Zoonotic Streptococcus canis Bacteremia Following a Dog Scratch in an Elderly Patient With a Nonconditional Pacemaker
Kamel Alachraf, Patrick Trouten, Jessica Thayer

TL;DR
An elderly woman with a pacemaker developed a rare infection from a dog scratch, highlighting the zoonotic potential of Streptococcus canis.
Contribution
This case report highlights S. canis as a zoonotic pathogen and emphasizes the importance of exposure history in diagnosing infections.
Findings
Streptococcus canis was identified as the cause of bacteremia following a dog scratch in an elderly patient with a pacemaker.
The patient showed clinical improvement with ceftriaxone treatment and no recurrence of infection.
Imaging and echocardiography ruled out metastatic infection or pacemaker involvement.
Abstract
Streptococcus canis is a β‐hemolytic Group G streptococcus commonly found in the microbiome of dogs and cats and is an uncommon cause of invasive human infection. Although typically regarded as a veterinary pathogen, S. canis has been reported to cause bacteremia, endocarditis, and other severe infections in humans, particularly in older adults with significant comorbidities or implanted medical devices. We describe a case of Streptococcus canis bacteremia in an 89‐year‐old woman with multiple comorbidities and a nonconditional permanent pacemaker who presented with fever, dyspnea, and severe lower back pain. Blood cultures grew S. canis, identified using standard microbiologic techniques. The clinical course raised concern for metastatic infection and pacemaker involvement. Imaging of the thoracic and lumbar spine demonstrated no evidence of discitis or osteomyelitis, and both…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
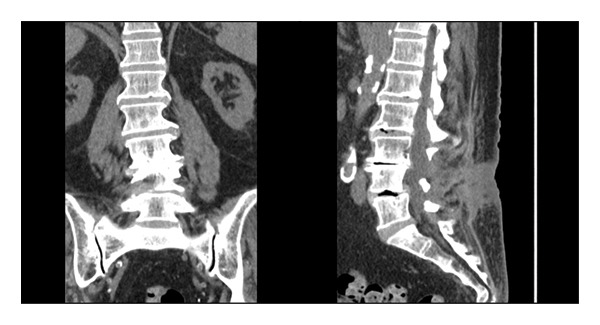 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2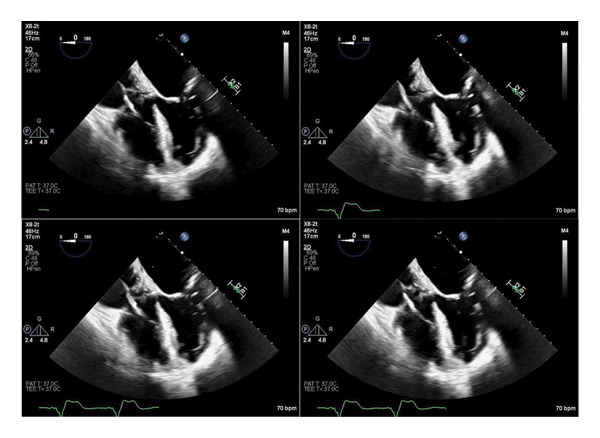 FIGURE 3
FIGURE 3| Hemoglobin | 10.6 g/dL | Low |
| MCV | 92.7 fL | Normal |
| WBC | 9.4 × 103/μL | Normal |
| Neutrophils | 6.59 × 103/μL | Normal |
| Sodium | 138 mmol/L | Normal |
| Potassium | 4.7 mmol/L | Normal |
| Chloride | 107 mmol/L | Normal |
| Bicarbonate | 26 mmol/L | Normal |
| Calcium | 8.5 mg/dL | Normal |
| Magnesium | 2.4 mg/dL | Normal |
| Bilirubin | 1.1 mg/dL | Normal |
| Glucose | 149 mg/dL | Elevated |
| Creatinine | 1.94 mg/dL | Elevated |
| AST | 53 U/L | Elevated |
| ALT | 42 U/L | Elevated |
| ALP | 74 U/L | Normal |
| Albumin | 3.4 g/dL | Normal |
| CRP | 118.5 mg/L | Elevated |
| AKI | Acute kidney injury |
| ALT | Alanine aminotransferase |
| ALP | Alkaline phosphatase |
| AST | Aspartate aminotransferase |
| BMP | Basic metabolic panel |
| CBC | Complete blood count |
| CKD | Chronic kidney disease |
| CRP | C‐reactive protein |
| CT | Computed tomography |
| EF | Ejection fraction |
| HFpEF | Heart failure with preserved ejection fraction |
| IV | Intravenous |
| LFTs | Liver function tests |
| MRI | Magnetic resonance imaging |
| OPAT | Outpatient parenteral antimicrobial therapy |
| SpO2 | Peripheral oxygen saturation |
| TEE | Transesophageal echocardiogram |
| TTE | Transthoracic echocardiogram |
| UA | Urinalysis |
| WBC | White blood cell count |
- —National Institutes of Health10.13039/100000002
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Rabies epidemiology and control · Cardiovascular Conditions and Treatments
1. Background
S. canis is the most frequently isolated streptococcus from dogs and cats. It is a β‐hemolytic, Group G (pyogenic) streptococcus that colonizes the skin, genital, and gastrointestinal tracts of healthy dogs and cats [1]. While S. canis is primarily considered a veterinary pathogen, it can occasionally cause invasive infections in humans, particularly in immunocompromised individuals or those with significant comorbidities or implanted medical devices. Reported human infections include bacteremia, cellulitis, necrotizing fasciitis, septic arthritis, and endocarditis, often in the context of zoonotic transmission [2].
2. Clinical Course
An 89‐year‐old female presented to the Emergency Department with a 4‐day history of fever, chills, shortness of breath, and general malaise, all of which had worsened over the preceding 24 h. She also reported lower back pain radiating to both legs. Her past medical history was significant for chronic kidney disease Stage IV, heart failure with preserved ejection fraction (HFpEF), atrial fibrillation, and a permanent pacemaker.
The patient’s initial vital signs were notable for a temperature of 38.6°C, blood pressure of 114/32 mmHg, heart rate of 70 bpm, respiratory rate of 19, and oxygen saturation of 94% on room air. The patient appeared ill and in distress, primarily due to right lower extremity and lower back pain. Integumentary exam revealed scattered bruising on the upper extremities, without signs of cellulitis or stigmata of endocarditis. Cardiac, pulmonary, abdominal, and neurologic examinations were unremarkable. However, the patient developed a new oxygen requirement of 2 L/min via nasal cannula the following morning.
Initial laboratory evaluation demonstrated anemia, acute kidney injury on chronic kidney disease, elevated transaminases, and a markedly elevated C‐reactive protein (Tables 1 and 2). Computed tomography of the chest, abdomen, and pelvis demonstrated subtle left lower lobe ground‐glass opacities. Urinalysis showed pyuria, though urine cultures were negative (Tables 1 and 2).
Empiric antimicrobial therapy with doxycycline and ceftriaxone was initiated. Urinary antigen testing for Legionella pneumophila and Streptococcus pneumoniae was obtained as part of the standard diagnostic evaluation for unexplained hypoxia. Blood cultures subsequently returned positive for Gram‐positive cocci, prompting substitution of doxycycline with vancomycin. The organism was later identified as Streptococcus canis using matrix‐assisted laser desorption/ionization time‐of‐flight mass spectrometry (MALDI‐TOF MS). Antimicrobial susceptibility testing was performed using standard laboratory methods and demonstrated susceptibility to beta‐lactam antibiotics, including ceftriaxone, which guided definitive therapy. On further questioning, the patient reported a dog scratch from her daughter’s pet several weeks prior to admission that resulted in a break in the skin with minor bleeding but did not require medical attention. She denied other animal exposures or recent open wounds.
After 2 days of targeted therapy with ceftriaxone, the patient showed significant clinical improvement, with resolution of her oxygen requirement and decreasing inflammatory markers. However, she continued to experience severe lumbar back pain. A CT of the thoracic and lumbar spine findings was interpreted as degenerative and not consistent with infectious involvement (Figures 1 and 2). MRI was not feasible due to the patient’s non conditional pacemaker. Given her bacteremia and implanted cardiac device, a transthoracic echocardiogram (TTE) was performed and was unrevealing. A follow‐up transesophageal echocardiogram (TEE), done per infectious disease recommendations, showed no valvular or lead vegetations (Figure 3).
Computed tomography (CT) of the lumbar spine without intravenous contrast, sagittal and coronal reconstructions, demonstrating no prevertebral or paraspinal soft tissue edema to suggest discitis, osteomyelitis, or septic arthritis.
Computed tomography (CT) of the thoracic spine without intravenous contrast and sagittal and coronal reconstructions, demonstrating no evidence of osseous involvement.
Transesophageal echocardiogram (TEE), midesophageal four‐chamber view, demonstrating no evidence of valvular vegetations or pacemaker lead–associated vegetations.
The patient demonstrated rapid clinical improvement with resolution of hypoxia, clearance of bacteremia, and declining inflammatory markers. Repeat blood cultures were negative. She was discharged to inpatient rehabilitation to complete a 2‐week course of intravenous ceftriaxone, after which she was able to return home and recovered without recurrence of infection.
3. Discussion
This case illustrates S. canis as a rare but significant cause of bacteremia in humans, particularly in elderly or immunocompromised hosts. Although typically associated with canine and feline microbiome, S. canis can be transmitted zoonotically, even from seemingly benign exposures. Although most human S. canis infections are linked to animal exposure with an apparent bite or scratch, several well documented cases include septicemia in a dog owner without any bite and native mitral valve endocarditis after a simple dog contact without any trauma [3–5]. In this case, the only identified risk factor was a minor dog scratch several weeks prior to symptom onset.
The patient presented with sepsis and developed a new oxygen requirement, suggesting pulmonary involvement, although imaging showed only minimal, nonspecific ground‐glass changes. Although the patient’s clinical status rapidly improved with antibiotics, previously reported cases of sepsis or valvular involvement prompted early infectious disease consultation and extensive imaging for sources of colonization. The patient’s severe lumbar back pain initially raised concern for osseous involvement. Moreover, her permanent pacemaker raised concern for device‐related infection, prompting cardiac imaging via TTE then TEE.
Although S. canis is rarely encountered in human infections, literature reports demonstrate its potential for causing invasive disease, including endocarditis, septic arthritis, and necrotizing infections. Causes often arise without obvious bite or scratch injuries, making clinical suspicion difficult [6–9]. Risk factors for severe disease include advanced age, underlying comorbidities, immunosuppression, and the presence of prosthetic material. Identification and susceptibility testing are essential to guide therapy, as S. canis is typically susceptible to beta‐lactam antibiotics. Delayed recognition and treatment may result in serious complications, including valve destruction, embolic events, and increased mortality; notably, Group C and Group G streptococcal endocarditis of which Streptococcus canis is a member has been associated with mortality rates approaching 17% [10].
4. Conclusion
This case highlights the importance of considering zoonotic pathogens in patients with unclear sources of infection and animal exposure. Even if initial clinical suspicion for zoonotic infection is low, thorough history of potential infectious exposures can guide infectious evaluation, particularly when the initial infectious source is unclear. Without advanced microbiology laboratory testing to isolate rare species, history of zoonotic or pet exposure would have been the only evidence of infectious source, given her negative urinary and respiratory cultures. Prompt diagnosis, appropriate imaging, and tailored antimicrobial therapy led to a favorable outcome in this complex patient with multiple comorbidities and an indwelling cardiac device.
Abbreviations used throughout the manuscript are summarized in Table 2.
Funding
This work did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors.
Disclosure
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Consent
Consent was obtained from the patient prior to the use of de‐identified patient information for the purpose of writing and publishing this report. The West Virginia University Institutional Review Board reviewed the project and determined it was Not Human Subjects Research and that an IRB protocol was not required.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prescott J. F. , Sykes J. E. , and Daniels J. B. , 50-Streptococcal and Enterococcal Infections, Greene’s Infectious Diseases of the Dog and Cat. (2021) 5th edition, W.B. Saunders, 597–610.
- 2Galpérine T. , Cazorla C. , Blanchard E. , Boineau F. , Ragnaud J. M. , and Neau D. , Streptococcus canis Infections in Humans: Retrospective Study of 54 Patients, Journal of Infection. (2007) 55, no. 1, 23–26, 10.1016/j.jinf.2006.12.013, 2-s 2.0-34250023701.17320186 · doi ↗ · pubmed ↗
- 3Amsallem M. , Iung B. , Bouleti C. et al., First Reported Human Case of Native Mitral Infective Endocarditis Caused by Streptococcus canis , Canadian Journal of Cardiology. (2014) 30, no. 11, 1462.e 1–2, 10.1016/j.cjca.2014.07.013, 2-s 2.0-84908474048.25442453 · doi ↗ · pubmed ↗
- 4Lacave G. , Coutard A. , Troché G. et al., Endocarditis Caused by Streptococcus canis: an Emerging Zoonosis?, Infection. (2016) 44, no. 1, 111–114, 10.1007/s 15010-015-0809-3, 2-s 2.0-84932098242.26104727 · doi ↗ · pubmed ↗
- 5Ohtaki H. , Ohkusu K. , Ohta H. et al., A Case of Sepsis Caused by Streptococcus canis in a Dog Owner: a First Case Report of Sepsis Without Dog Bite in Japan, Journal of Infection and Chemotherapy. (2013) 19, no. 6, 1206–1209, 10.1007/s 10156-013-0625-6, 2-s 2.0-84890859204.23740090 · doi ↗ · pubmed ↗
- 6Chamat-Hedemand S. , Dahl A. , Østergaard L. et al., Prevalence of Infective Endocarditis in Streptococcal Bloodstream Infections is Dependent on Streptococcal Species, Circulation. (2020) 142, no. 8, 720–730, 10.1161/CIRCULATIONAHA.120.046723.32580572 · doi ↗ · pubmed ↗
- 7Mališová B. , Šantavý P. , Lovečková Y. et al., Human Native Endocarditis Caused by Streptococcus canis-a Case Report, Acta Pathologica, Microbiologica et Immunologica Scandinavica. (2019) 127, no. 1, 41–44, 10.1111/apm.12905, 2-s 2.0-85058770533.30549135 · doi ↗ · pubmed ↗
- 8Takeda N. , Kikuchi K. , Asano R. et al., Recurrent Septicemia Caused by Streptococcus canis After a Dog Bite, Scandinavian Journal of Infectious Diseases. (2001) 33, no. 12, 927–928, 10.1080/00365540110076903, 2-s 2.0-0035700047.11868767 · doi ↗ · pubmed ↗