Endoscopic gluteal tendon repair reduces complication rates while achieving outcomes comparable to open repair: A multilevel meta‐analysis
Nikolai Ramadanov, Maximilian Voss, Ariana Lott, Robert Hable, Robert Prill, Roland Becker, Marko Ostojic, Plamen Penchev, Ingo J. Banke

TL;DR
Endoscopic gluteal tendon repair offers similar outcomes to open surgery but with fewer complications, making it a favorable option when available.
Contribution
This study provides the first multilevel meta-analysis comparing open and endoscopic gluteal tendon repair outcomes and complication rates.
Findings
Both open and endoscopic repair show comparable functional and pain improvements in the short term.
Endoscopic repair has a lower complication rate compared to open repair.
No significant differences were found in efficacy between the two techniques when using MCID units.
Abstract
The purpose of this systematic review and multilevel meta‐analysis was to compare short‐term functional outcomes, pain relief, and complication rates between open and endoscopic gluteal tendon repair, expressed as functional improvement normalized to minimal clinically important difference (MCID) units. The hypothesis was that endoscopic repair would provide comparable clinical efficacy with a lower complication rate compared with open repair. PubMed, Embase, CENTRAL and Epistemonikos were searched to 15 October 2025. Eligible primary studies reporting postoperative or change outcomes were synthesized with a frequentist multilevel random‐effects model (inverse variance, restricted maximum likelihood estimation, Hartung–Knapp adjustment). Thirty‐four studies (1278 patients; 1283 hips) met criteria. Postoperative functional MCID (27 studies; n = 1005): overall 9.01 (95% confidence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
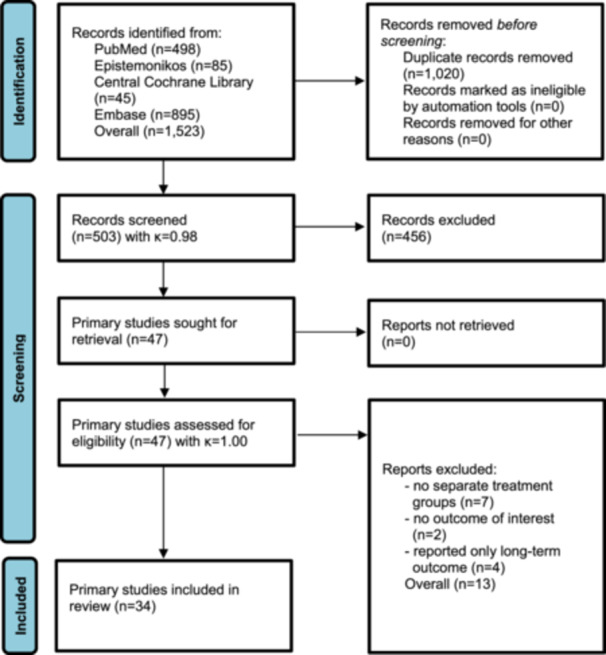 Figure 1
Figure 1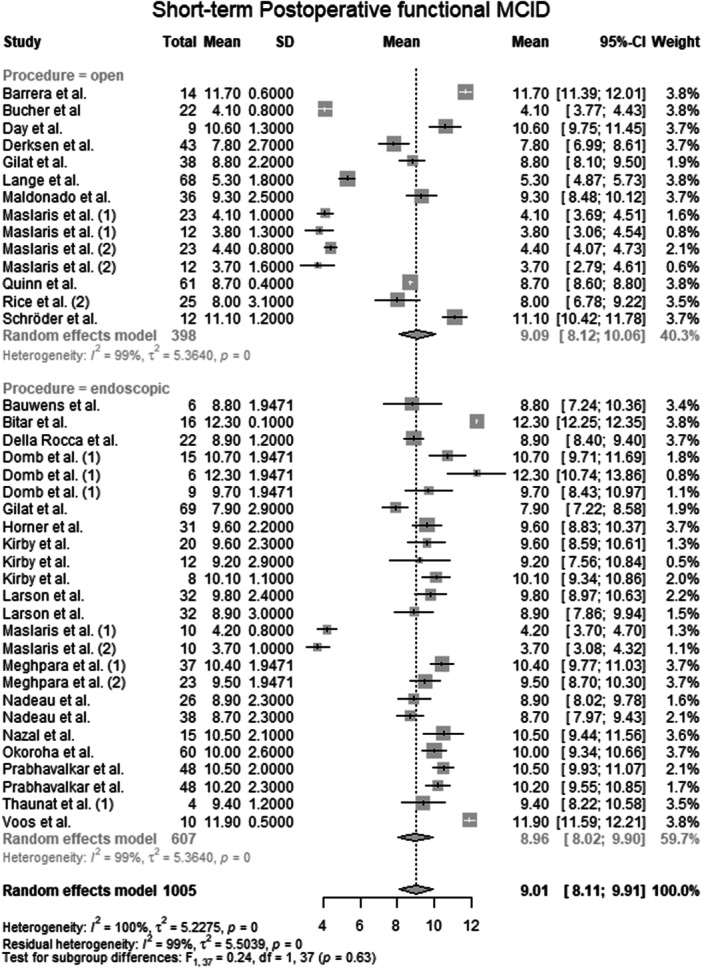 Figure 2
Figure 2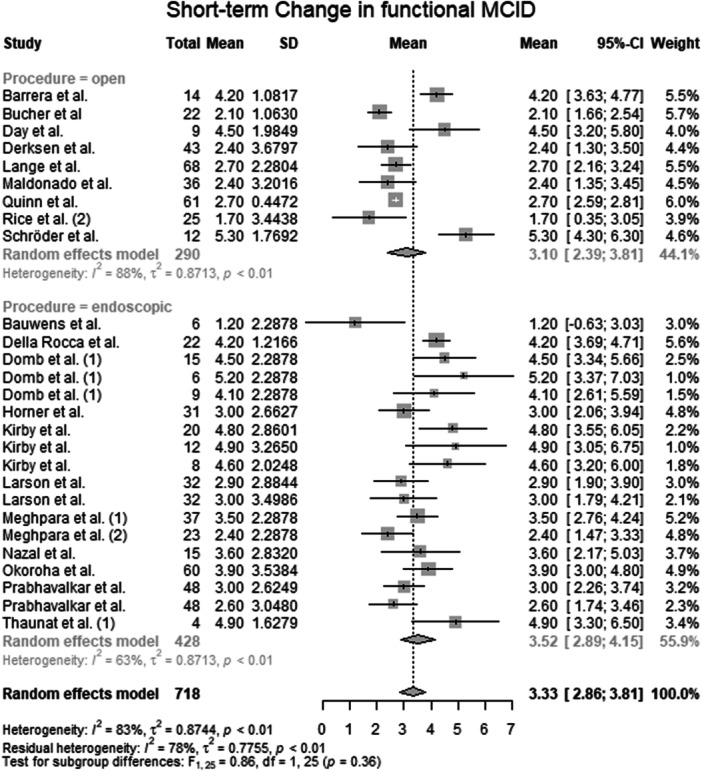 Figure 3
Figure 3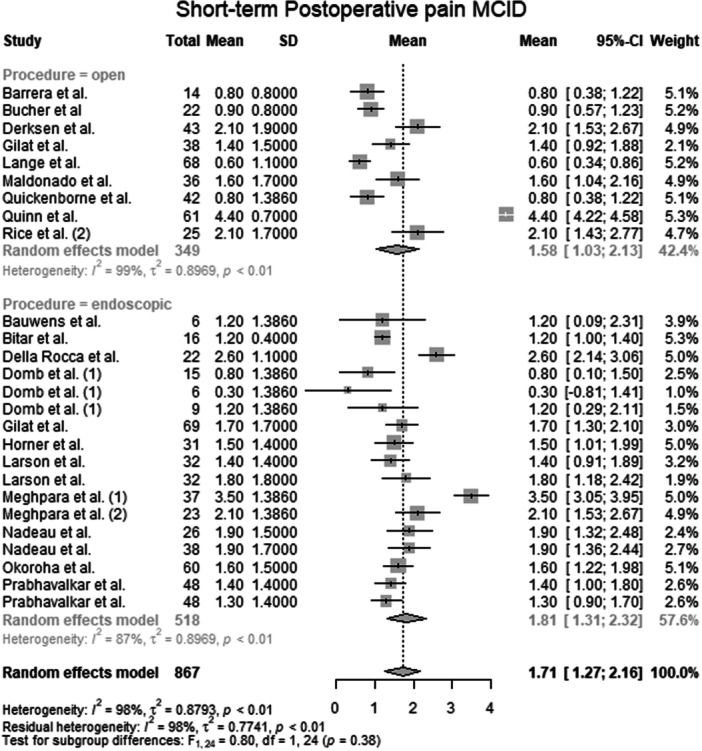 Figure 4
Figure 4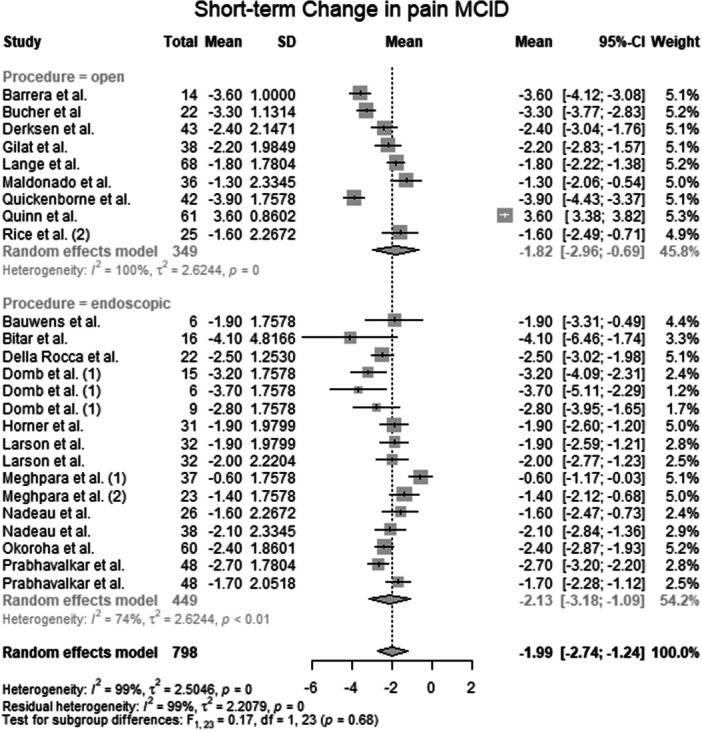 Figure 5
Figure 5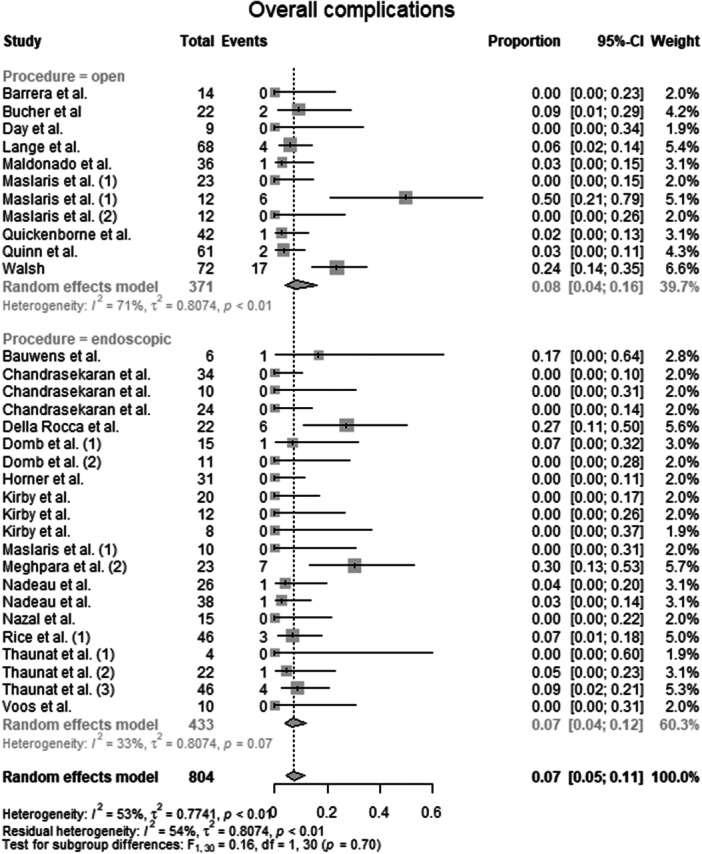 Figure 6
Figure 6| Author | Origin | Journal | Study design | LoE | Operation | Patients, | Hips, | Age, years ± SD (range) | Male sex, | BMI, kg/m2 ± SD (range) | Follow‐up duration (months) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Barrera M et al. 2021 [ | Switzerland |
| Retrospective case series | IV | Mini‐open | 14 | 14 | 62.4 ± 18.0 | 1 (7.0) | 14.3 ± 7.0 (6‐24) | |
| Bauwens PH et al. 2021 [ | France | Orthopaedics & Traumatology: Surgery & Research | Retrospective case series | IV | Endoscopic | 6 | 6 | 73.3 | 2 (33.3) | 28.2 | >24 |
| Bitar AC et al. 2023 [ | Brazil |
| Retrospective case series | IV | Endoscopic | 16 | 16 | 65.0 (32.0–73.0) | 1 (6.0) | 42 (12–131) | |
| Bucher TA et al. 2013 [ | United Kingdom |
| Prospective case series | IV | Open | 22 | 22 | 62.0 (49.0–74.0) | 3 (13.6) | 12 | |
| Chandrasekaran S et al. 2015 [ | USA |
| Retrospective case series | IV | Endoscopic | 34 | 34 | 57.0 (20.1–78.8) | 2 (6.0) | 27.9 (19.2–40.4) | 27.2 (24.4–45.9) |
| Endoscopic | 10 | 10 | 54.4 (20.1–71.1) | 0 (0.0) | 28.5 (21.4–34.5) | ||||||
| Endoscopic | 24 | 24 | 58.7 (41.3–78.8) | 2 (8.0) | 28.0 (19.2–40.4) | ||||||
| Day MA et al. 2022 [ | USA |
| Prospective case series | IV | Open | 9 | 9 | 60.3 ± 9.3 | 1 (11.1) | 29.4 ± 6.3 | 6 |
| Della Rocca F et al. 2023 [ | Italy |
| Retrospective case series | IV | Endoscopic | 22 | 22 | 58.6 (52.0–69.0) | 4 (18.2) | 28.5 (20.6–34.3) | 42 ± 14.5 (24–72) |
| Derksen A et al. 2022 [ | Germany |
| Retrospective case series | IV | Open | 43 | 43 | 65.2 ± 11.3 (41.3–85.1) | 11 (25.6) | 22.8 ± 9.7 (9–46) | |
| Domb BG et al. 2013 (1) [ | USA |
| Prospective case series | IV | Endoscopic | 15 | 15 | 57.8 (44.0–74.0) | 1 (6.7) | 26.2 (19.9–32.6) | 27.9 (24–37) |
| Endoscopic | 6 | 6 | 57.3 (49.0–70.0) | 25.5 (24.0–26.9) | |||||||
| Endoscopic | 9 | 9 | 58.1 (44.0–74.0) | 26.5 (19.9–32.6) | |||||||
| Domb BG et al. 2024 (2) [ | USA |
| Prospective case series | IV | Endoscopic | 11 | 11 | 60.1 ± 10.1 (46.2–74.8) | 1 (9.1) | 25.4 ± 4.9 (24.0–34.2) | 124.4 ± 55.1 (120.0–153.1) |
| Gilat R et al. 2024 [ | Israel |
| Retrospective case series | IV | Open | 38 | 38 | NR | NR | NR | 37.2 ± 16.8 |
| Endoscopic | 69 | 69 | NR | NR | NR | ||||||
| Horner NS et al. 2023 [ | USA |
| Retrospective cohort study | III | Endoscopic | 31 | 31 | 50.8 ± 7.3 | 4 (12.9) | 27.9 ± 5.2 | 26.2 ± 5.2 |
| Kirby D et al. 2020 [ | USA |
| Retrospective case series | IV | Endoscopic | 20 | 20 | 51.3 ± 11.9 | 5 (21.0) | 25.3 ± 3.9 | 28.8 ± 11.3 |
| Endoscopic | 12 | 12 | 54.8 ± 11.3 | 4 (27.0) | 25.1 ± 4.0 | ||||||
| Endoscopic | 8 | 8 | 46.0 ± 11.4 | 1 (12.0) | 25.5 ± 4.0 | ||||||
| Lange J et al. 2024 [ | Denmark |
| Retrospective observational study | IV | Open | 67 | 68 | 59.0 (56.0–61.0) | 0 (0.0) | 28.0 (27.0–29.0) | 12 |
| Larson JH et al. 2024 [ | USA |
| Retrospective propensity‐matched cohort study | III | Endoscopic | 32 | 32 | 50.6 ± 8.0 | 3 (9.4) | 27.8 ± 6.2 | 24 |
| Endoscopic | 32 | 32 | 52.7 ± 8.9 | 1 (3.1) | 28.9 ± 6.8 | ||||||
| Maldonado DR et al. 2020 [ | USA |
| Retrospective case series | IV | Open | 36 | 36 | 65.2 ± 12.7 (57.8–73.7) | 5 (13.9) | 29.0 ± 5.0 (26.4–31.2) | 40.8 ± 26.19 (24.16–46.20) |
| Maslaris A et al. 2020 (1) [ | Greece |
| Retrospective cohort study | III | Open | 23 | 23 | 68.0 ± 8.2 | 3 (13.0) | 29.0 ± 5.2 | 20.3 ± 12.5 (3–63) |
| Open | 12 | 12 | 67.0 ± 8.2 | 4 (33.0) | 29.7 ± 7.3 | ||||||
| Endoscopic | 10 | 10 | 59.0 ± 10.0 | 3 (30.0) | 25.8 ± 1.8 | ||||||
| Maslaris A et al. 2022 (2) [ | USA |
| Retrospective cohort study | III | Endoscopic | 10 | 38 | 64.0 ± 12.2 | 1 (10.0) | 28.2 ± 6.5 | 20.9 ± 12.5 |
| retrospectiv | Open | 6 | 23 | 63.0 ± 8.6 | 3 (50.0) | 27.7 ± 4.2 | |||||
| retrospectiv | Open | 12 | 16 | 69.5 ± 11.3 | 4 (25.0) | 30.2 ± 7.6 | |||||
| Meghpara MB et al. 2020 (1) [ | USA |
| Retrospective case series | IV | Endoscopic | 37 | 37 | 51.5 ± 10.5 (17.2–74.8) | 3 (8.1) | 27.7 ± 13.1 (19.4–40.4) | 73.4 (60.0–105.1) |
| Meghpara MB et al. 2021 (2) [ | USA |
| Retrospective comparative cohort study | III | Endoscopic | 23 | 23 | 62.7 ± 10.1 (36.9–74.4) | 1 (4.3) | 29.9 ± 4.2 (24.0–84.5) | 38.3 ± 19.2 (24.0–84.5) |
| Nadeau NJ et al. 2024 [ | USA |
| Retrospective comparative cohort study | III | Endoscopic | 26 | 26 | 57.0 ± 12.0 | 6 (13.0) | 29.0 ± 5.0 | ≥24 |
| Endoscopic | 38 | 38 | 59.0 ± 12.0 | 2 (5.0) | 28.0 ± 5.0 | ||||||
| Nazal MR et al. 2020 [ | USA |
| Prospective case series | IV | Endoscopic | 13 | 15 | 66.9 ± 9.0 | 3 (20.0) | 28.8 ± 3.9 | 31.2 ± 10.9 (24–60) |
| Okoroha KR et al. 2019 [ | USA |
| Retrospective case series | IV | Endoscopic | 60 | 60 | 57.9 ± 9.9 | 5 (8.3) | 27.6 ± 6.1 | 24 (22–24) |
| Prabhavalkar ON et al. 2023 [ | USA |
| Propensity‐matched comparative cohort study | III | Endoscopic | 48 | 48 | 53.3 ± 9.8 (30.9–72.2) | 4 (8.0) | 26.7 ± 4.6 (18.8–40.7) | 38.5 ± 15.7 (24.0–72.8) |
| Endoscopic | 48 | 48 | 54.3 ± 9.0 (32.1–76.0) | 3 (6.0) | 27.1 ± 4.3 (17.5–38.8) | 58.8 ± 17.2 (24.0–88.8) | |||||
| Quickenborne D et al. 2025 [ | Belgium |
| Prospective case series | IV | Open | 42 | 42 | 4 (9.5) | 12 (6–12) | ||
| Quinn M et al. 2024 [ | USA |
| Retrospective case series | IV | Mini‐open | 61 | 61 | 61.4 ± 1.3 | 2 (3.2) | 25.9 ± 1.13 (24–30.9) | |
| Rice MW et al. 2022 (1) [ | USA |
| Retrospective case series | IV | Endoscopic | 46 | 46 | 59.1 ± 8.9 | 6 (13.0) | 27.3 ± 6.9 | 72.0 |
| Rice MW et al. 2023 (2) [ | USA |
| Retrospective case series | IV | Open | 25 | 25 | 69.0 ± 6.8 | 1 (4.0) | 26.9 ± 5.0 | 37.2 (30.0–64.8) |
| Schröder JH et al. 2018 [ | Germany |
| Retrospective cohort study | IV | Open | 12 | 12 | 58.0 (43.0–75.0) | 0 (0.0) | 19 (12–46) | |
| Thaunat M et al. 2011 (1) [ | France |
| Retrospective case series | IV | Endoscopic | 4 | 4 | 68.5 (64.0–79.0) | 6 | ||
| Thaunat M et al. 2018 (2) [ | France |
| Retrospective case series | IV | Endoscopic | 20 | 22 | 66.0 ± 8.0 (45.0–82.0) | 3 (15.0) | 27.6 ± 4.9 | 31.7 ± 7.6 (24–47) |
| Thaunat M et al. 2021 (3) [ | France |
| Retrospective case series | IV | Endoscopic | 46 | 46 | 62.7 ± 9.0 (43.0–82.0) | 3 (6.5) | 25.7 ± 4.0 (19.0–34.0) | 46.7 ± 15 (24–72 |
| Voos JE et al. 2009 [ | USA |
| Prospective case series | IV | Endoscopic | 10 | 10 | 50.4 (33.0–66.0) | 2 (20.0) | 25 (19–38) | |
| Walsh MJ et al. 2011 [ | Australia |
| Retrospective cohort study | IV | Open | 72 | 72 | 62 (36.0–88.0) | 5 (7.0) | 12 | |
| Total | 1278 | 1283 | 59.6 (46.0–73.3) | 131 (10.2) | 27.6 (25.1–30.2) | 32.22 (6.0–124.4) | |||||
| Open surgery group | 490 | 491 | 54.2 (59.0–69.5 | 31 (6.3) | 28.7 (26.9–30.2) | 38.4 (6.0–40.8) | |||||
| Endoscopic surgery group | 788 | 792 | 57.7 (46.0–73.3) | 76 (9.6) | 27.3 (25.1–29.9) | 29.0 (6.0–124.4) | |||||
| Author | Bias due to confounding | Bias in selection of participants | Bias in classification of interventions | Bias due to deviations from intended interventions | Bias due to missing data | Bias in measurement of outcomes | Bias in selection of the reported result | Overall risk of bias |
|---|---|---|---|---|---|---|---|---|
| Barrera M et al. 2021 [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Bauwens PH et al. 2021 [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Bitar AC et al. 2023 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Bucher TA et al. 2013 [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Chandrasekaran S et al. 2015 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Day MA et al. 2022 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Della Rocca F et al. 2023 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Derksen A et al. 2022 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Domb BG et al. 2013 (1)[ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Domb BG et al. 2024 (2) [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Gilat R et al. 2024 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Horner NS et al. 2023 [ | Moderate | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Kirby D et al. 2020 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Lange J et al. 2024 [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Larson JH et al. 2024 [ | Moderate | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Maldonado DR et al. 2020 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Maslaris A et al. 2020 (1) [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Maslaris A et al. 2022 (2) [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Meghpara MB et al. 2020 (1) [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Meghpara MB et al. (2) 2021 [ | Moderate | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Nadeau NJ et al. 2024 [ | Moderate | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Nazal MR et al. 2020 [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Okoroha KR et al. 2019 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Prabhavalkar ON et al. 2023 [ | Moderate | Moderate | Low | Low | Low | Moderate | Moderate | Moderate |
| Quickenborne D et al. 2025 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Quinn M et al. 2024 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Rice MW et al. 2022 (1) [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Rice MW et al. 2023 (2) [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Schröder JH et al. 2018 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
| Thaunat M et al. 2011 (1) [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Thaunat M et al. 2018 (2) [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Thaunat M et al. 2021 (3) [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Voos JE et al. 2009 [ | Serious | Moderate | Low | Low | Low | Moderate | Moderate | Serious |
| Walsh MJ et al. 2011 [ | Serious | Moderate | Low | Low | Moderate | Moderate | Moderate | Serious |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBody Contouring and Surgery · Hip disorders and treatments · Tendon Structure and Treatment
INTRODUCTION
Gluteus medius and minimus tendon tears—often termed the ‘rotator cuff tears of the hip’—are increasingly recognized as a cause of chronic lateral hip pain and abductor dysfunction, particularly in middle‐aged to older women [25, 33]. They affect up to ~10% of native hips over 60 and up to 28% of osteoarthritic hips undergoing total hip arthroplasty (THA), with even higher prevalence after (revision) THA, where they contribute to persistent postoperative pain [7, 11, 26, 49]. Gluteal pathology is associated with inferior THA outcomes, even when asymptomatic [60].
Surgical repair is indicated when conservative treatment fails, and imaging confirms tendon detachment [30]. Traditionally, repair has been performed via an open approach using anchors or transosseous tunnels, analogous to rotator cuff repair [2, 22, 70]. More recently, endoscopic repair has emerged [20], with several described technique modifications including biological augmentation such as microfracture [29].
Current evidence suggests comparable functional outcomes between techniques, including pain relief, satisfaction, and strength recovery [13, 43], while open repair is associated with higher complication rates (7%–8% vs. ~0.7% endoscopic) [13, 33]. Open repair may remain preferable for retracted full‐thickness tears requiring mobilization or augmentation, with similarly low re‐tear rates (3%–4%) [33]. However, most available data derive from retrospective case series (Level IV), with few direct comparisons and no randomized trials [2, 13, 20]. Prior reviews reported functional improvement with both approaches but fewer complications after arthroscopy [33], while emphasizing the need for higher‐quality evidence [13]. Looney et al. [34] demonstrated that high‐grade fatty infiltration limits functional improvement but not pain relief, underscoring the influence of muscle quality and the limited scope of existing analyses.
Despite multiple previous reviews, the literature remains limited by small sample sizes, descriptive synthesis, heterogeneous patient‐reported outcome measure (PROM) instruments and a lack of clinically interpretable pooled effect estimates. Importantly, no prior synthesis has applied a multilevel meta‐analytic framework or standardized outcomes using minimal clinically important difference (MCID) units to harmonize heterogeneous PROMs.
The purpose of this study was to compare short‐term functional outcomes, pain relief, and complication rates between open and endoscopic gluteal tendon repair using a multilevel meta‐analysis. It was hypothesized that endoscopic repair achieves comparable clinical efficacy in function and pain, while being associated with lower complication rates compared with open repair.
METHODS
Definition
Several terms are used in the literature to describe injuries of the lateral hip tendons, including gluteus medius tendon, gluteus minimus tendon, hip abductor tendon, gluteal tendon and hip rotator cuff. As these terms refer to the same anatomical structures involved in abductor function, the term ‘gluteal tendon’ was used consistently throughout this study.
Reporting standards and protocol registration
The peer‐reviewed study protocol [57] was registered in the International Prospective Register of Systematic Reviews (PROSPERO) on 11 July 2025 (CRD420251088765). This meta‐analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) 2020 guidelines [47], with the completed checklist provided as Table S1. The study further followed the 2025 Transparency in the Reporting of Artificial Intelligence (TITAN) guideline [1], with the completed checklist provided as Table S2. An author self‐assessment using A MeaSurement Tool to Assess systematic Reviews (AMSTAR) 2 [63] was performed by two independent reviewers to document adherence to critical methodological domains; the completed checklist is provided in Table S3.
Search strategy and study selection
A comprehensive database search was conducted in PubMed, Embase, CENTRAL (Cochrane Library) and Epistemonikos, covering studies published up to 15 October 2025. Boolean logic was applied using database‐specific syntax, including: ((gluteus medius) OR (gluteus minimus) OR (gluteal tendon) OR (hip abductor)) AND ((arthroscopy) OR (endoscopy) OR (endoscopic) OR (arthroscopic) OR (open)). No restrictions were applied regarding language or publication year. Two reviewers (M. V. and A. L.) independently performed a two‐stage screening process (title/abstract, then full text). Disagreements were resolved by a third reviewer (N. R.). Inter‐rater reliability was assessed using Cohen's kappa (κ).
Eligibility criteria
Eligible studies included randomized controlled trials (RCTs), prospective or retrospective observational studies and case series. Case reports, narrative reviews and editorials were excluded. Exclusion criteria were: (1) insufficient description of surgical technique and (2) absence of relevant functional or pain‐related outcomes. Importantly, eligibility was determined by the availability of outcomes assessed at short‐term follow‐up (≤24 months), irrespective of the maximum follow‐up duration reported. If both short‐ and long‐term outcomes were available, only short‐term data were extracted; studies reporting exclusively long‐term outcomes were excluded.
Data extraction
Data were independently extracted by two reviewers (M. V. and A. L.), with discrepancies resolved by consensus with a third reviewer (N. R.). Extracted variables included author, year, country, sample size, demographics, study design, risk of bias, follow‐up and outcome measures. Missing standard deviations were addressed by contacting authors, estimating from reported ranges (range/4) or imputing using established methods [74]. PROM scoring systems were reviewed to ensure directional consistency. Visual analogue scale (VAS) scores were standardized to a 0–10 scale, and Western Ontario and McMaster Universities Osteoarthritis Index scores were inverted so that higher values consistently indicated better outcomes.
MCID normalization
PROM values were standardized by expressing outcomes in MCID units, calculated by dividing observed means and standard deviations by the respective MCID of each instrument. This approach enabled harmonization across heterogeneous PROMs and pooling into a single functional MCID outcome [55].
Primary outcome analysis
Primary outcomes comprised postoperative functional outcomes and change scores, expressed in MCID units; postoperative pain outcomes and their change scores, also expressed in MCID units and overall complication rates. Postoperative functional MCID reflects functional PROM values normalized to the MCID, whereas change in functional MCID represents the pre‐ to postoperative change expressed relative to the MCID (not a change of the MCID itself). Analogous definitions applied to postoperative pain MCID and change in pain MCID.
Secondary outcome analyses
Secondary analyses included PROM‐specific evaluations (International Hip Outcome Tool—12 Items [iHOT‐12], Hip Outcome Score—Sports Specific Subscale [HOS‐SSS], Hip Outcome Score—Activities of Daily Living [HOS‐ADL], Hip disability and Osteoarthritis Outcome Score [HOOS], modified Harris Hip Score [mHHS] and Oxford Hip Score [OHS]), performed to assess consistency across instruments and support interpretation of the MCID‐based pooled outcomes rather than to provide independent comparisons.
Risk of bias assessment
Risk of bias was independently assessed by two reviewers (M. V. and A. L.) using Risk of Bias (RoB) 2 for randomized trials [64] and ROBINS‐I for non‐randomized studies [65], with adjudication by a third reviewer (N. R.). Publication bias was assessed using Begg's test [5] and funnel plot inspection [66].
Statistical analysis
Treatment effects were analysed using a frequentist multilevel random‐effects meta‐analysis with inverse variance weighting, restricted maximum likelihood estimation and Hartung–Knapp adjustment [56]. Continuous outcomes are reported as means with 95% confidence intervals (CIs). Subgroup analyses compared open versus endoscopic techniques, and heterogeneity was quantified using Higgins' I ^2^ statistic. All analyses were performed using the R packages meta and metafor.
RESULTS
Systematic literature search
A total of 503 records were screened by title and abstract after removal of 1020 duplicates, with high inter‐reviewer agreement (κ = 0.98). Forty‐seven full‐text articles [3, 4, 6, 8, 9, 10, 12, 14, 15, 16, 17, 18, 19, 21, 23, 24, 27, 28, 31, 32, 35, 36, 37, 38, 39, 40, 41, 42, 44, 45, 46, 48, 50, 51, 52, 53, 54, 58, 59, 61, 62, 67, 68, 69, 71, 72, 73] were assessed for eligibility with full agreement (κ = 1.0). Thirteen studies were excluded because treatment groups could not be differentiated [8, 9, 23, 39, 40, 61, 71], relevant outcomes were not reported [14, 21] or only long‐term outcomes were available [35, 48, 50, 54].
Ultimately, 34 primary studies [3, 4, 6, 10, 12, 15, 16, 17, 18, 19, 24, 27, 28, 31, 32, 36, 37, 38, 41, 42, 44, 45, 46, 51, 52, 53, 58, 59, 62, 67, 68, 69, 72, 73] including 1278 patients (1283 hips) were included in the multilevel meta‐analysis (Figure 1).
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta‐Analyses.
Patient characteristics
The open repair group included 14 studies [3, 10, 15, 17, 24, 31, 36, 37, 38, 52, 53, 59, 62, 73] with 490 patients (491 hips), 6.3% male, mean age 54.2 years and mean body mass index (BMI) 28.7 kg/m^2^.
The endoscopic group comprised 23 studies [4, 6, 12, 16, 18, 19, 24, 27, 28, 32, 37, 38, 41, 42, 44, 45, 46, 51, 58, 67, 68, 69, 72] with 788 patients (792 hips), 9.6% male, mean age 57.7 years and mean BMI 27.3 kg/m^2^.
Further study and patient details are summarized in Table 1. Preoperative PROMs did not differ significantly between groups (Figures [Link], [Link], [Link], [Link], [Link], [Link], [Link], [Link], Table S4).
Quality assessment
Among the 34 included studies, five showed moderate risk of bias [27, 32, 42, 44, 51], whereas 29 were rated as serious risk of bias [3, 4, 6, 10, 12, 15, 16, 17, 18, 19, 24, 28, 31, 36, 37, 38, 41, 45, 46, 52, 53, 58, 59, 62, 67, 68, 69, 72, 73] (Table 2). Funnel plots indicated variable publication bias. Minimal asymmetry was observed for postoperative functional MCID (Figure S9) and pain MCID (Figure S11), little bias for change in functional MCID (Figure S10), moderate asymmetry for change in pain MCID (Figure S12) and pronounced asymmetry for complications, suggesting relevant publication bias (Figure S13).
Multilevel meta‐analysis of primary outcomes
Postoperative functional MCID
Data from 1005 patients from 27 primary studies [3, 4, 6, 10, 15, 16, 17, 18, 24, 27, 28, 31, 32, 36, 37, 38, 41, 42, 44, 45, 46, 51, 53, 59, 62, 67, 72] were pooled (Figure 2, Table S4), with the open surgery group consisting of 398 patients from 12 primary studies [3, 10, 15, 17, 24, 31, 36, 37, 38, 53, 59, 62] and the endoscopic surgery group consisting of 607 patients from 18 primary studies [4, 6, 16, 18, 24, 27, 28, 32, 37, 38, 39, 42, 44, 45, 46, 51, 67, 72]. The mean postoperative functional MCID of the entire patient group was 9.01 points (mean: 9.01; CIs: 8.11–9.91; I ^2^ = 100%; τ ^2^ = 5.2; p = 0.00). The mean postoperative functional MCID of the open surgery group was 9.09 points (mean: 9.09; CIs: 8.12–10.06; I ^2^ = 99%; τ ^2^ = 5.4; p = 0.00). The mean postoperative functional MCID of the endoscopic surgery group was 8.96 points (mean: 8.96; CIs: 8.02–9.90; I ^2^ = 99%; τ ^2^ = 5.4; p = 0.00). The test for subgroup differences showed no statistically significant differences in postoperative functional MCID between the open surgery group and the endoscopic surgery group (F = 0.24; df = 1.0; p = 0.63).
Forest plot of the postoperative functional MCID. CI, confidence interval; MCID, minimal clinically important difference; SD, standard deviation.
Change in functional MCID
Data from 718 patients from 21 primary studies [3, 4, 10, 15, 16, 17, 18, 27, 28, 31, 32, 36, 41, 42, 45, 46, 51, 53, 59, 62, 67] were pooled (Figure 3, Table S4), with the open surgery group consisting of 290 patients from 9 primary studies [3, 10, 15, 17, 31, 36, 53, 59, 62] and the endoscopic surgery group consisting of 428 patients from 12 primary studies [4, 16, 18, 27, 28, 32, 41, 42, 45, 46, 51, 67]. The mean change in functional MCID of the entire patient group was 3.33 points (mean: 3.33; CIs: 2.86–3.81; I ^2^ = 83%; τ ^2^ = 0.9; p < 0.01). The mean change in functional MCID of the open surgery group was 3.10 points (mean: 3.10; CIs: 2.39–3.81; I ^2^ = 88%; τ ^2^ = 0.9; p < 0.01). The mean change in functional MCID of the endoscopic surgery group was 3.52 points (mean: 3.52; CIs: 2.89–4.15; I ^2^ = 63%; τ ^2^ = 0.9; p < 0.01). The test for subgroup differences showed no statistically significant differences in change in functional MCID between the open surgery group and the endoscopic surgery group (F = 0.86; df = 1.0; p = 0.36).
Forest plot of the change in functional MCID. CI, confidence interval; MCID, minimal clinically important difference; SD, standard deviation.
Postoperative pain MCID
Data from 867 patients from 20 primary studies [3, 4, 6, 10, 16, 17, 18, 24, 27, 31, 32, 36, 41, 42, 44, 46, 51, 52, 53, 59] were pooled (Figure 4, Table S4), with the open surgery group consisting of 349 patients from 9 primary studies [3, 10, 17, 24, 31, 36, 52, 53, 59] and the endoscopic surgery group consisting of 518 patients from 12 primary studies [4, 6, 16, 18, 24, 27, 32, 41, 42, 44, 46, 51]. The mean postoperative pain MCID of the entire patient group was 1.71 points (mean: 1.71; CIs: 1.27–2.16; I ^2^ = 98%; τ ^2^ = 0.9; p < 0.01). The mean postoperative pain MCID of the open surgery group was 1.58 points (mean: 1.58; CIs: 1.03–2.13; I ^2^ = 99%; τ ^2^ = 0.9; p < 0.01). The mean postoperative pain MCID of the endoscopic surgery group was 1.81 points (mean: 1.81; CIs: 1.31–2.32; I ^2^ = 87%; τ ^2^ = 0.9; p < 0.01). The test for subgroup differences showed no statistically significant differences in postoperative pain MCID between the open surgery group and the endoscopic surgery group (F = 0.80; df = 1.0; p = 0.38).
Forest plot of the postoperative pain MCID. CI, confidence interval; MCID, minimal clinically important difference; SD, standard deviation.
Change in pain MCID
Data from 798 patients from 20 primary studies [3, 4, 6, 10, 16, 17, 18, 24, 27, 31, 32, 36, 41, 42, 44, 46, 51, 52, 53, 59] were pooled (Figure 5, Table S4), with the open surgery group consisting of 349 patients from 9 primary studies [3, 10, 17, 24, 31, 36, 52, 53, 59] and the endoscopic surgery group consisting of 449 patients from 11 primary studies [4, 6, 16, 18, 27, 32, 41, 42, 44, 46, 51]. The mean change in pain MCID of the entire patient group was −1.99 points (mean: −1.99; CIs: −2.74 to −1.24; I ^2^ = 99%; τ ^2^ = 2.5; p = 0.00). The mean change in pain MCID of the open surgery group was −1.82 points (mean: −1.82; CIs: −2.96 to −0.69; I ^2^ = 100%; τ ^2^ = 2.6; p = 0.00). The mean change in pain MCID of the endoscopic surgery group was −2.12 points (mean: −2.12; CIs: −3.18 to −1.09; I ^2^ = 74%; τ ^2^ = 2.6; p < 0.01). The test for subgroup differences showed no statistically significant differences in change in pain MCID between the open surgery group and the endoscopic surgery group (F = 0.17; df = 1.0; p = 0.68).
Forest plot of the change in pain MCID. CI, confidence interval; MCID, minimal clinically important difference; SD, standard deviation.
Overall complications
Data from 804 patients from 25 primary studies [3, 4, 10, 12, 15, 16, 18, 19, 27, 28, 31, 36, 37, 38, 41, 44, 45, 52, 53, 59, 67, 68, 69, 72, 73] were pooled (Figure 6, Table S4), with the open surgery group consisting of 371 patients from 9 primary studies [3, 10, 15, 31, 36, 37, 38, 52, 53, 73] and the endoscopic surgery group consisting of 433 patients from 16 primary studies [4, 12, 16, 18, 19, 27, 28, 38, 41, 44, 45, 58, 67, 68, 69, 72]. The pooled proportion of overall complications for the entire patient group was 0.07 (95% CI: 0.05–0.11, I ^2^ = 53%, τ ^2^ = 0.8; p < 0.01), corresponding to a crude event rate of 58/804. For the open surgery group, the pooled proportion of overall complications was 0.08 (95% CI: 0.04–0.16, I ^2^ = 71%, τ ^2^ = 0.8; p < 0.01), with a crude event rate of 33/371 (0.09). For the endoscopic surgery group, the pooled proportion of overall complications was 0.07 (95% CI: 0.04–0.12, I ^2^ = 33%, τ ^2^ = 0.8; p = 0.07), with a crude event rate of 25/433 (0.06). The test for subgroup differences showed no statistically significant differences in overall complications between the open surgery group and the endoscopic surgery group (F = 0.16; df = 1.0; p = 0.70).
Forest plot of the overall complications. CI, confidence interval.
Multilevel meta‐analysis of secondary outcomes
The postoperative PROMs iHOT‐12, HOS‐SSS, HOS‐ADL and HOOS, and the change in mHHS, iHOT‐12, HOS‐SSS, HOS‐ADL and OHS showed no statistically significant differences between the open surgery group and the endoscopic surgery group (Figures [Link], [Link], [Link], [Link], [Link], [Link], [Link], [Link], [Link]). The funnel plots of primary and secondary outcomes are presented in Figures [Link], [Link], [Link], [Link], [Link], [Link], [Link], [Link], [Link], [Link].
DISCUSSION
The most important finding of the present study was that both open and endoscopic gluteal tendon repair result in clinically meaningful improvements in function and pain, with no relevant differences in efficacy between techniques. However, endoscopic repair was associated with lower complication rates and may therefore be preferred in most clinical scenarios when arthroscopic expertise is available. These findings have direct clinical implications, suggesting that surgical approach selection should be guided primarily by invasiveness and complication risk rather than expectations of superior functional recovery. In contrast to earlier descriptive reviews based on limited patient numbers [13], the present study provides a quantitative synthesis of a substantially larger evidence base using MCID‐based interpretation, offering clinically meaningful guidance for decision‐making.
The central distinction between open and endoscopic repair appears to relate to safety rather than efficacy. Both techniques achieved clinically relevant improvements in patient‐reported outcomes, underscoring that gluteal tendon repair itself effectively addresses pain and dysfunction. The open approach showed a non‐significant trend toward higher adverse event rates, particularly wound‐related complications, infections and postoperative haematomas, which may negatively affect recovery, increase healthcare utilization and reduce patient satisfaction.
The consistency of functional and pain improvements across both groups suggests that the pathophysiological target—tendon reattachment—is adequately addressed by either technique. The primary differentiator is therefore the extent of surgical exposure. Endoscopic repair minimizes soft tissue trauma and preserves vascularity, which may partly explain the lower complication rates, an important consideration in the typically older, predominantly female patient population with higher comorbidity burden.
The findings of this multilevel meta‐analysis align with prior systematic reviews [13, 33], which similarly reported equivalent functional outcomes but a more favourable complication profile for endoscopic repair. Longstaffe et al. [33] and Chandrasekaran et al. [13] reported low and comparable retear rates (approximately 3%–4%), reinforcing that structural healing is not substantially technique‐dependent. More recent cohort studies [36, 43] further support these observations, demonstrating sustained improvements in strength, gait and patient satisfaction.
By pooling a substantially larger dataset and applying a multilevel meta‐analytic framework, the present study extends prior work with greater statistical precision. MCID‐based normalization allowed harmonization of heterogeneous PROM instruments, addressing a major limitation of earlier analyses. Funnel plot asymmetry—particularly for complications—suggests possible publication bias, but the overall pattern consistently indicates higher morbidity without superior efficacy after open repair.
From a clinical standpoint, both techniques remain valid options for gluteal tendon tears, with endoscopic repair favoured when technically feasible. Reduced complication rates may translate into shorter hospital stays, fewer reoperations and lower overall costs. However, endoscopic repair is technically demanding, may require longer operative time and depends on arthroscopic expertise, particularly during the learning curve.
Open repair retains an important role in complex scenarios, including massive or retracted tears, poor tissue quality or when concomitant procedures necessitate open exposure. Surgical decision‐making should therefore remain individualized, incorporating tear characteristics, patient comorbidities and surgeon experience. Shared decision‐making is essential, as patients can be counselled that functional outcomes are comparable, while perioperative risk profiles differ.
This study has several limitations. The evidence base consists predominantly of retrospective case series (Level IV), with few prospective or comparative studies and no RCTs. Heterogeneity in patient selection, concomitant procedures and rehabilitation protocols may have influenced outcomes. Despite MCID‐based standardization, residual bias from pooling heterogeneous PROMs cannot be excluded. Importantly, tear size, tear pattern, and tissue quality were inconsistently reported, introducing potential selection bias, as larger or more complex tears may be preferentially treated with open repair. The absence of non‐operative comparator studies further limits contextualization of surgical outcomes. Finally, the predominance of studies with serious risk of bias [3, 4, 6, 10, 12, 15, 16, 17, 18, 19, 24, 28, 31, 36, 37, 38, 41, 45, 46, 52, 53, 58, 59, 62, 67, 68, 69, 72, 73] and evidence of publication bias—particularly for complications—necessitate cautious interpretation.
In daily clinical practice, these findings support informed surgical counselling. When both approaches are feasible, endoscopic repair may be preferred due to lower complication risk without sacrificing functional recovery or pain relief, while open repair remains appropriate for complex tear patterns or compromised tissue quality.
CONCLUSION
Open and endoscopic gluteal tendon repair provide clinically meaningful short‐term improvements in function and pain, with no relevant differences in efficacy. Endoscopic repair is associated with lower complication rates and may be considered when arthroscopic expertise is available. This multilevel meta‐analysis adds quantitative evidence from a larger dataset using multilevel modelling and MCID‐based interpretation, offering clearer guidance for clinical decision‐making.
AUTHOR CONTRIBUTIONS
Nikolai Ramadanov, Maximilian Voss and Ariana Lott performed the literature search, the data extraction and the risk of bias assessment. Robert Hable and Nikolai Ramadanov conducted the statistical calculations. Robert Hable and Nikolai Ramadanov created all figures and tables. Nikolai Ramadanov wrote the manuscript. Ingo J. Banke, Robert Prill, Plamen Penchev, Marko Ostojic and Roland Becker supervised the work.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
Ethics approval was not required as this study is a multilevel meta‐analysis of previously published primary studies.
Supporting information
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
Supporting information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agha RA , Mathew G , Rashid R , Kerwan A , Al‐Jabir A , Sohrabi C , et al.; TITAN Group . Transparency in the reporting of artificial intelligence—the TITAN guideline. Premier J Sci. 2025;10:100082.
- 2Alpaugh K , Chilelli BJ , Xu S , Martin SD . Outcomes after primary open or endoscopic abductor tendon repair in the hip: a systematic review of the literature. Arthroscopy. 2015;31(3):530–540.25442666 10.1016/j.arthro.2014.09.001 · doi ↗ · pubmed ↗
- 3Barrera M , Bothorel H , Poultsides L , Christofilopoulos P . Short‐term outcomes following mini‐open repair of chronic gluteus medius tendon tears using a double‐row technique. J Hip Preserv Surg. 2021;8(2):202–208.35145719 10.1093/jhps/hnab 060PMC 8825688 · doi ↗ · pubmed ↗
- 4Bauwens PH , Haidar I , Thaunat M . Endoscopic transfer of gluteus maximus and tensor fasciae latae for massive gluteus medius tear: preliminary results. Orthop Traumatol Surg Res. 2021;107(8):102927. 10.1016/j.otsr.2021.102927 33845176 · doi ↗ · pubmed ↗
- 5Begg CB , Mazumdar M . Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–1101.7786990 · pubmed ↗
- 6Bitar AC , Guimarães JB , Marques R , de Castro Trindade CA , Filho AGO , Nico MAC , et al. Clinical and radiological results after endoscopic treatment for gluteal tendon injuries with a minimum follow‐up of 12 months. Arch Bone Joint Surg. 2023;11(10):641–648.37873531 10.22038/ABJS.2023.70495.3304 PMC 10590485 · doi ↗ · pubmed ↗
- 7Brethouwer DA , Brown ML , Mc Cauley JC , Bugbee WD , Chang EY , Lombardi AF , et al. What is the prevalence of hip abductor pathology in patients undergoing total hip arthroplasty? Arthroplast Today. 2024;31:101601. 10.1016/j.artd.2024.101601 39811777 PMC 11732240 · doi ↗ · pubmed ↗
- 8Browning RB , Fenn TW , Allahabadi S , Rice MW , Swindell HW , Ebersole JW , et al. Three‐grade magnetic resonance imaging‐based gluteus medius and/or minimus tear classification system provides excellent inter‐rater reliability. Arthrosc Sports Med Rehabil. 2023;5(3):e 773–e 782.37388882 10.1016/j.asmr.2023.04.004PMC 10300604 · doi ↗ · pubmed ↗