Catheter Ablation of His-Purkinje System–Related Ventricular Tachycardia After Left Bundle Branch Area Pacing
Yu Zhang, Weifeng Jiang, Xu Liu, Xiaofeng Hu

TL;DR
A case report shows that ventricular tachycardia can occur after a specific heart pacing procedure and requires careful diagnosis and treatment.
Contribution
This is the first reported case of His-Purkinje system-related ventricular tachycardia following left bundle branch area pacing.
Findings
HPS-VT can develop after LBBAP, requiring targeted ablation for treatment.
Accurate diagnosis is crucial to avoid conduction system injury.
Recurrence of VT may necessitate additional ablation procedures.
Abstract
Sustained His-Purkinje system–related ventricular tachycardia (HPS-VT) after left bundle branch area pacing (LBBAP) has not to our knowledge been previously reported. A 65-year-old woman presented 1 month after dual-chamber LBBAP with hypotension and recurrent palpitations. Electrocardiogram showed 2 bundle branch block–like VT morphologies; device interrogation demonstrated ventriculoatrial dissociation, consistent with HPS-VT. Intracardiac echocardiography localized the left bundle branch pacing lead to the anterior left ventricular septum. Targeted septal ablation terminated VT, but early recurrence required a second ablation, resulting in complete atrioventricular block; pacing was revised to the right ventricular septum. VT had not recurred at the 1-month follow-up. This case illustrates that HPS-VT can complicate LBBAP. Lead-related conduction system stimulation or injury may…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
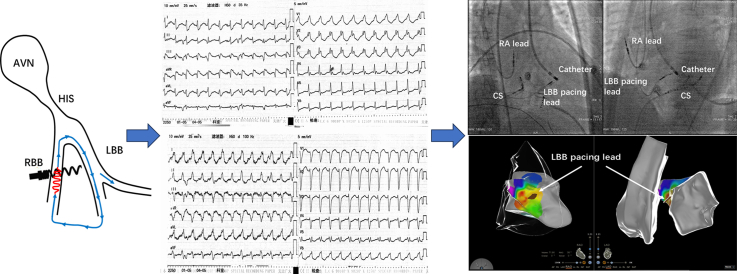 Figure 1
Figure 1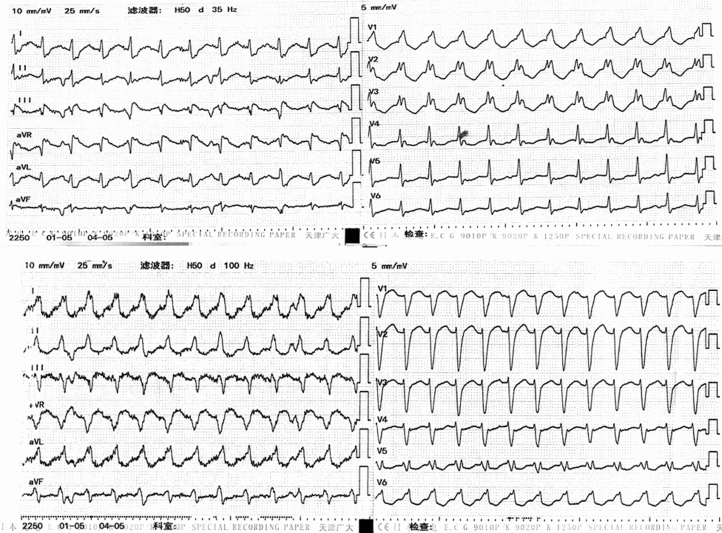 Figure 2
Figure 2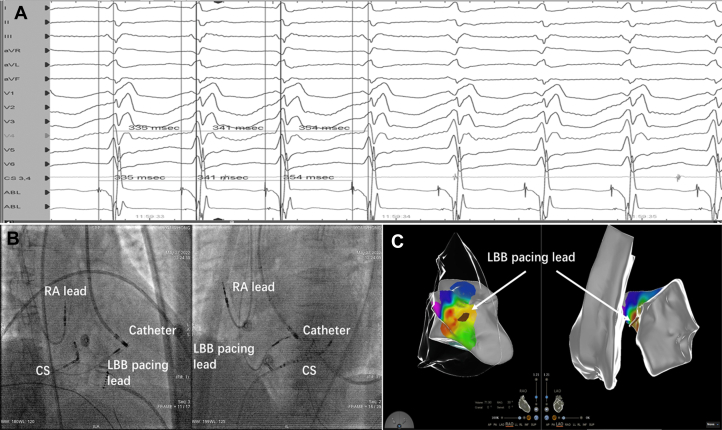 Figure 3
Figure 3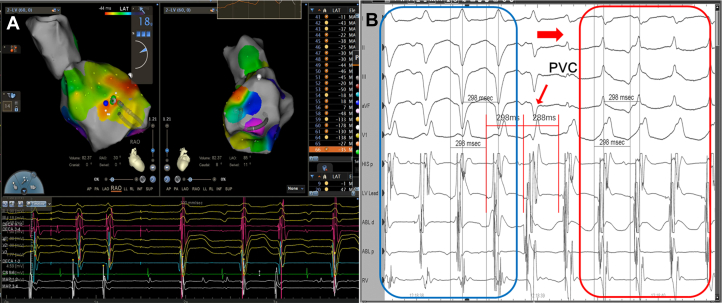 Figure 4
Figure 4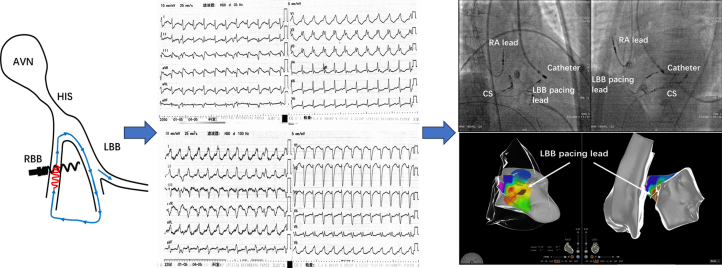 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiac pacing and defibrillation studies · Atrial Fibrillation Management and Outcomes
History of Presentation
A 65-year-old woman presented with recurrent palpitations for 1 month and re-exacerbation with dizziness for 1 day. On arrival, her blood pressure was 90/60 mm Hg, and she reported presyncope. Previous electrocardiograms had demonstrated a right bundle branch block pattern.Take-Home Messages
- •Sustained His-Purkinje system–related ventricular tachycardia may occur after left bundle branch area pacing.
- •Careful electrophysiologic assessment and accurate diagnosis are essential to minimize conduction system injury.
Past Medical History
The patient had a history of sick sinus syndrome, and she had undergone dual-chamber pacemaker implantation with left bundle branch area pacing (LBBAP) 1 month earlier. She had no known hypertension, diabetes, or coronary disease, and no drug allergies. There was no family history of sudden death.
Differential Diagnosis
Considerations included supraventricular tachycardia with aberrancy or atrioventricular re-entry, bundle branch re-entrant VT (BBRVT), and His-Purkinje system (HPS)–related ventricular tachycardia (VT) (fascicular/interfascicular).
Investigations
Twelve-lead electrocardiograms demonstrated 2 bundle branch block–like VT morphologies with similar ventricular rates (Figure 1). Device interrogation indicated ventriculoatrial dissociation (V:A = 3:1), supporting VT. Baseline laboratory results and transthoracic echocardiography were unremarkable.Figure 1. Emergency 12-Lead ECGs Showing 2 VT MorphologiesTwo bundle branch block–like VT morphologies with similar cycle lengths are demonstrated. In lead V1, one tracing shows an RBBB-like pattern and the other an LBBB-like pattern. LBBB = left bundle branch block; RBBB = right bundle branch block; VT = ventricular tachycardia.
Management
First procedure (index admission)
During VT, Purkinje-Purkinje (PP) interval changes preceded RR, and premature beats advanced the His potential with reset, which was diagnostic of HPS-related VT (Figure 2A). Intraprocedural intracardiac echocardiography showed the LBBAP lead on the anterior left ventricular (LV) septum, immediately adjacent to the earliest endocardial activation on 3-dimensional mapping (Figures 2B and 2C). Targeted LV septal endocardial ablation opposite the lead promptly terminated VT and rendered it noninducible, where a sharp left bundle branch potential was recorded preceding the local ventricular electrogram.Figure 2. Integrated Electrophysiological and Imaging Findings During VT Mapping and Ablation(A) High-gain intracardiac electrograms during VT showing Purkinje-Purkinje (PP) interval changes preceding RR changes, a diagnostic feature of HPS-related VT. (B) Fluoroscopy in the right anterior oblique and left anterior oblique projections depicting intracardiac catheter positions and the LBBAP lead traversing the interventricular septum. (C) Three-dimensional activation map integrated with intracardiac echocardiography shell shows the earliest LV anterior septal activation immediately adjacent to the LBBP lead marker. CS = coronary sinus; HPS = His-Purkinje system; LBB = left bundle branch; LBBAP = left bundle branch area pacing; LBBP = left bundle branch pacing; LV = left ventricular; RA = right atrial; VT = ventricular tachycardia.
Early recurrence and second procedure (postprocedure day 1)
During the second procedure, the VT was paroxysmal and nonsustained. Connecting the left bundle branch lead to a multichannel recorder confirmed early bundle electrograms and persistent PP-to-RR precedence. The earliest activation site remained located at the LV anterior septal region (Figure 3A). A fusion premature ventricular complex advanced the His potential, indicating a re-entrant mechanism. VT morphology switched between left anterior fascicular block–like and left posterior fascicular block–like without cycle-length change, favoring distal (interfascicular) re-entry over BBRVT (Figure 3B). Repeat focal ablation at the anterior LV septum terminated VT but resulted in complete atrioventricular block; the pacing lead was subsequently repositioned to the right ventricular septum, with stable pacing parameters achieved.Figure 33-Dimensional Activation Mapping and Electrophysiological Evidence of Distal HPS-Related VT During the Second Procedure(A) Second-procedure 3-dimensional activation map depicting earliest activation on the septal surface. (B) During mapping, a fusion premature ventricular complex advances the His potential and resets the tachycardia, while the QRS morphology shifts from an LAFB-like pattern (blue box) to an LPFB-like pattern (red box), consistent with a distal (interfascicular) re-entry mechanism. HPS = His-Purkinje system; LAFB = left anterior fascicular block; LPFB = left posterior fascicular block; PVC = premature ventricular complex; VT = ventricular tachycardia.
Outcome and Follow-Up
No VT recurred on in-hospital monitoring or 1-month ambulatory follow-up. Symptoms resolved completely, and pacing thresholds and sensing remained stable.
Discussion
To our knowledge, sustained HPS-related VT after LBBAP has not been previously reported. This case suggests that, in selected patients with underlying HPS disease, physiologic pacing in close proximity to the conduction system may facilitate sustained VT. A plausible substrate is either HPS injury from the left bundle branch lead—predisposing to BBRVT—or direct lead-mediated stimulation of the HPS.1 Because right-ventricular entrainment was not performed, the mechanism could not be definitively established; ablation was undertaken and resulted in complete atrioventricular block.2 Had classic BBRVT been confirmed, right bundle ablation would likely have been a more targeted strategy, particularly given the patient's preexisting complete right bundle branch block.3 Although the first ablation terminated VT, widespread HPS disease likely permitted distal Purkinje re-entry, accounting for recurrence and the need for a second intervention. A key lesson is that left bundle branch pacing may be followed by HPS-related re-entrant VT, mandating meticulous diagnostic confirmation and mechanistic differentiation before ablation. Taken together, this first documented case demonstrates that left bundle branch pacing can, in rare instances, be followed by sustained HPS-related VT and that both diagnosis and therapy are challenging; these observations may inform clinical decision-making and procedural planning in similar scenarios.Visual SummaryIllustration of His-Purkinje System–Related Ventricular Tachycardia After Left Bundle Branch Area Pacing, Showing Successful Ablation But Also Underscoring Important Limitations in the Diagnostic and Procedural ApproachAVN = atrioventricular node; CS = coronary sinus; LBB = left bundle branch; RA = right atrium; RBB = right bundle branch.
Conclusions
This first documented case shows that sustained HPS-related VT may occur after LBBAP. Careful diagnostic confirmation and individualized ablation are required, given the risk of conduction injury and pacing revision.
Funding Support and Author Disclosures
This research was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0521906). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nogami A.Komatsu Y.Talib A.K.Purkinje-related ventricular tachycardia and ventricular fibrillation: solved and unsolved questions JACC Clin Electrophysiol 92023217221963749824710.1016/j.jacep.2023.05.040 · doi ↗ · pubmed ↗
- 2Voskoboinik A.Gerstenfeld E.P.Moss J.D.Complex re-entrant arrhythmias involving the His-Purkinje system: a structured approach to diagnosis and management JACC Clin Electrophysiol 62020148814983321380810.1016/j.jacep.2020.06.009 · doi ↗ · pubmed ↗
- 3Chen H.Shi L.Yang B.Electrophysiological characteristics of bundle branch reentry ventricular tachycardia in patients without structural heart disease Circ Arrhythmia Electrophysiol 1172018 e 00604910.1161/CIRCEP.117.00604929986947 · doi ↗ · pubmed ↗