Spontaneous retroperitoneal haematoma causing acute haemodynamic collapse: a case report
Sandeepa Dadigamuwage, Vimarshini Samarakoon, Rajesh Thengungal Kochupapy

TL;DR
A 70-year-old man with a rare abdominal bleed died despite medical efforts due to treatment delays and refusal of blood transfusion.
Contribution
This case report emphasizes the importance of rapid diagnosis and intervention in acute retroperitoneal hemorrhage.
Findings
Computed tomography confirmed a large retroperitoneal haematoma with active bleeding.
The patient's refusal of blood transfusion complicated management and contributed to his death.
Timely access to endovascular embolisation is critical in such emergencies.
Abstract
Spontaneous retroperitoneal haemorrhage is a rare but potentially life-threatening cause of acute abdominal pain and shock. We report a 70-year-old man with polycythaemia on aspirin who presented with sudden right-sided abdominal pain, groin discomfort, leg paraesthesia and haemodynamic instability. Computed tomography (CT) demonstrated a large right-sided retroperitoneal haematoma with active arterial extravasation, confirmed on CT angiography. Management was complicated by the patient’s refusal of blood transfusion despite counselling. Although endovascular embolisation was planned, his clinical deterioration coincided with interventional radiology being unavailable due to another emergency. He progressed to refractory shock and died 21 hours after presentation. This case highlights the need for early CT imaging, timely access to embolization and sensitive communication when patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
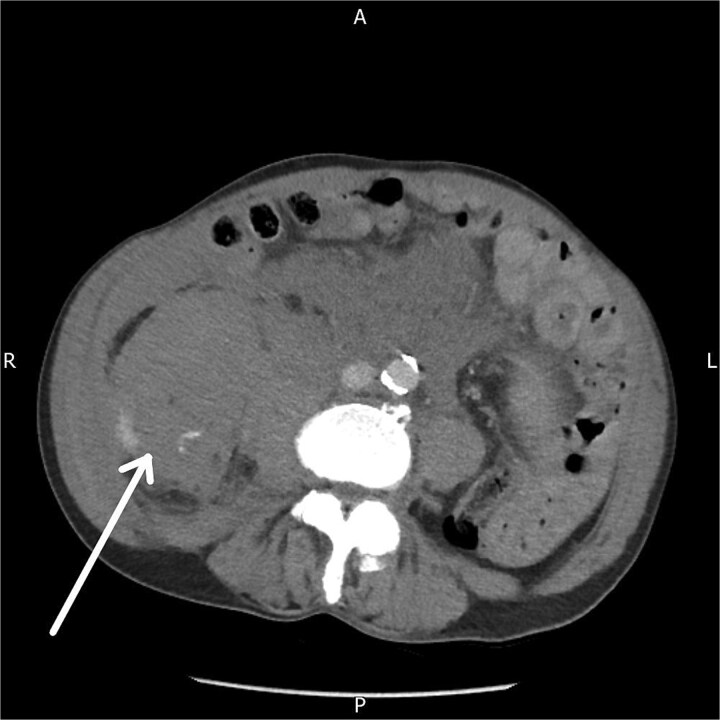 Figure 1
Figure 1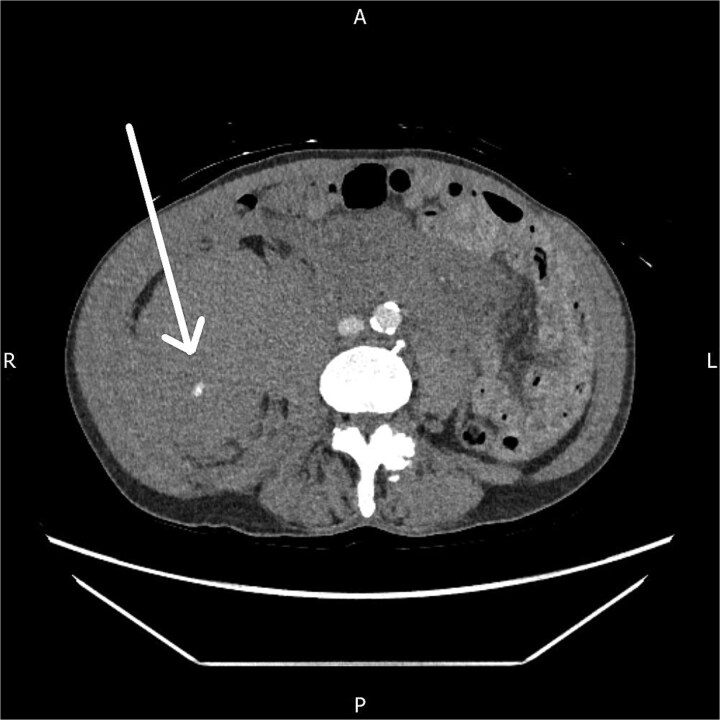 Figure 2
Figure 2| Parameter | On admission | 13 Hours after admission | Reference range |
|---|---|---|---|
| Haemoglobin (g/L) | 150 | 112 | 130–175 g/L |
| White Cell Count (×109/L) | 53.6 | 84.9 | 3.6–9.2 × 109/L |
| Neutrophils (×109/L) | 46.4 | 71.9 | 1.7–6.2 × 109/L |
| Platelets (×109/L) | 567 | 814 | 150–450 × 109/L |
| CRP (mg/L) | 12 | 27.1 | 0.1–5 mg/L |
| Urea (mmol/L) | 8.7 | 11.7 | 2.5–7.8 mmol/L |
| Creatinine (μmol/L) | 94 | 136 | 64–104 μmol/L |
| Sodium (mmol/L) | 138 | 137 | 133–146 mmol/L |
| Potassium (mmol/L) | 5.4 | 4.9 | 3.5–5.3 mmol/L |
| Lactate (mmol/L) | 3.2 | 14.0 | 0.5–2.0 mmol/L |
| pH | 7.39 | 7.14 | 7.35–7.45 |
| PaO₂ (kPa) | 9.2 | 3.37 | 10–13 kPa |
| PaCO₂ (kPa) | 5.3 | 5.52 | 4.7–6.0 kPa |
| SaO₂ (%) | 93.1 | 23.0 | 95–100% |
| Bicarbonate (mmol/L) | N/A | 13.5 | 22–26 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCase Reports on Hematomas · Abdominal Trauma and Injuries · Spinal Hematomas and Complications
Introduction
Spontaneous retroperitoneal haematoma is a rare but potentially life-threatening condition occurring without trauma or iatrogenic injury. It accounts for around 1% of acute abdominal emergencies and carries a mortality rate of 20%–30%, largely due to delayed recognition and sudden haemodynamic collapse [1, 2]. Spontaneous retroperitoneal haematoma is most often associated with anticoagulation, advanced age, vascular fragility or underlying comorbidities, although idiopathic cases are well described [3].
Clinical presentation is variable, ranging from flank or abdominal pain to profound shock, and symptoms may be non-specific until significant bleeding has occurred. Contrast-enhanced computed tomography (CT) is essential for diagnosis, allowing confirmation of bleeding, assessment of extent and detection of active extravasation, a key predictor of deterioration and need for intervention [4].
Management is guided by haemodynamic status. Stable patients may be managed conservatively, while active bleeding or instability usually requires urgent endovascular embolization or surgery [5].
Case report
A 70-year-old man presented with sudden onset right lower abdominal pain radiating to the groin, accompanied by numbness of the right leg. The pain began while rising from a sunbed. His medical history included polycythaemia managed with daily aspirin, and he was under regular haematology follow-up. He reported minor trauma to the right flank two weeks prior.
On examination, he appeared pale and distressed. His observations showed hypotension with a systolic blood pressure of 90 mmHg and tachycardia. Abdominal examination revealed marked right lower abdominal tenderness, and neurological assessment identified paraesthesia of the right leg up to the knee. Howship–Romberg sign was positive. Based on the unilateral groin pain and neurological findings, an obturator hernia was initially suspected.
Initial laboratory results showed a haemoglobin of 150 g/L and raised inflammatory markers. A summary of investigations on admission and at 13 hours is provided in Table 1.
A contrast-enhanced CT abdomen and pelvis performed five hours after presentation demonstrated a large right-sided retroperitoneal haematoma extending from the perinephric region into the psoas compartment, with clear evidence of active arterial extravasation (Fig. 1). Splenic enlargement with patchy enhancement was also noted, felt to represent a perfusion abnormality. No underlying mass or vascular lesion was identified.
Axial contrast-enhanced CT abdomen and pelvis demonstrating a right-sided retroperitoneal haematoma with evidence of active contrast extravasation.
Given the initial haemodynamic improvement following fluid resuscitation, and after discussion with interventional radiology, embolization was deferred, with a plan for close monitoring. Thirteen hours after admission, his haemoglobin had fallen significantly, prompting a CT angiogram. At that point, the patient disclosed an advance decision refusing any blood or blood-product transfusion due to concerns about mRNA vaccine contamination in donor blood. His decision-making capacity was formally assessed and documented.
The CT angiogram, performed 14 hours after presentation, showed a further increase in the size of the haematoma with ongoing active arterial contrast extravasation (Fig. 2). Despite the clear need for embolization, the interventional radiology team was unavailable due to a concurrent emergency life-saving procedure.
Axial CT angiogram showing persistent right-sided retroperitoneal haematoma with ongoing active contrast extravasation.
The patient subsequently deteriorated rapidly with worsening hypotension and respiratory failure. Emergency laparotomy was considered but deemed unsafe without transfusion support. Despite maximal non-blood resuscitation and intravenous tranexamic acid, he suffered a cardiac arrest and died approximately 21 hours after admission.
Discussion
Spontaneous retroperitoneal haematoma is an uncommon but serious condition that typically occurs in anticoagulated or medically complex patients, although minor unnoticed trauma may be contributory [6]. The retroperitoneal cavity can accommodate large volumes of blood before producing overt clinical signs, accounting for the delayed or subtle presentation seen in many cases. Patients may initially report flank or abdominal pain, but rapid progression to haemodynamic instability is well recognized [7].
CT is central to diagnosis, confirming the presence and extent of bleeding and identifying features such as active contrast extravasation, which strongly predict deterioration and the need for intervention [8]. Haemodynamically stable patients without radiological evidence of ongoing haemorrhage may be managed conservatively with close monitoring, whereas worsening instability or active bleeding usually warrants urgent endovascular embolization, now considered the preferred minimally invasive approach [9]. Surgical exploration is reserved for refractory cases or when interventional radiology is unavailable [10].
In this case, initial stabilization was followed by sudden deterioration, and although embolization was planned, access to interventional radiology was delayed due to a concurrent emergency. This reflects a practical challenge: the window for intervention in spontaneous retroperitoneal haematoma can be narrow, and system pressures may critically influence outcome. Additionally, management was complicated by the patient’s refusal of blood transfusion due to concerns about vaccine-related contamination. Such beliefs are increasingly encountered and require clear, empathetic communication, yet may limit life-saving options at crucial moments [11].
This case underscores the rapid clinical trajectory of spontaneous retroperitoneal haematoma and the importance of timely imaging, coordinated escalation and sensitive, patient-centred decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sunga KL, Bellolio MF, Gilmore RM et al. Spontaneous retroperitoneal hematoma: etiology, characteristics, management, and outcome. J Emerg Med 2012;43:e 157–61. 10.1016/j.jemermed.2011.06.00621911282 · doi ↗ · pubmed ↗
- 2Chan YC, Morales JP, Reidy JF et al. Management of spontaneous and iatrogenic retroperitoneal haemorrhage: conservative management, endovascular intervention or open surgery? Int J Clin Pract 2008;62:1604–13.17949429 10.1111/j.1742-1241.2007.01494.x · doi ↗ · pubmed ↗
- 3Wytock DH, Lebron RP, Milano CA et al. Spontaneous retroperitoneal hemorrhage: management in the endovascular era. J Vasc Surg 2019;70:573–9.
- 4Takahashi M, Yoshida K, Shimura T et al. Spontaneous retroperitoneal hematoma: role of multidetector CT in diagnosis and management. Clin Radiol 2010;65:751–7.
- 5García-Moncó JC, Antuña S, Escribano D et al. Management of spontaneous retroperitoneal hematoma: a multicenter experience. Eur J Trauma Emerg Surg 2019;45:1107–14.30167738
- 6Sunga KL, Bellolio MF, Gilmore RM et al. Spontaneous retroperitoneal hemorrhage: diagnosis and management. Int J Emerg Med 2012;5:51.10.1016/j.jemermed.2011.06.00621911282 · doi ↗ · pubmed ↗
- 7Chan YC, Morales JP, Reidy JF et al. Endovascular management of spontaneous retroperitoneal haemorrhage: indications and outcomes. Int J Clin Pract 2008;62:1604–13.17949429 10.1111/j.1742-1241.2007.01494.x · doi ↗ · pubmed ↗
- 8Takahashi M, Yoshida K, Shimura T et al. Multidetector CT in spontaneous retroperitoneal hematoma: predicting active bleeding. Clin Radiol 2010;65:751–7.