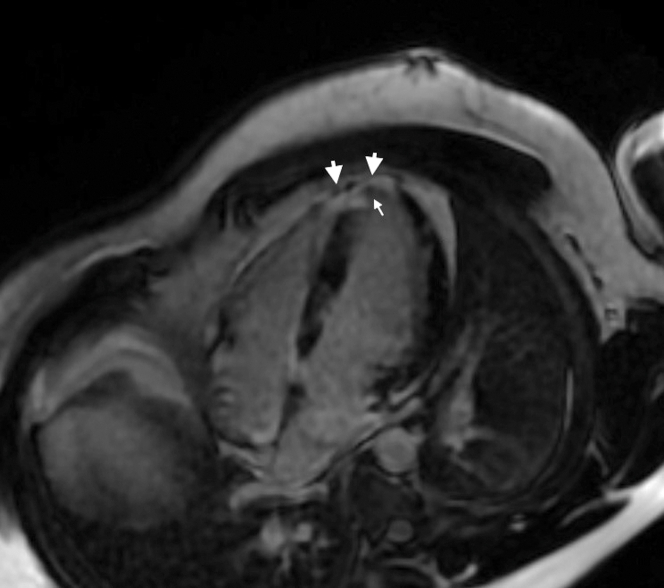 Figure 2
Figure 2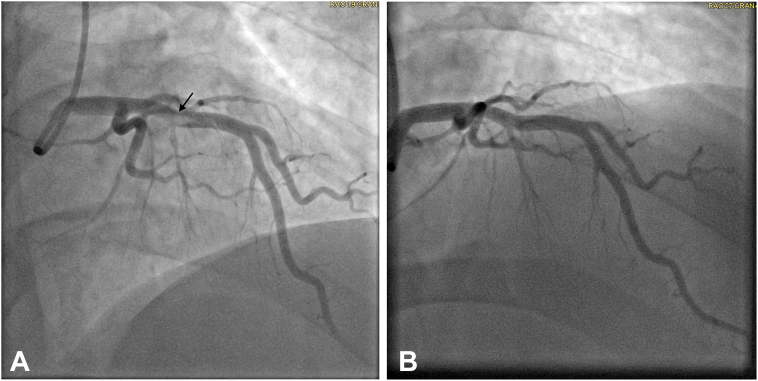 Figure 3
Figure 3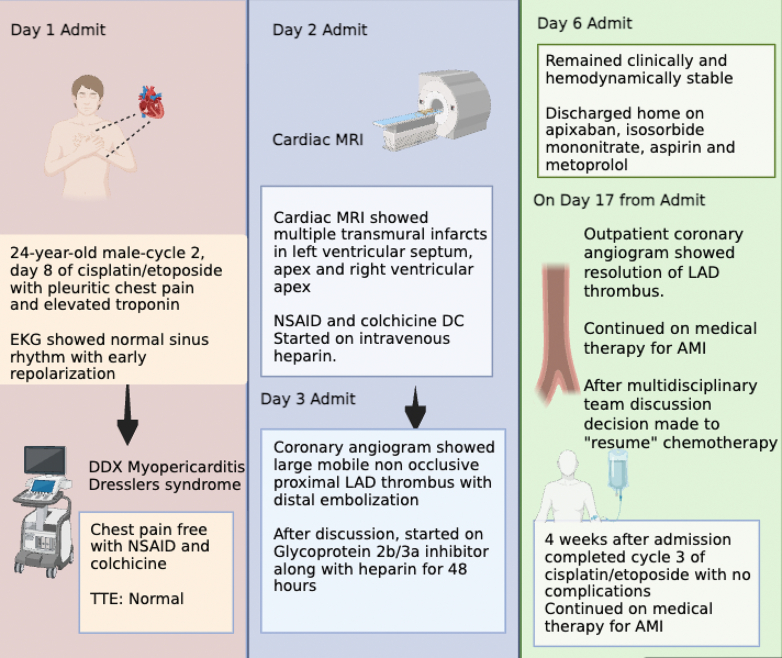 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-induced cardiotoxicity and mitigation · Chemotherapy-induced organ toxicity mitigation · Acute Myocardial Infarction Research
Visual SummaryPatient Presentation and Treatment CourseThe figure was created using BioRender. AMI = acute myocardial infarction; DC = discontinuation; DDX = differential diagnosis; EKG = electrocardiogram; LAD = left anterior descending artery; MRI = magnetic resonance imaging; NSAID = nonsteroidal anti-inflammatory drug; TTE = transthoracic echocardiogram.
History of Present Illness
A 24-year-old man with testicular cancer presented to the emergency department on day 8 of cycle 2 of cisplatin and etoposide chemotherapy with 24 hours of pleuritic chest pain. On examination, he was hemodynamically stable with an unremarkable physical examination. Electrocardiogram demonstrated normal sinus rhythm with early repolarization. High-sensitivity cardiac troponin was elevated at 8,100 ng/L, with subsequent serial measurements of 6,422, 10,481, and 9,067 ng/L.Take-Home Messages
- •Cisplatin-induced myocardial infarction requires prompt recognition and coordinated care.
- •With multidisciplinary evaluation, rechallenge can be safely performed in select patients.
Past Medical History
He was recently diagnosed with a stage IIB (T2b N1 M0) nonseminomatous germ cell tumor of the testis and had undergone left orchiectomy 2 months earlier. His planned chemotherapy regimen consisted of 4 cycles of cisplatin/etoposide because he opted to avoid bleomycin because of its potential for pulmonary toxicity. He had a body mass index of 33 kg/m^2^ and no other traditional cardiovascular risk factors.
Differential Diagnosis
In the context of pleuritic chest pain with an elevated troponin, the differential diagnosis was myopericarditis and cisplatin-induced coronary vasospasm with Dressler syndrome.
Investigations
Transthoracic echocardiography revealed normal cardiac structure and function with no pericardial effusion. As part of the diagnostic work-up, cardiac magnetic resonance was performed. Cardiac magnetic resonance demonstrated a normal left ventricular ejection fraction of 79% with a small area of apical hypokinesis. There was transmural late gadolinium enhancement involving approximately 15% of the myocardium with associated edema affecting the anteroseptum, apex, and right ventricular apex (Figure 1).Figure 1. Cardiac Magnetic ResonanceFour-chamber view showing delayed contrast enhancement in the left ventricular septum, apex, and right ventricular apex (large arrows). Small arrow displays microvascular obstruction.
Given the known association between cisplatin and arterial thrombosis, coronary angiography was performed. This revealed a large, nonocclusive, mobile thrombus in the proximal left anterior descending (LAD) artery at the level of a large septal perforator, with poor distal runoff in the distal LAD, likely due to distal embolization (Figure 2A).Figure 2. Coronary Angiograms(A) Initial coronary angiogram with a large filling defect (thrombus) in the proximal left anterior descending (LAD) artery (arrow). (B) Two-week coronary angiogram with resolution of the thrombus in the proximal LAD after medical management.
Management
On admission, he was started on colchicine and nonsteroidal anti-inflammatory drugs and was chest pain free within 12 hours. After coronary angiography and multidisciplinary discussion, thrombectomy was deferred because of the high risk of further embolization. He was started on a glycoprotein 2b/3a inhibitor along with heparin for 48 hours. Because he remained asymptomatic, a “watch and wait” approach with systemic anticoagulation and planned follow-up coronary angiography to reassess the thrombus was deemed the safest strategy. A bubble study was negative, and further work-up showed no evidence of venous thrombosis. He was discharged on hospital day 5 on metoprolol, aspirin, isosorbide mononitrate, and apixaban. A repeat coronary angiogram performed 2 weeks later demonstrated complete resolution of the thrombus with normal coronary arteries (Figure 2B).
There was discussion between the oncology and cardio-oncology teams regarding the safety of resuming cisplatin given his recent acute myocardial infarction (AMI) and his poor long-term cancer prognosis with cessation of therapy. Based on review of published case series, his young age, being symptom-free, and his stable clinical status on current medical treatment and cancer prognosis, the risk-benefit ratio was thought to favor resumption of his chemotherapy regimen with close cardiac monitoring.
Outcomes and Follow-Up
He completed cycle 3 without complications but opted to forgo cycle 4 in favor of active surveillance. Aspirin therapy was continued for 1 year in accordance with AMI guidelines. At his 6-month follow-up, he requested discontinuation of isosorbide mononitrate. At 2-year follow-up, he remains free of recurrent cardiovascular events, his tumor is in complete remission, and he remains on metoprolol and apixaban. The optimal duration of antithrombotic therapy in this context is unclear. Given the lack of evidence supporting long-term use, we plan to reassess this at his 3-year follow-up. If antithrombotic therapy is discontinued at that time, low-dose aspirin will be restarted and continued indefinitely. Metoprolol is planned for at least 3 years after his cardiac event and will also be readdressed at this next visit. His traditional cardiovascular risk factors will require closely monitoring and treatment going forward.
Discussion
We describe the case of a 24-year-old man who developed an AMI from a large, mobile LAD thrombus during cisplatin therapy for testicular cancer. The event was successfully managed medically, and he was later safely rechallenged with cisplatin without additional cardiovascular complications.
The risk of cisplatin-induced cardiovascular disease is greatest within the first year after treatment but may persist or increase years later, suggesting a biphasic pattern of risk.1 Thromboembolic complications occur in approximately 9% to 11%2 of patients immediately after cisplatin-based chemotherapy, and chest pain is reported in up to 40%.3 Coronary angiography may reveal single and even multivessel coronary thrombosis without underlying atherosclerosis.4 Experimental evidence supports plaque erosion as the leading mechanism, with cisplatin inducing endothelial damage, thromboxane production, and platelet activation and aggregation. Vasospastic angina has also been reported. This early vascular toxicity is pathologically distinct from chronic atherosclerotic disease. Notably, cisplatin levels can remain detectable in the body for years after therapy, maintaining a prolonged risk of chest pain and acute ischemic events.5
Published literature regarding continuation of cisplatin after an acute cardiovascular event is limited to conflicting case reports. Morrow et al6 described a 45-year-old with an AMI and cardiac arrest treated with primary percutaneous intervention, attributed to underlying atherosclerosis. He completed chemotherapy on standard post-myocardial Infarction (MI) therapy but experienced another AMI 10 months later due to progressive atherosclerosis and left ventricular thrombus, prompting anticoagulation. Scafa-Udriste et al7 reported a case of a 34-year-old man with an acute inferior MI and mild right coronary artery stenosis who continued cisplatin after initiation of standard secondary prevention for MI. In contrast, our patient who was younger and had no evidence of atherosclerosis, presented with a large mobile LAD thrombus and multiple infarcts, and was maintained on long-term anticoagulation to prevent recurrent events.
A “high-risk vascular fingerprint” has recently been proposed for patients with testicular cancer receiving cisplatin, defined by the presence of ≥3 of the following: body mass index ≥25 kg/m^2^, current smoking, hypertension (blood pressure >140/90 mm Hg or treated), hyperlipidemia (or treated), and elevated fasting plasma glucose.8 Our patient did not meet these high-risk criteria on admission.
The incidence of testicular cancer in young men has been rising, and although cure rates are excellent, evidence guiding cisplatin continuation after an AMI remains limited. Moreover, there are no data defining optimal cardioprotection strategies in this population. Establishing national registries to track patients who experience acute cardiovascular events during or after cisplatin treatment could provide valuable insights to inform management.
Conclusions
Cisplatin-associated cardiovascular events, although uncommon, can be life-threatening. Our patient presented with Dressler syndrome and was found to have a large, mobile LAD thrombus. Early recognition and prompt management were lifesaving, and a multidisciplinary approach enabled continuation of his chemotherapy. He remains on long-term anticoagulation and has remained free of recurrent events 2 years after his initial presentation.
Funding Support and Author Disclosures
Dr Nohria has received unrelated research support from Bristol Myers Squibb; consulting fees from AstraZeneca and Takeda Oncology; speaker fees from MLI Education; and is a paid clinical expert for Teledoc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lauritsen J.Hansen M.K.Bandak M.Cardiovascular risk factors and disease after Male germ cell cancer J Clin Oncol 386202058459210.1200/jco.19.0118031821065 · doi ↗ · pubmed ↗
- 2Soultati A.Mountzios G.Avgerinou C.Endothelial vascular toxicity from chemotherapeutic agents: preclinical evidence and clinical implications Cancer Treat Rev 385201247348310.1016/j.ctrv.2011.09.00221982720 · doi ↗ · pubmed ↗
- 3Fukuda M.Oka M.Itoh N.Vasospastic Angina likely related to cisplatin-containing chemotherapy and thoracic irradiation for lung cancer Intern Med 385199943643810.2169/internalmedicine.38.43610397083 · doi ↗ · pubmed ↗
- 4Herrmann J.Yang E.H.Iliescu C.A.Vascular toxicities of cancer therapies Circulation 1331320161272128910.1161/CIRCULATIONAHA.115.01834727022039 PMC 4817363 · doi ↗ · pubmed ↗
- 5Gietema J.A.Meinardi M.T.Messerschmidt J.Circulating plasma platinum more than 10 years after cisplatin treatment for testicular cancer Lancet 355920920001075107610.1016/S 0140-6736(00)02044-410744098 · doi ↗ · pubmed ↗
- 6Morrow A.J.Cameron A.C.Payne A.R.White J.Lang N.N.Cisplatin related cardiotoxicity – acute and chronic cardiovascular morbidity in a testicular cancer survivor Scottish Med J 6512020242710.1177/003693301989734731886736 · doi ↗ · pubmed ↗
- 7Scafa-Udriste A.Popa-Fotea N.-M.Bataila V.Calmac L.Dorobantu M.Acute inferior myocardial infarction in a young man with testicular seminoma: a case report World J Clin Cases 91620214040404510.12998/wjcc.v 9.i 16.404034141764 PMC 8180225 · doi ↗ · pubmed ↗
- 8Lubberts S.Boer H.Altena R.Vascular fingerprint and vascular damage markers associated with vascular events in testicular cancer patients during and after chemotherapy Eur J Cancer 63201618018810.1016/j.ejca.2016.05.02227322917 · doi ↗ · pubmed ↗