Functional Outcomes of Intensive Rehabilitation Versus Fusion Surgery in Patients With Low Back Pain Due to Lumbar Degenerative Spine Disease: A Systematic Review and Meta-Analysis
Tito Guillermo D Rejante, Kevin Paul B Ferraris, Joseph Erroll V Navarro, Kenny S Seng, Jose Carlos S Alcazaren

TL;DR
This study compares the effectiveness of spinal fusion surgery and intensive rehabilitation for chronic low back pain caused by degenerative spine disease.
Contribution
The study provides a meta-analysis comparing functional outcomes of spinal fusion and rehabilitation for lumbar degenerative disease.
Findings
Spinal fusion showed a significant improvement in disability scores compared to rehabilitation.
Fusion surgery also showed better results in reducing low back pain.
There was no significant difference in leg pain improvement or overall patient outcome between the two treatments.
Abstract
Lumbar degenerative disease is mostly managed non-operatively, but lumbar spinal fusion has been used for almost a century. It has shown clinical efficacy in decreasing pain and disability scores and allowing patients to return to work. However, spinal fusion may not be clinically effective and may place a financial burden on patients. The alternative to spinal fusion is physical therapy and rehabilitation for lumbar degenerative diseases. This study aims to compare the functional outcomes of intensive rehabilitation and lumbar spine fusion surgery among patients with chronic low back pain from lumbar spine degenerative disease. We conducted a systematic search of clinical trials on the topic, followed by a meta-analysis using a random-effects model. The functional outcomes compared included the Oswestry Disability Index (ODI) score, improvement in low back pain and leg pain, as well…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
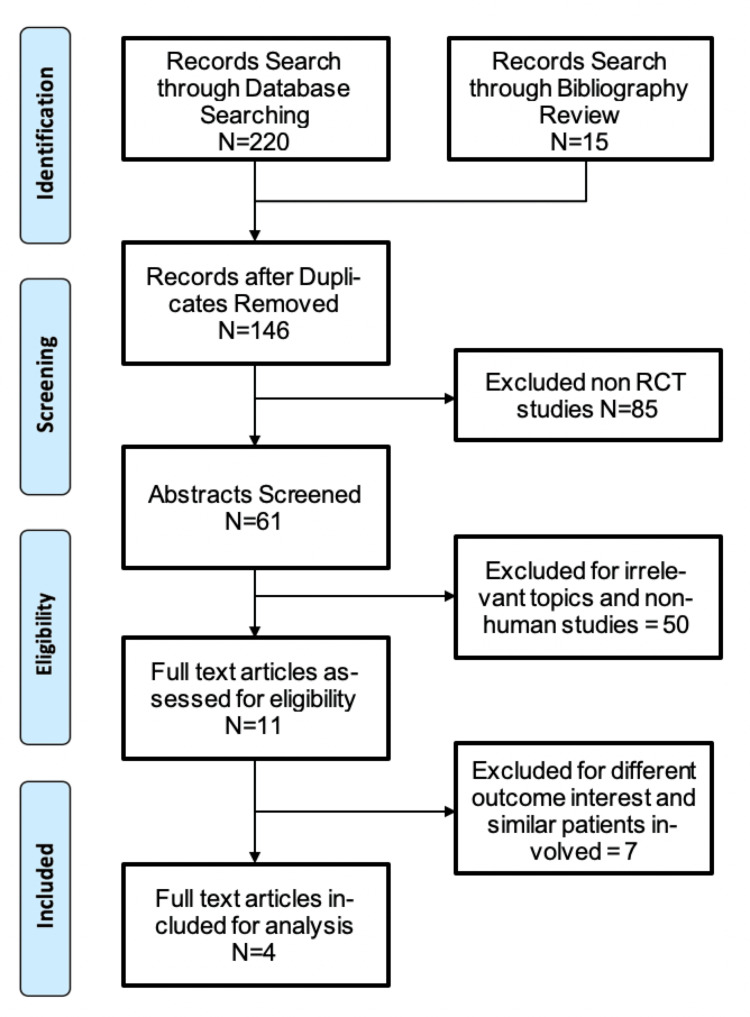 Figure 1
Figure 1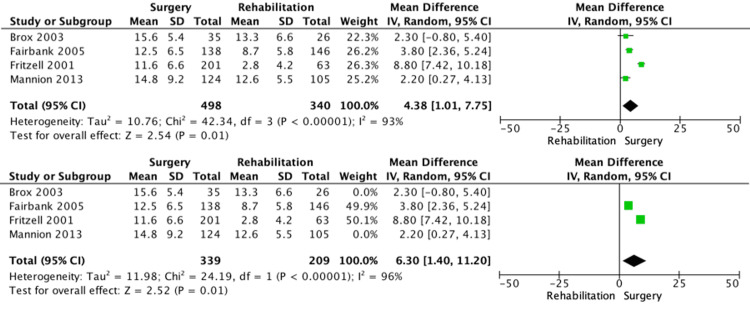 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4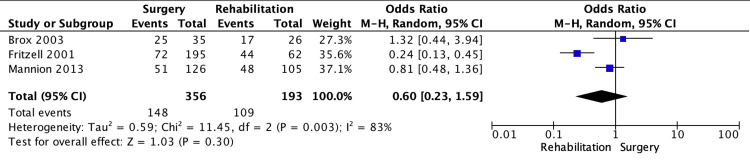 Figure 5
Figure 5| Study | Randomised patients (surgery/rehabilitation or physical therapy) | Intervention | Follow-up interval | Inclusion criteria | Setting | Tool | Endpoints | Reference |
| Fairbank et al. (2005) | 176/173 | Intensive rehabilitation/spinal fusion surgery | 2 years | Aged between 18 and 55, with more than a 12-month history of chronic low back pain (with or without referred pain), and irrespective of whether they had had previous root decompression or discectomy | United Kingdom | Oswestry disability index and the shuttle walking test, SF-36 questionnaire | No difference | [ |
| Fritzell et al. (2001) | 72/222 | Three types of spinal fusion surgery (posterolateral fusion with variable screw placement and interbody bone graft)/physical therapy (nonsurgical) | 6 months, 12 months, 2 years | Aged 25-65 years and of both sexes with severe chronic low back pain may have had previous spine surgery, except for successful removal of a herniated disc more than 2 years before entering the study, and with no persistent nerve root symptoms | Sweden | Oswestry disability index, visual analog scale (VAS), general function score (GFS), and Zung depression scale | Decrease in disability, pain, and depression, and the overall result was significantly greater in the surgical group | [ |
| Mannion et al. (2013) | 242/231 | Spinal fusion surgery/multidisciplinary cognitive-behavioral and exercise rehabilitation | 2 years, 11 years | Aged 18-55 years (UK), 25-60 years (Norway); low back pain duration of at least 1 year | United Kingdom and Norway | Oswestry disability index score | No statistically or clinically significant differences between treatment groups for ODI scores | [ |
| Brox et al. (2003) | 35/26 | Lumbar fusion surgery/cognitive Intervention and exercises | 1 year | Age 25-60 years. Low back pain duration for at least 1 year | Norway | Oswestry disability index score | Equal improvement in patients with chronic low back pain and disc degeneration randomized to cognitive intervention and exercises, or lumbar fusion | [ |
| Criteria | Fairbank et al. (2005) [ | Fritzell et al. (2001) [ | Mannion et al. (2013) [ | Brox et al. (2003) [ |
| Randomization sequence generation | Low | Low | Low | Low |
| Allocation concealment | Low | Low | High | Low |
| Blinding | High | High | High | High |
| Incomplete data | Low | Low | High | Low |
| Selective reporting | Low | Low | Low | Low |
| Overall RoB | Low | Low | Low | Low |
| Remarks | High risk for performance bias | High risk for performance bias | High risk for selection, performance, and attrition bias; >Risk for reporting bias | High risk for performance bias |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Musculoskeletal pain and rehabilitation · Scoliosis diagnosis and treatment
Introduction and background
Back pain is widespread, with over 600 million individuals afflicted, and is the leading cause of years of disability worldwide [1]. Low back pain is the hallmark of lumbar degenerative disease; unfortunately, it is a nonspecific complaint when trying to determine which patients will benefit most from surgery [2]. Initial management is mostly non-operative, but lumbar spinal fusion has been used for almost a century. It has shown clinical efficacy in decreasing pain and disability scores and allowing patients to return to work [2]. The principle of spinal fusion is to provide a biomechanically lasting interbody union, which can be accomplished using different surgical approaches, implants, and grafts [3]. However, fusion procedures have not been effective for all patients, and the alternative is physical therapy and rehabilitation.
Physical rehabilitation is the most common method used to apply non-operative treatment of symptoms in patients with chronic low back pain. Therapeutic protocols may include modalities for pain relief, bracing, exercise, ultrasound, electrical stimulation, and activity modification. Physical rehabilitation is recommended to reduce pain, restore range of motion and function, strengthen and stabilize the spine, and restore neural tissue mobility [4,5]. In low- and middle-income countries, where the costs of spinal implants could be prohibitive for the majority of patients with chronic low back pain, this study becomes relevant in determining whether intensive rehabilitation may become a reasonable option.
In randomized controlled trials (RCTs) by Brox et al. [6], Fairbank et al. [7], and Mannion et al. [4], there were no statistically significant differences between treatment groups randomized to either lumbar fusion surgery or cognitive intervention and exercises. In contrast, the RCTs by Möller and Hedlund [8] and Fritzell et al. [9] showed that patients randomized to the surgical group had better outcomes than their non-surgical counterparts. For clinicians who deliberate and contemplate these two diverging treatment options, it becomes imperative to clarify the weight of the evidence through a meta-analysis.
This article was previously shared as a preprint on the Research Square server on April 29, 2021 (https://doi.org/10.21203/rs.3.rs-478001/v1).
Review
Materials and methods
Search Strategy
We conducted a systematic review and meta-analysis of prospective studies and RCTs published between January 2000 and June 2020. A detailed search was conducted in PubMed, the Cochrane Central Registry of Clinical Trials, and EMBASE using the following keywords: “chronic low back pain,” “lumbar spine,” “degenerative disease,” “spinal fusion,” “lumbar fusion,” “surgical stabilization,” “physical therapy,” and “rehabilitation.” An effort was made to search for relevant grey literature through OpenGrey, BASE, and CORE.
Eligibility Criteria
The study types included in our research were both RCTs and prospective studies. RCTs comparing the outcomes between groups of patients with chronic low back pain for more than one year from degenerative disc disease or spondylosis (with or without spondylolisthesis) treated with either fusion surgery or rehabilitation, and studies with random allocation between groups, were considered eligible for this study. Functional outcomes included the Oswestry Disability Index (ODI), low back pain, leg pain, and overall patient outcome. There should be at least a one-year follow-up.
Exclusion criteria included case reports, letters to the editor, commentaries, cross-sectional surveys, and documentaries. Trials involving patients with low back pain due to fracture, metastasis, or inflammation, as well as studies comparing different forms of surgical interventions and studies with different outcomes of interest, were excluded. Data collection was performed by two independent authors in accordance with the mentioned eligibility criteria. Any discrepancies were resolved through collaborative discussion.
Study Selection and Reporting
All included articles were independently screened and assessed for validity and eligibility. The appraisal was done using the Cochrane Methodological Risk Assessment Tool. The following data were extracted from each of the included trials: author, year of publication, type of population, study design, sample size, duration of study, intervention, comparator, study outcomes, and location of population. Our report followed the generally accepted guideline, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Statistical Analysis
Data were extracted from tables and the associated text describing the outcomes before and after treatment. The functional outcomes were pretreatment and posttreatment differences based on the ODI, low back pain, or leg pain, determined through the Visual Analog Scale (VAS) score, and overall patient outcome. The homogeneity of odds ratios (ORs) was tested using Cochran's Q statistic. If homogeneity was rejected at the 0.1 level, the ORs were analyzed using the random-effects model, with the presumption that multiple potential sources of heterogeneity were present in the included studies. The overall ORs were computed using the Cochran-Mantel-Haenszel method. Meta-analysis results were presented as mean differences (MDs) and standard deviations (SDs), with 95% confidence intervals (CIs), and were graphically displayed as forest plots. The inverse variance method was used to calculate estimates for continuous variables. Review Manager version 5.4 (The Cochrane Collaboration, Copenhagen, Denmark) was the software used for the analyses.
Results
Search Results
The search revealed 220 articles from a database search and 15 articles from a bibliography search. After 89 duplicates and 85 non-RCTs were excluded, 61 articles were screened, and full-text articles were reviewed. Of the 11 screened-in articles, seven were further excluded because they had different outcome interests and similarities in the patients involved. Four studies fulfilled the eligibility criteria and were analyzed after a full-text systematic review. Figure 1 shows the flow of the selection process, while Table 1 summarizes the characteristics of the included studies.
Flow diagram for data extraction strategy in conformity with the PRISMA guidelinesPRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study Characteristics
The four studies included were published from 2000 to 2020, involving 1,177 patients. Studies took place in the United Kingdom, Sweden, and Norway. All of the studies involved patients with chronic low back pain. All studies had lumbar fusion as the main surgical approach, described as posterolateral fusion, compared with rehabilitation and physical therapy. The non-surgical approach, which includes rehabilitation, physical therapy, and exercises, had different programs and routines across the studies. Follow-up ranged from 1 year to 11 years. Four of the studies had a follow-up period of two years. All of the studies used the ODI to measure changes in disability. Four studies used the VAS to measure changes in pain. Most of the studies were single-blinded. There were no significant differences in baseline characteristics of the groups being compared, and all studies reported randomization. Four studies had adequate follow-up. The study by Mannion et al. [4] shows a 45% dropout in their long-term follow-up of 11 years, which may lead to attrition bias. Table 2 gives a summary of the risk-of-bias assessment for the included studies.
Functional outcomes
Oswestry Disability Index (ODI)
The forest plot shows the MD in change in ODI between the lumbar spine fusion surgery and rehabilitation groups (Figure 2). All studies showed improvement in the change in ODI, favoring surgery. There was a 4.38 improvement in the change in ODI, with high heterogeneity among the studies (95% CI: 1.01-7.75; p = 0.01; I² = 93%). The sensitivity analysis (Figure 2) shows the MD in change in ODI between the lumbar spine fusion surgery and rehabilitation groups at two years. Studies by Mannion et al. and Brox et al. have 11-year and 1-year follow-ups, respectively [4,6]. All studies showed improvement in the change in ODI after two years, favoring surgery. There was a 6.3 improvement in the change in ODI (95% CI: 1.4-11.2; p = 0.01; I² = 96%).
Forest plotConstructed forest plot among patients with chronic low back pain using a random-effects model. Comparator 01: lumbar spine fusion surgery versus rehabilitation. Outcome 01: change in Oswestry Disability Index.Sensitivity analysis among patients with chronic low back pain using a random-effects model. Comparator 01: lumbar spine fusion surgery versus rehabilitation. Outcome 01: change in Oswestry Disability Index at two years.Source: [4,6,7,9]
Low Back Pain
The subgroup analysis shows the MD in improvement in low back pain between the lumbar spine fusion surgery and rehabilitation groups (Figure 3). All studies showed improvement in low back pain, favoring surgery. There was a 9.62 improvement in VAS score for low back pain (95% CI: 0.57-18.67; p = 0.04; I² = 97%).
Subgroup analysis of low back painSubgroup analysis of improvement in low back pain using a random-effects model between lumbar spine fusion surgery and rehabilitation. Comparator 01: lumbar spine fusion surgery versus rehabilitation. Outcome 02: improvement in low back pain.Source: [6,7,9]
Leg Pain
The subgroup analysis shows the MD in improvement in leg pain between the lumbar spine fusion surgery and rehabilitation groups (Figure 4). There was a 7.2 improvement in the VAS score for leg pain (95% CI: -8.58 to 22.97; p = 0.37; I² = 98%); however, the effect was not significant.
Subgroup analysis of leg painSubgroup analysis of improvement in leg pain using a random-effects model between lumbar spine fusion surgery and rehabilitation. Comparator 01: lumbar spine fusion surgery versus rehabilitation. Outcome 03: improvement in leg pain.Source: [6,9]
Overall Patient Outcome
The subgroup analysis shows the OR in overall patient outcomes between the lumbar spine fusion surgery and rehabilitation groups (Figure 5). There was no significant difference in the overall patient outcome (95% CI: 0.23-1.59; p = 0.30; I² = 83%).
Subgroup analysis of overall patient outcomeSubgroup analysis of overall patient outcome using a random-effects model between lumbar spine fusion surgery and rehabilitation. Comparator 01: lumbar spine fusion surgery versus rehabilitation. Outcome 04: overall patient outcome.Source: [4,6,9]
Discussion
This meta-analysis of five RCTs showed a significant improvement in disability index scores and low back pain among patients who underwent lumbar spine fusion surgery, compared to those who received intensive rehabilitation. However, these findings were in contrast with the studies of Mannion et al., Brox et al., Fairbank et al., and Fritzell et al. [4,6,7,9], which revealed that intensive rehabilitation is comparable to lumbar fusion surgery. Notably, the two options showed no significant differences in leg pain scores or improvement in overall patient outcome, as confirmed by the patients’ subjective validation of improvement in outcome and reduced pain scores.
Pain is naturally subjective, and validated pain tools were used across the included studies to quantify pain intensities. Lumbar fusion surgery showed significant improvement in low back pain; however, scores in leg pain did not significantly improve. Additionally, no statistical difference was seen between the two treatments regarding overall patient outcomes. These results align with those of Chou et al. [10], which similarly found intensive rehabilitation to be comparable to fusion surgery in patients with low back pain and lumbar spondylolisthesis. However, patients with lumbar degenerative disease may benefit more from fusion surgery, particularly those presenting with stenosis and evidence of instability. Also, the landmark Spine Patient Outcomes Research Trial (SPORT), with randomized (n = 304) and observational (n = 303) patients with lumbar spondylolisthesis, supports these findings, showing that surgery yielded superior outcomes at two-, four-, and eight-year follow-up [11-13].
The forest plot on the change in the disability score highlighted a rather high heterogeneity of I² = 98% (Figure 2). Many factors may contribute to this variability, such as the duration of the evaluation. To address this variable, a sensitivity analysis included only studies with longer follow-ups of more than two years. Despite this, the heterogeneity remained high, which may suggest that other variables, such as rehabilitation strategies and surgical techniques, influenced the results. In addition, studies of these kinds of treatments, where blinding is difficult, are subject to performance bias, which may have been a contributing factor.
Given the overall findings, lumbar spine fusion surgery appears to offer better outcomes in lowering disability and improving low back pain among patients with chronic low back pain due to degenerative causes, such as spondylolisthesis. These findings are consistent with the results of the study by Möller and Hedlund [8], which demonstrated that surgical management has an advantage over an intensive exercise program in addressing such cases, in terms of improved function and reduced low back pain. Intensive rehabilitation serves as a viable alternative for patients who do not prefer surgery, as it appears comparable to lumbar spinal fusion surgery in improving leg pain and overall patient outcomes. Considering factors such as costs and accessibility, and the presence of comorbid conditions that may contraindicate surgery or general anesthesia, intensive rehabilitation represents a reasonable option for many patients.
Conclusions
Among patients with chronic low back pain, lumbar spine fusion surgery showed improvement in functional outcomes related to changes in disability and low back pain, when compared with intensive rehabilitation. However, the two treatment options showed no differences with respect to improvement in leg pain and overall patient outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Years lived with disability (YL Ds) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010 Lancet Vos T Flaxman AD Naghavi M 2163219638020122324560710.1016/S 0140-6736(12)61729-2PMC 6350784 · doi ↗ · pubmed ↗
- 2State of the union: a review of lumbar fusion indications and techniques for degenerative spine disease J Neurosurg Spine Reid PC Morr S Kaiser MG 1143120193126113310.3171/2019.4.SPINE 18915 · doi ↗ · pubmed ↗
- 3Lumbar spinal fusion - indications and techniques (Article in German)Orthopäde Schnake KJ Rappert D Storzer B Schreyer S Hilber F Mehren C 50584820193055244910.1007/s 00132-018-03670-w · doi ↗ · pubmed ↗
- 4Comparison of spinal fusion and nonoperative treatment in patients with chronic low back pain: long-term follow-up of three randomized controlled trials Spine J Mannion AF Brox JI Fairbank JC 143814481320132420041310.1016/j.spinee.2013.06.101 · doi ↗ · pubmed ↗
- 5Surgical stabilisation of the spine compared with a programme of intensive rehabilitation for the management of patients with chronic low back pain: cost utility analysis based on a randomised controlled trial BMJ Rivero-Arias O Campbell H Gray A Fairbank J Frost H Wilson-Mac Donald J 123933020051591153610.1136/bmj.38441.429618.8FPMC 558091 · doi ↗ · pubmed ↗
- 6Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration Spine (Phila Pa 1976) Brox JI Sørensen R Friis A 191319212820031297313410.1097/01.BRS.0000083234.62751.7A · doi ↗ · pubmed ↗
- 7Randomised controlled trial to compare surgical stabilisation of the lumbar spine with an intensive rehabilitation programme for patients with chronic low back pain: the MRC spine stabilisation trial BMJ Fairbank J Frost H Wilson-Mac Donald J Yu LM Barker K Collins R 123333020051591153710.1136/bmj.38441.620417.8FPMC 558090 · doi ↗ · pubmed ↗
- 8Surgery versus conservative management in adult isthmic spondylolisthesis: a prospective randomized study: part 1Spine Möller H Hedlund R 17111715252000 https://journals.lww.com/spinejournal/fulltext/2000/07010/Surgery_Versus_Conservative_Management_in_Adult.16.aspx 1087014810.1097/00007632-200007010-00016 · doi ↗ · pubmed ↗