Voxel-based spatial distribution of intracranial meningioma subtypes and their relationship to radiogenomic maps
Georgios Naros, Aldo Spolaore, Sophie Wang, Mykola Gorbachuk, Kathrin Machetanz, Benjamin Bender, Felix Behling, Jens Schittenhelm, Marcos Tatagiba

TL;DR
This study maps the brain locations of different meningioma subtypes and shows how their positions relate to genetic patterns and tumor grades.
Contribution
The study introduces voxel-based spatial templates that link meningioma subtypes to genetic mutations and tumor grades.
Findings
Meningioma subtypes show distinct spatial preferences that align with known genetic mutation maps.
Predictive modeling using spatial features achieved moderate accuracy in predicting histological subtypes and higher accuracy for tumor grading.
Higher-grade meningiomas are more likely to occur in the frontoparietal transition zone.
Abstract
Meningiomas are histologically and genetically heterogeneous tumors with varying anatomical distributions. While distinct genetic mutations have been associated with specific tumor locations, the spatial distribution of histological subtypes and their relationship to radiogenomic profiles remains poorly defined. Moreover, the predictive value of spatial information for histopathological classification and tumor grading has not yet been systematically explored. This study aimed to systematically analyze the anatomical predilection of histological meningioma subtypes and their concordance with known mutation-specific spatial patterns, and the predictive potential of voxel-based spatial features. We retrospectively analyzed 737 patients undergoing surgical resection of intracranial meningiomas. Preoperative magnetic resonance images were normalized to a common stereotactic space, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
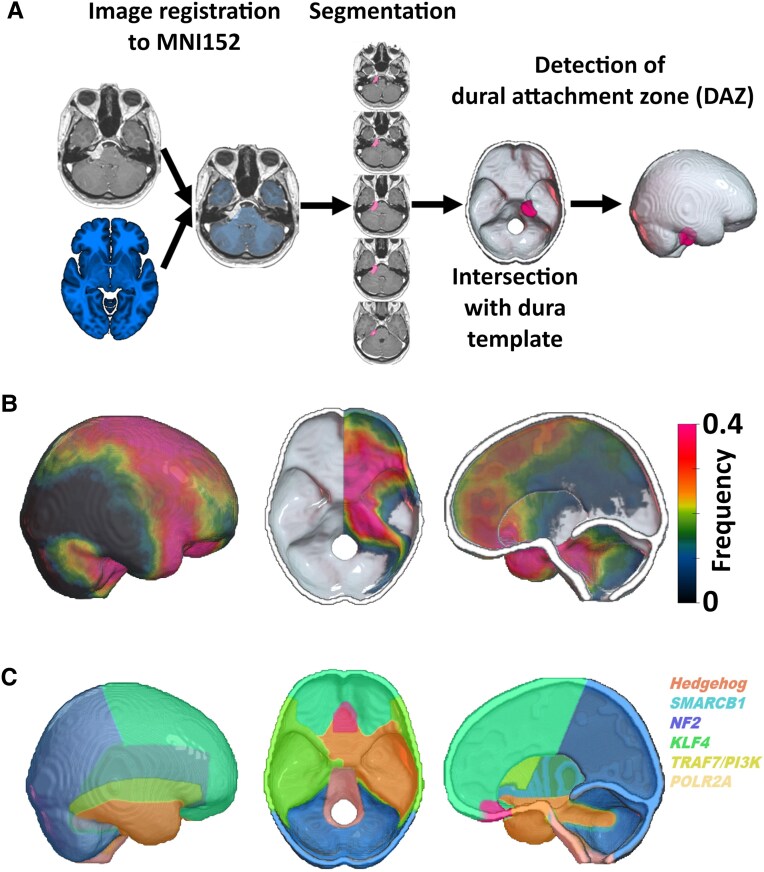 Figure 1
Figure 1|
| |
|---|---|
|
| 57.0 ± 12.7 |
|
| |
| Female | 540 (73) |
| Male | 197 (27) |
|
| 34.2 ± 40.3 |
|
| |
| | 302 (41) |
| Parasagittal | 115 (16) |
| Falcine | 47 (6) |
| Cerebral convexity | 140 (19) |
| | 435(59) |
| Cavernous sinus | 14 (2) |
| Sphenoid wing | 58 (8) |
| Clinoidal | 62 (8) |
| Tuberculum sellae | 53 (7) |
| Planum sphenoidale | 14 (2) |
| Olfactory groove | 33 (5) |
| Petroclival | 48 (7) |
| CPA | 58 (8) |
| Cerebellar convexity | 16 (2) |
| Tentorial | 28 (4) |
| Foramen jugulare | 11 (2) |
| Foramen magnum | 13 (2) |
| Temporobasal | 10 (1) |
| Frontobasal | 16 (2) |
| Histology | |
| Meningothelial | 372 (51) |
| Fibrous | 58 (8) |
| Transitional | 85 (12) |
| Psammomatous | 20 (3) |
| Angiomatous | 18 (2) |
| Microcytic | 19 (3) |
| Secretory | 29 (4) |
| lymphoplasmacyte | 0 (0) |
| Metaplastic | 6 (1) |
| Chordoid | 12 (2) |
| Clear cell | 1 (0) |
| Papillary | 0 (0) |
| Rhabdoid | 2 (0) |
| Atypical | 113 (15) |
| Anaplastic | 2 (0) |
| WHO | |
| CNS Grade 1 | 579 (79) |
| CNS Grade 2 | 156 (21) |
| CNS Grade 3 | 2 (0) |
- —University of Tübingen10.13039/501100002345
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Glioma Diagnosis and Treatment · Pituitary Gland Disorders and Treatments
Introduction
Meningiomas are the most common primary intracranial tumor in adults,^1^ originating from arachnoidal cap cells of the leptomeninges.^2^ In recent decades, several genetic mutations were identified that are associated with both the tumorigenesis of meningiomas^3^ and the oncological outcome after treatment.^4,5^ These factors contribute to the development of different histological phenotypes and the frequently updated World Health Organization (WHO) gradings.^2,3,6^ Meningiomas linked to deletions on chromosome 22q (affecting NF2 or SMARCB1) are commonly associated with fibrous, psammomatous, transitional, atypical and anaplastic histological subtypes.^7,8^ *NF2-*mutated meningiomas represent the majority of tumors located in the falx cerebri, tentorium cerebelli, as well as cerebral and cerebellar convexities.^8-11^ Mutations in the PI3K-AKT-mTOR pathway (including AKT1, AKT3, PIK3CA, PIK3R1) have been observed in CNS WHO grade I meningothelial or transitional meningiomas arising from the medial skull base.^12,13^ Additionally, mutations affecting the Hedgehog signaling pathway (such as SMO, SUFU, PRKA-R1A) are more likely to result in CNS WHO Grade 1 meningothelial subtype located in the midline of the anterior cranial fossa.^8-10^ Furthermore, there are several other pathogenic variants (including KLF4, TRAF7, SMARCE1, BAP1) associated with secretory, meningothelial, clear cell or rhabdoid histology subtype of skull base meningiomas.^9^
Despite these findings, data on the spatial distribution of meningioma subtypes and their relationship to genetic factors and embryological origins remain limited and inconclusive.^9^ The location of intracranial meningiomas is generally described by their dural attachment zone (DAZ), but in large tumors (such as those in the falx or sphenoid wing), this can be obscured, and in some cases (such as convexity meningiomas), the DAZ description can be imprecise. Voxel-based lesion-symptom mapping (VLSM) offers a promising tool to investigate these complex relationships. This imaging-based statistical technique enables the spatial localization of disease patterns by normalizing individual tumor masks into a standard stereotactic space. VLSM allows for objective, rater-independent analyses of tumor location across cohorts, facilitating the identification of anatomical clusters associated with particular histological and clinical variables. Although VLSM has been widely applied in focusing on stroke and other focal brain lesion, its application in neuro-oncology—and specifically in meningioma research—remains limited. Only a few prior studies have employed this approach to characterize the spatial distribution of intracranial meningiomas,^14,15^ and even fewer have integrated histopathological or genetic data into the analysis.^16^
The present study seeks to address these gaps by applying voxel-based lesion symptom mapping to a large cohort of patients with histologically confirmed intracranial meningiomas. By combining spatial localization with detailed histological subtyping, we aim to delineate the anatomical distribution of meningioma subtypes in a statistically robust, unbiased manner. By comparing the spatial profile of different subtypes to known radiogenomic mutations maps, we intend to explore the spatial-genomic-histologic landscape of meningiomas and provide novel insights into their pathophysiology, with potential implications for classification, prognosis, and targeted therapeutic strategies.
Materials and methods
Patient population
This retrospective observational single center study enrolled 1175 patients who underwent surgical treatment of intracranial meningioma between 2007 and 2017 at our institution. 737/1175 (63%) of cases met the inclusion criteria defined as sufficient quality of preoperative magnetic resonance imaging (MRI), first-line treatment and complete clinical information about histopathological results. Eleven patients (1.5%) with intraventricular meningiomas were excluded. The clinical data was acquired from medical records including age at diagnosis, gender and histopathological findings. Tumor locations were evaluated based on preoperative MRI by experienced, board-certified skull base neurosurgeons. Histopathological diagnosis was reclassified according to the WHO 2021 classification.^17^ Details of the clinical and demographic characteristics are depicted in Table 1. This study was approved by the local ethics committee of the Medical Faculty of the Eberhard Karls University Tuebingen (No. 702/2024B02) and performed in accordance with the Declaration of Helsinki. All participants gave written informed consent. The results are reported following the STROBE guidelines.^18^
Magnetic resonance imaging
Imaging studies were conducted at our institution using 1.5 T MRI scanner (MRI; Siemens Healthineers) including a high-resolution T1-weighted contrast-enhanced MPRAGE sequence (slice thickness: 1.0 mm; TR: 2300 ms; TE: 3.51 ms; TI: 1100; flip angle: 8°; pixel bandwidth: 130; pixel spacing: 1/1 mm; matrix: 256 × 256). Nevertheless, many of the segmentations were carried out on preoperative MRI that have been performed externally, therefore the above listed parameters may vary significantly among patients. The last scan before surgery was used for analyses.
Voxel-based lesion symptom mapping (VLSM)
All Digital Imaging and Communications in Medicine (DICOM) format images were first converted to the Neuroimaging Informatics Technology Initiative (NIfTI) format by using dcm2niix.^19^ Statistical Parametric Mapping Software version 12 (SPM12, Institute of Neurology, University College London, London, UK; https://www.fil.ion.ucl.ac.uk/spm/docs/) and MATLAB (R2024a, MathWorks, Natick, MA, USA) were used to register and normalize patient’s MR images to a standard brain template (MNI152; Montreal Neurological Institute, McGill University, Montreal, Quebec, Canada) (Fig. 1). The registration was visually assessed, and a manual correction was applied if required. The normalized image was resampled to a voxel size of 1 × 1 × 1 mm. The tumor was semi-automatically segmented using a fast-marching method implemented in MATLAB (see Supplementary material). The segmentation was performed and reviewed by two neurosurgeons. Manual corrections to the tumor mask were made in MRIcron (https://www.nitrc.org/projects/mricron/). The individual tumor volume was noted, and the tumor mask was saved for further analysis. All tumor masks were mirrored to the right hemisphere of the brain. Dural attachment zone (DAZ) was acquired by intersecting the tumor mask with a template representing the dura, falx and tentorium. This template was generated based on a publicly available high-resolution computer tomography (CT) template^20^ and falx/tentorium masks provided by Brain Biomechanics Imaging Resources Project (https://www.nitrc.org/projects/bbir). Voxel-based lesion symptom mapping (VLSM) enables to evaluate the relationship of a predictor (e.g. DAZ of the meningioma) to a specific outcome or feature (e.g. histopathological subtype) at individual voxels (i.e. voxel-vice).^21^ In this study, VLSM was based on a univariable linear regression model and one-tail t-statistics as implemented in SPM12 (https://www.fil.ion.ucl.ac.uk/spm) and NiiStat (https://www.nitrc.org/projects/niistat). Categorial variables were incorporated after dummy coding (0: reference group; 1: observational group). Only voxels affected in at least 10 patients were included in the VLSM analysis to ensure sufficient statistical power and to minimize the influence of outliers.^22^ Thus, 193 228 voxels were included in the VLSM analysis. VLSM statistics provides Z-scores representing standardized test statistics derived from these models. A positive Z-score indicates a positive association between the occurrence of meningiomas in this voxel and a specific feature (e.g. a specific histopathological subtype). To account for multiple comparisons across the numerous voxels analyzed, False Discovery Rate (FDR) correction is applied. This statistical method controls the expected proportion of false positives among the voxels identified as significant, enhancing the reliability of the results.^22,23^
Workflow. (A) Patients’ individual MRI data were registered to a 1-mm isotropic, high-resolution, T1-weighted MRI template provided by the Montreal Neurological Institute (MNI). Meningiomas were semi-automatically segmented and flipped to the right hemisphere. Tumor masks were intersected with a standardized template representing the dura and falx to detect the dural attachment zone (DAZ) of the meningioma. This information was used for the voxel-wise lesion symptom mapping analysis. (B) Frequency maps represent the spatial distribution of meningioma DAZ in the present cohort (n = 737). Warmer colors indicate higher tumor frequency across the cohort, highlighting anatomical hotspots. Meningiomas were most frequently located at the anterior two-thirds of the falx cerebri, the frontal convexity, the sphenoid wing, and the petroclival junction. In contrast, tumors were rarely observed in the parieto-occipital and cerebellar convexity. This map provides a reference for the overall anatomical distribution of meningiomas prior to subtype-specific stratification. (C) Schematic radiogenomic mutation maps illustrating the known anatomical predilection of meningiomas harboring common driver mutations. These binary maps were manually created based on anatomical descriptions in the literature3,7,9,10,12,13,24-31 and used for voxel-wise spatial concordance analysis with histological subtypes.
Predictive modeling of histology and grade
To determine whether tumor localization carries predictive value for histological subtype or CNS WHO grade, a multinomial logistic regression model was implemented in MATLAB (R2024a, MathWorks, Natick, MA, USA). For each patient, the individual tumor mask was intersected with the corresponding subtype-specific VLSM probability maps (Z-scores). The mean Z-value within the intersection was extracted as a spatial covariate, reflecting the degree of spatial similarity between the individual tumor and each subtype-specific spatial pattern. A regularized multinomial logistic regression model was then trained using a ridge-penalized linear learner within a one-versus-all coding framework (see Supplementary material). Model performance was evaluated using fivefold cross-validation to prevent overfitting and to estimate generalizability. Separate models were constructed for histological subtype classification (including subtypes represented by ≥10 patients) and CNS WHO grade prediction (Grade 1 versus Grade 2). Predictive performance was quantified by overall accuracy (ACC), per-class accuracy, and macro-averaged area under the receiver operating characteristic curve (AUC).
Radiogenomic maps of meningioma associated mutations
Mutation-specific spatial distribution maps were generated based on previously published data describing the anatomical predilection of genetically defined meningioma subgroups.^3,7,9,12,13,24-36^ For this purpose, schematic mutation maps were constructed for the most common driver mutations in meningioma tumorigenesis, including NF2, SMARCB1, Hedgehog (SMO, SUFU) AKT1, TRAF7, KLF4, and POLR2A. Each map was manually delineated using a high-resolution MNI152 brain template, reflecting the region’s most frequently associated with each mutation (see Supplementary Table 1, Fig. 1). To quantify the spatial concordance between histological subtype-specific maps and radiogenomic mutation templates, we performed an area under the curve–receiver operating characteristic (AUC-ROC) analysis (perfcurve.m MATLAB function). This approach evaluates the ability of a continuous probability map (derived from VLSM) to distinguish between voxels belonging to a given mutation-specific anatomical distribution (binary mask) and those that do not. The AUC value ranges from 0.5 (no discrimination) to 1.0 (perfect discrimination), with higher values indicating greater spatial overlap. An AUC > 0.7 was considered indicative of significant spatial concordance. This voxel-wise analysis provides a robust, threshold-independent measure of the spatial correspondence between histological and radiogenomic patterns.
Statistics
Statistical evaluation of clinical data was performed using SPSS (IBM SPSS Statistics for Windows, Version 25.0, Armonk, NY: IBM Corporation) and custom-written MATLAB scripts including MATLAB statistics toolbox. For comparison of categorical data, we used a chi-squared test (X² test). Group comparisons of metric variables were based on non-parametric Mann-Whitney U-tests. P-values < 0.05 were considered significant. Results are shown as mean ± standard deviation (SD).
Supplementary Material
fcag025_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ostrom QT, Price M, Neff C, et al CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2016–2020. Neuro Oncol. 2023;25(12 Suppl 2):IV 1–IV 99.37793125 10.1093/neuonc/noad 149PMC 10550277 · doi ↗ · pubmed ↗
- 2Riemenschneider MJ, Perry A, Reifenberger G. Histological classification and molecular genetics of meningiomas. Lancet Neurol. 2006;5(12):1045–1054.17110285 10.1016/S 1474-4422(06)70625-1 · doi ↗ · pubmed ↗
- 3Fountain DM, Smith MJ, O’Leary C, et al The spatial phenotype of genotypically distinct meningiomas demonstrate potential implications of the embryology of the meninges. Oncogene. 2020;40(5):875–884.33262459 10.1038/s 41388-020-01568-6PMC 8440207 · doi ↗ · pubmed ↗
- 4Wang JZ, Patil V, Landry AP, et al Molecular classification to refine surgical and radiotherapeutic decision-making in meningioma. Nat Med. 2024;30:3173–3183.39169220 10.1038/s 41591-024-03167-4PMC 11564112 · doi ↗ · pubmed ↗
- 5Youngblood MW, Miyagishima DF, Jin L, et al Associations of meningioma molecular subgroup and tumor recurrence. Neuro Oncol. 2021;23(5):783–794.33068421 10.1093/neuonc/noaa 226PMC 8099468 · doi ↗ · pubmed ↗
- 6Kalamarides M, Stemmer-Rachamimov AO, Niwa-Kawakita M, et al Identification of a progenitor cell of origin capable of generating diverse meningioma histological subtypes. Oncogene. 2011;30(20):2333–2344.21242963 10.1038/onc.2010.609 · doi ↗ · pubmed ↗
- 7Preusser M, Brastianos PK, Mawrin C. Advances in meningioma genetics: Novel therapeutic opportunities. Nat Rev Neurol. 2018;14(2):106–115.29302064 10.1038/nrneurol.2017.168 · doi ↗ · pubmed ↗
- 8Brastianos PK, Horowitz PM, Santagata S, et al Genomic sequencing of meningiomas identifies oncogenic SMO and AKT 1 mutations. Nat Genet. 2013;45(3):285–289.23334667 10.1038/ng.2526 PMC 3739288 · doi ↗ · pubmed ↗