Mental health risks and support for frontline workers during the 2013–2016 Ebola outbreak
Ira Chaturvedi, Andrew S. Huang, Amy Luo, Alexander H. Chang, J. Lee Jenkins, Edbert B. Hsu

TL;DR
This study examines mental health challenges faced by frontline workers during the 2013–2016 Ebola outbreak and highlights the need for better support and interventions.
Contribution
The paper provides a comprehensive scoping review of mental health and well-being dimensions and interventions for frontline workers during the Ebola outbreak.
Findings
Frontline workers experienced significant stress, anxiety, social isolation, fear, and guilt during the Ebola outbreak.
Few studies have addressed mental health interventions for frontline workers, emphasizing a gap in research and practice.
Recommendations for psychological support and education resources were identified at multiple levels.
Abstract
The 2013–2016 West African Ebola virus outbreak was the longest and largest Ebola outbreak to date. High levels of stress and isolation experienced by frontline workers (FWs) during the Ebola outbreak highlight the importance of recognizing mental health and well-being (MHW). This study aimed to summarize and synthesize the MHW dimensions and interventions among FWs during the Ebola outbreak. A scoping review was conducted for English- and French-language articles indexed in PubMed and the Global Health Library, published from 2013 up to March 2025. Quantitative and qualitative studies reporting on the epidemiology and interventions for MHW among FWs, including healthcare personnel and ancillary health staff, during the Ebola outbreak were eligible for inclusion. A total of 22 articles were included in this review. Of these, 14 articles addressed the epidemiology of MHW for FWs, 3…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1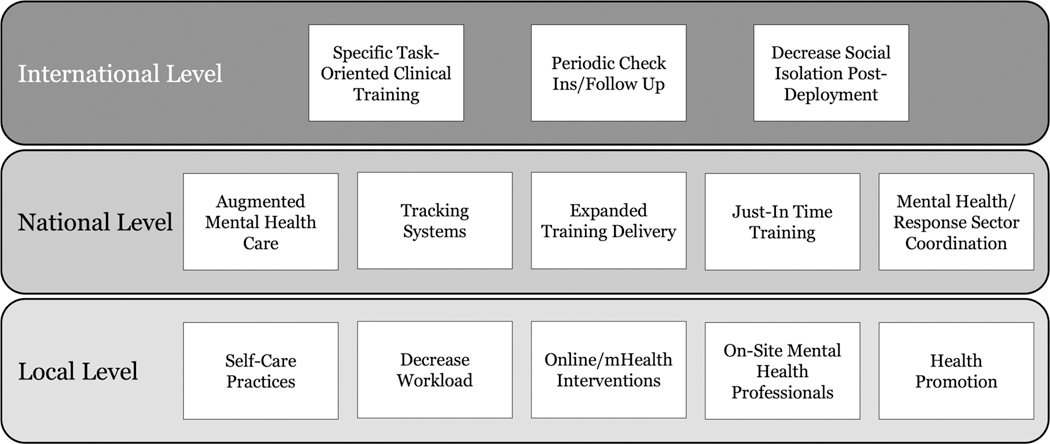 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDisaster Response and Management · Viral Infections and Outbreaks Research · COVID-19 and Mental Health
Introduction
Infectious disease outbreaks place markedly increased demands on healthcare systems and personnel. Frontline workers (FWs), including both medical and nonmedical support staff, must deal with challenging work environments, resource constraints, staffing shortages, and increased workloads. In addition, FWs face increased risks of infection through close patient contact and must often adapt to new infection control protocols and unfamiliar practices. For FWs, fears of becoming infected and of the unknown are among the most pressing psychosocial challenges [1]. In responding to infectious outbreaks, FWs experience a daunting combination of stressors that can profoundly affect their mental health and well-being (MHW) [2].
The 2013–2016 West African Ebola virus outbreak was the longest and largest Ebola outbreak to date, as well as the first to spread beyond Central or Eastern Africa [3]. Following the index case in a remote village in Guinea in December 2013, the outbreak spread rapidly throughout the country and to densely populated urban areas in neighboring Sierra Leone and Liberia by mid-2014. During this outbreak, Ebola involved seven more countries in Africa, Europe, and North America. At the end of the outbreak, 28,652 infections and approximately 11,325 deaths in the ten countries were recorded [4]. The adjusted case fatality rates in the three countries at the epicenter of the outbreak rose above 80 percent [5].
FWs were essential to the 2013–2016 West Africa Ebola outbreak response. At the peak of the outbreak, many international organizations sent aid to local healthcare workers in West Africa, with the CDC deploying approximately 1,450 CDC responders to Guinea, Liberia, and Sierra Leone [6]. Additionally, 24,655 medical FWs in West Africa were trained in infection prevention and control practices [7]. Nevertheless, constant exposure from working in Ebola Treatment Units (ETUs) resulted in a 20 to 30 times higher likelihood of infection of FWs compared to the general adult population [8]. Mortality rates among medical FWs were much higher than those of the general population; while mortality rates in Guinea, Sierra Leone, and Liberia were 0.02%, 0.06%, and 0.11%, respectively, medical FW fatality rates were 1.45%, 6.85%, and 8.07%, respectively [9].
As a cornerstone of any infectious outbreak response, FWs will be subject to the short- and long-term mental health impacts of a wide variety of psychological stressors and traumas [10]. Understanding how this impacts the mental health and well-being of FWs is essential to supporting and protecting the workforce [11]. The scope of MHW interventions for FWs during the 2013–2016 West Africa Ebola outbreak has not been comprehensively examined to date. Of note, this may have implications for ways in which the MHW of FWs in other infectious outbreaks in low-resource settings might be addressed. This scoping review aimed to (1) synthesize the epidemiological patterns and key dimensions of MHW and (2) characterize interventions implemented to address MHW among frontline workers during the Ebola outbreak. We contextualize the stressors faced by FWs during the Ebola outbreak and stratify the identified interventions according to local, national, and international levels.
Materials and methods
We conducted a scoping review of English- and French-language articles indexed in PubMed and the Global Health Library published between December 2013 and 19 March 2025. This period covers the entire span of the 2013–2016 West Africa Ebola outbreak, including its World Health Organization (WHO) declaration as a Public Health Emergency of International Concern (PHEIC) on 8 August 2014.
Search strategy and selection process
2.1.
Peer-reviewed literature search strategies were developed by the team with a university informationist. The complete search strategies are detailed in Supplementary materials, incorporating PubMed and the Global Health Library for peer-reviewed English- and French-based articles. Duplicates were removed. The results were imported into Covidence (Veritas Health Innovation, Melbourne, Australia), and additional identified duplicates were removed.
During the screening of the title and abstract, articles were required to (1) pertain to FWs; (2) relate to the period during the Ebola outbreak; and (3) include the terms, stress, sleep, mental health, resilience, or wellness. When screening the full text, the inclusion criteria included a description pertaining to epidemiology or intervention or proposed intervention for FWs. Exclusion criteria were applied to articles not describing FW MHW epidemiology or interventions pertaining to FW MHW during the Ebola outbreak. Two members of the team independently assessed each citation. Studies were included only if two reviewers agreed that the studies contained original quantitative or qualitative data addressing one or more of the key questions. In cases of initial disagreement between reviewers regarding the inclusion of a study, it was reviewed by the team to reach a consensus and make a final determination. The inclusion criteria required the article to (1) address one of the key questions. The exclusion criteria were studies (1) not written in English or French; (2) not pertaining to the target population; (3) not related to the topics; (4) not pertaining to the specified time frame; and (5) including no original data (e.g., editorial, commentary, or review articles). For each study that met the inclusion criteria, a team member used Covidence to extract pre-determined information about the characteristics and context of the studies. A second member of the team reviewed the extracted information for accuracy. The extracted information was organized into tables.
Data extraction and synthesis
2.2.
A PICOTS (population, intervention, comparator, outcomes, timing, setting) typology was developed to guide the scoping review. The population included FWs composed of both medical (e.g., healthcare workers) and nonmedical (e.g., ancillary and support staff) personnel who worked in response to Ebola. Interventions included any interventions or proposed interventions focused on addressing stress and wellness in FWs. Comparators consisted of FWs not working to respond to the Ebola outbreak during the same period. Outcomes included reduced stress or enhanced wellness following an intervention. Timing spanned from 2013 to 2016 during the Ebola outbreak. Setting included any location where FWs encountered those with Ebola virus disease. The findings were narratively synthesized in accordance with the established narrative analysis methods [12].
Results
Study identification and inclusion
3.1.
After removing duplicates, a total of 186 records were retrieved (Figure 1). Following the screening of the title and abstract, we retrieved 39 full-text reports for eligibility. Among these, 1 report was unable to be retrieved and 16 full-text reports were excluded due to wrong article type (e.g., editorial, commentary, or reviews), topic (e.g., unrelated to MHW), or population (e.g., Ebola patients or survivors). The final review included 22 articles.
Characteristics of included studies
3.2.
The characteristics of the included studies are summarized in Table 1. Among the 22 articles that met the inclusion criteria, 14 (64%) characterized the epidemiology of MHW among FWs in response to the Ebola outbreak, 3 (14%) described interventions implemented to address stress and wellness among FWs, and 5 (23%) included both. Ten (45%) studies were conducted in Sierra Leone, two (9%) studies were conducted in Liberia, one (5%) study was conducted in Guinea, five (23%) studies were conducted in multiple countries in West Africa, two (9%) studies were conducted in Nigeria, two (9%) studies were conducted in Germany, and one (5%) study was conducted in the United States of America (USA). The study populations included local and deployed FWs, including physicians, nurses, medical students, community health workers, auxiliary staff (e.g., hygienists, laboratory technicians), and facility management or leadership members. Among the included studies, 10 (45%) were in-depth interviews, 6 (27%) were cross-sectional, 5 (23%) were case studies, and 2 (9%) were pre-/post-test designs. All studies but one were written in English.
Epidemiological patterns and key dimensions among FWs
3.3.
Of the twenty-two articles included in this study, nineteen examined the epidemiology of mental health and related morbidities in various FW subpopulations during the 2013–2016 Ebola outbreak [13–30]. These studies used qualitative methods such as interviews or questionnaires to characterize the mental toll on the workforce when responding to the outbreak [15, 21, 22, 24, 25, 27–30]. It was noted that during the Ebola outbreak, mental and psychosocial problems increased, especially in countries at the epicenter of the outbreak, such as Sierra Leone. Some common themes that originated from the literature suggested that FWs felt an increased sense of isolation, moral strain, and psychological distress. Interestingly, while these themes were noted to be present in FWs responding to the Ebola 2013–2016 outbreak, the role of being an HCW was protective to one’s mental health as compared to other Ebola survivors [19, 23].
Social isolation
3.3.1.
A recurring theme seen throughout the literature was the sense of isolation that the FWs faced. Compared to medical and research staff not working in ETUs, FWs working in ETUs experienced significantly higher levels of social isolation [13, 15–17, 22, 25, 27, 28, 30]. A factor that increased HCW isolation was the stigma around treating Ebola [13, 15, 27, 28, 30]. Stigma around Ebola extended beyond regional communities at the epicenter of the outbreak, such as Sierra Leone, and was also evident in countries that provided international aid or treated patients, such as the United Kingdom and the United States of America [15, 16, 20, 21, 29, 31, 32]. In addition to community stigma, many FWs feared contagion when working in ETUs, resulting in self-distancing from peers [29, 30]. This fear of contagion extended to households, local communities, and patients, which not only strained and disrupted the interpersonal relationships of FWs but also contributed to feelings of isolation [17, 20, 27, 29, 30].
Moral strain
3.3.2.
Another theme was the ethical burden placed on FWs when treating Ebola patients. FWs recall their personal experiences in ETUs and the moral distress that they felt when prioritizing a public health containment approach rather than adopting a patient-centric approach [18, 21]. Moral distress resulted when individuals could not take an action they believed to be ethically correct or were uncertain of what the ethical action was [33]. This distress, in contrast to other forms of distress, threatens one’s core values and has broadly reaching ethical consequences. The alternate standard of care received by patients in ETUs often triggered this distress among FWs during the Ebola outbreak [15].
Psychological distress
3.3.3.
The most prevalent theme was the mental health toll faced by FWs in responding to the outbreak. Although various factors can contribute to psychological distress, working in ETUs accounted for significantly higher psychological stress compared to not working in ETUs, with one study showing working in biocontainment units to be more stressful than daily tasks for 60% of respondents [20, 29]. The specific profession of the staff was a determinant of the level of mental burden on FWs. For example, one study showed that medical FWs in Sierra Leone, such as male medics and medical staff who were responsible for cleaning and disinfecting ETUs, had higher scores for OCD, anxiety, phobic anxiety, interpersonal sensitivity, paranoid ideation, and positive symptoms [7]. Positive symptoms accounted for the number of self-reported symptoms of psychopathology respondents experienced. However, this study also noted that FWs with prior experience working in highly stressful medical situations did not view working in ETUs to be as stressful as those lacking similar prior experience, and very serious concerns lessened as measures to address mental health were implemented.
It was also noted that FWs displayed high levels of psychological distress, depression, anxiety, sadness, and prolonged stress [15–17, 22–24, 27, 30]. While there was direct psychological distress due to directly engaging with the Ebola outbreak, FWs also faced higher levels of anxiety, in some cases, due to social and political unrest in the region [17]. Additionally, HCWs also showed increased fear of infection and death, contributing to heightened stress levels in this population [17, 27, 30]. Many FWs also discussed ways in which under-resourced settings were described by some as “a real horror show” [15]. Limited medical resources, PPE, and medical staff demanded long hours for staff, eventually leading to fatigue and depersonalization.
Interventions addressing MHW among FWs
3.4.
Of the twenty-two articles extracted, eight discussed and/or tested interventions that addressed stress and/or wellness in FWs [14, 27–32, 34]. Many FWs felt that the culmination of various factors previously described led to increased levels of stress and psychological burden, necessitating specific interventions. Strengthening current mental health resources for FWs with the use of mental health specialists to provide requisite psychosocial support or implement cognitive behavioral therapy for FWs was suggested [14, 34]. Studies showed that these mental health resources were used by many of the FWs in ETUs [29]. Studies recommended psychosocial coping methods and other resources for stress management to be offered to FWs [14, 27, 34]. One study incorporated a team of non-specialist nurses who were trained in mental health awareness to support their wards [14]. This training of nurses proved successful in ensuring mental health support for HCWs during the outbreak. Other studies suggested a need for change in the work environment of HCWs, reducing the length of workers’ shifts and placing a larger emphasis on supporting FWs through various services [16]. These interventions should be considered for not only FWs directly working in ETUs but for all FWs. The effectiveness of mobile health (mHealth) interventions in supporting mental health in FWs by helping FWs identify trauma stressors and self-triage was mentioned [32]. Furthermore, in addition to individual-based interventions, studies showed that the inclusion of pre-, peri-, and post-deployment trainings and briefings for international HCWs increased the level of preparedness HCWs felt before working at ETUs and aided in navigating the stressors they faced [25, 31, 32].
Discussion
This scoping review explored the epidemiology and interventions addressing mental health and wellness pertaining to FWs during the 2013–2016 Ebola outbreak. Exhaustion from long hours in resource-limited settings was commonplace during the outbreak. Local FWs were not the only ones impacted. Many international organizations deployed HCWs who cared for those with EVD, risking their own personal and mental health. Among a total of twenty-two articles, fourteen articles addressed the epidemiology of mental health and wellness among FWs, three articles described interventions for mental health and wellness among FWs, and five articles discussed both epidemiology and interventions in the context of the Ebola outbreak. Along with dealing with workplace stressors, FWs contended with social stressors from their families and their communities. FWs experienced significant social isolation due to the fear and stigma throughout the outbreak to a much greater degree than colleagues who were not in direct contact with Ebola patients. While working in ETUs, many workers dealt with isolation, depression, stigmatization, interpersonal stress, and extreme stress. FWs were required to isolate and quarantine upon leaving the ETU. Additionally, many who worked in ETUs were excluded from social events even after quarantining. The stigma of contracting Ebola continued to impact those at times even following recovery.
These high levels of stress and isolation experienced by FWs working during the Ebola outbreak increased the risks of experiencing mental health issues and led to a high demand for mental health interventions [31, 32, 34, 35]. Although the WHO Mental Gap Action Program (mhGAP) outlined recommendations, countries affected by Ebola lacked mental health and psychosocial support (MHPSS) programs, trained mental health professionals, or the resources to implement these programs [36]. For instance, Liberia and Sierra Leone have a dearth of psychologically trained staff, each with just a single trained psychiatrist, a few dozen mental health nurses, and roughly a thousand trained paraprofessionals trained to assess and manage common mental disorders [23, 37]. The lack of trained personnel amplified the risks of psychological distress and psychopathology [38]. Mental health interventions for the general population were generally implemented with the aid of international organizations, many late into the Ebola outbreak [39, 40].
Several limitations are noted. Although the search strategies were designed to be comprehensive in identifying FWs, including both medical and nonmedical personnel during the Ebola outbreak, other alternate designations of FWs may not have been captured. Studies that did not delineate FW groups were not included given the difficulty of ascertaining the specific impact on FWs. Heterogeneity and limitations of design and outcome measures often limited the comparability of the identified studies. The relative scarcity of the studies which addressed interventions highlights the challenges of conducting intervention-based studies in the most-impacted countries and suggests directions for future research. Recommendations for future mental health interventions encompassing a whole-systems approach at the local, national, and international levels are discussed.
Local-level interventions
4.1.
Locally, the importance of interventions to directly reduce mental health burdens on FWs cannot be overstated. At the hospital level, one strategy to reduce mental distress of FWs is to decrease shift hours and direct patient interaction time [16, 22]. Various ways to optimize shift loads have been proposed [22]. Balancing shift loads with the increased demand for patient care is a fundamental operational dilemma during outbreaks.
Providing staff with early psychosocial support and strategies for coping with high-stress situations may serve to reduce mental distress among FWs and deploying such interventions as soon as possible is critical [7]. One way to achieve this is through workshops on mental health for FWs. Research shows that the implementation of workshops focused on teaching psychological first aid and coping strategies helps FWs feel more confident not only in being able to access psychosocial support but also in their ability to treat patients [14, 27, 34]. Coping strategies such as using physical protection; practicing self-confidence and pragmatism; and engaging in self-care, peer-support networks, social media platforms, wellness activities, and religion have been shown to reduce mental health burden on FWs [24, 25, 27, 30]. During the COVID-19 pandemic, practicing self-care was an effective intervention for FWs to balance their personal needs with those of their patients [41]. While this requires dedicated time, interventions can be implemented during work shifts, providing FWs with strategies and skills to cope with high levels of stress, burnout, and other mental health issues.
Offering FWs access to psychological support using online and mobile Health (mHealth) platforms that enable them to track their moods, achieve goals, and learn micro-practices can mitigate the psychological burden on FWs [32, 37, 42]. It has been shown that mHealth models allow FWs to tap into a successful self-triage system where they are able to identify traumatic stressors and follow a treatment plan to reduce stress.
Incorporating a full-time facility-based mental health practitioner will also reduce FWs’ mental health burden by providing real-time linkages to ongoing psychological care [43]. Though more costly than other interventions, a trained mental health practitioner able to discuss issues privately or in group settings was found to be useful by HCWs. The rapid identification of outbreak-associated psychological stressors, especially for high-risk groups, and the provision of effective coping strategies and resources were also in great demand wherever the 2013–2016 Ebola outbreak occurred. Finally, other types of adjunctive health interventions targeting FWs, such as acupuncture and acupressure, have proven to be successful in reducing anxiety, burnout, and secondary traumatic scores among FWs (Figure 2) [44, 45].
National-level interventions
4.2.
At the national level, government-sponsored funding and initiatives can also help alleviate the burden of outbreak response on FWs. For example, supplementing the salaries of FWs engaging in outbreak response acknowledges their elevated risk and workload while reducing financial stress [27]. Government agencies must prepare and work with other organizations to ensure that facilities not only have sufficient staff and supplies but also programs and structures in place to foster the mental health of FWs in response to an outbreak. Given the dearth of mental health professionals in regions impacted by the outbreak, efforts should be made to establish additional training programs to develop a skilled deployable cadre [46]. National authorities can also take the lead in the development of systems to track and assist FWs in managing burnout and stress and promote recognition of these impacts on the workforce. Some interventions, such as Community Resiliency Model (CRM) training, focused on body awareness, have proven to help reduce both immediate and long-term stress, with HCWs reporting improved mental well-being as well as decreased stress and somatic symptoms [47]. National organizations can work together to develop similar expanded platforms to provide FWs throughout the country with ready asynchronous access to resources to help cope with high-stress environments. Support at the national level for the development and delivery of training modules on working in stressful and resource-constrained environments could serve as an important preventative measure against burnout.
These measures can be developed and strengthened during normal operations to better address the mental health toll on FWs as part of a comprehensive behavioral health strategy. In the event of an outbreak, wide-scale just-in-time modules specific to the immediate threat, using online and mHealth interventions, may serve as effective, less-costly augmentation measures. As part of any outbreak response planning, the inclusion of mental health professionals pre-, during, and post-outbreak has been strongly recommended [22]. Careful coordination from the mental health and emergency response sectors is essential to identify resources and potential gaps in addressing the mental health needs of FWs to ensure that it is of the highest priority.
International-level interventions
4.3.
Given the ubiquitous nature of international assistance during outbreak response, systematic approaches to safeguard the mental health of deployed personnel must be taken into consideration. For international medical FWs responding to outbreaks in other countries, the need to improve mental and psychosocial support, especially during pre- and post-deployment, has been well recognized [26]. Including pre-deployment screenings and trainings can help improve response to mental distress by equipping HCWs with stress management tools such as Anticipate, Plan and Deter (APD) training [31, 32]. Additionally, specific task-oriented clinical training during the pre-deployment phase can aid mental preparation for the mission [21, 26]. Including peri-deployment support such as voluntary infield briefings allows HCWs to have the opportunity to share experiences and engage in social networks as well as reduce stress during their deployment [32]. Offering information about Ebola to friends, family, and colleagues back home may help decrease the social isolation of returning participants post-deployment [15, 26]. The post-deployment provision of psychological support to FWs upon their return, such as through periodic check-ins and follow-ups with a mental health specialist, has also been noted to be beneficial [24, 31].
Conclusions
This scoping review highlights the importance of social isolation, moral strain, and psychological distress impacting FWs as well as a relative scarcity of interventions addressing the mental and social stressors faced during the 2013–2016 Ebola outbreak. The findings suggest a significant demand for mental health intervention development and implementation as part of a comprehensive behavioral health response plan. MWH interventions supporting FWs should be actively explored. Recommendations can be incorporated into healthcare systems during routine operations as well as during outbreak responses to address the gaps in the mental health support of FWs.
Supplementary Material
Supplemental Materials
Supplementary materials are available at https://doi.org/10.20935/MHealthWellB7717.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cabarkapa S, Nadjidai SE, Murgier J, Ng CH. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: a rapid systematic review. Brain Behav Immun-Health. 2020;8:100144. doi: 10.1016/j.bbih.2020.10014432959031 PMC 7494453 · doi ↗ · pubmed ↗
- 2Xiong Y, Peng L. Focusing on health-care providers’ experiences in the COVID-19 crisis. Lancet Glob Health. 2020; 8:e 740–1. doi: 10.1016/S 2214-109X(20)30214-X 32573442 PMC 7190304 · doi ↗ · pubmed ↗
- 3Oleribe OO, Salako BL, Ka MM, Akpalu A, Mc Connochie M, Foster M, Ebola virus disease epidemic in West Africa: lessons learned and issues arising from West African countries. Clin Med. 2015;15:54–7. doi: 10.7861/clinmedicine.15-1-54 · doi ↗
- 4Forna A, Nouvellet P, Dorigatti I, Donnelly CA. Case fatality ratio estimates for the 2013–2016 West African ebola epidemic: application of boosted regression trees for imputation. Clin Infect Dis. 2020;70:2476–83. doi: 10.1093/cid/ciz 67831328221 PMC 7286386 · doi ↗ · pubmed ↗
- 5WHO Ebola Response Team. Ebola virus disease in West Africa—the first 9 months of the epidemic and forward projections. N Engl J Med. 2014;371:1481–95. doi: 10.1056/NE-J Moa 141110025244186 PMC 4235004 · doi ↗ · pubmed ↗
- 6Dahl BA. CDC’s response to the 2014–2016 ebola epidemic— guinea, liberia, and sierra leone. MMWR Suppl. 2016;65:12–20. doi: 10.15585/mmwr.su 6503 a 3 · doi ↗
- 7Li L, Wan C, Ding R, Liu Y, Chen J, Wu Z, Mental distress among Liberian medical staff working at the China Ebola Treatment Unit: a cross sectional study. Health Qual Life Outcomes. 2015;13:156. doi: 10.1186/s 12955-015-0341-226409446 PMC 4583730 · doi ↗ · pubmed ↗
- 8World Health Organization. Health worker Ebola infections in Guinea, Liberia and Sierra Leone: a preliminary report. Geneva: WHO; 2015.