Anatomical Shifts of the Bowel During Positioning: Relevance to Prone Lateral Access Surgery
Takashi Sono, Hiroshi Iwata, Yasuyuki Onishi, Takayosh Shimizu, Koichi Murata, Bungo Otsuki, Shuichi Matsuda

TL;DR
This study shows that the bowel shifts backward in the prone position, which is important for lateral spine surgery planning.
Contribution
The study quantifies bowel positional changes in prone versus supine positions for lateral lumbar surgery.
Findings
Bowel displacement was consistently posterior in the prone position at L2/3, L3/4, and L4/5 levels.
Female sex and prior abdominal surgery were linked to reduced bowel mobility at L3/4 and L4/5.
The abdominal aorta showed minimal positional change between postures.
Abstract
This radiographic analysis aimed to evaluate the differences in the anatomical position of the bowel relative to the lateral surgical corridor and the spine between prone and supine positions. Retroperitoneal transpsoas lateral lumbar interbody fusion can be performed in the prone position, allowing simultaneous lateral and posterior spinal access without repositioning; however, bowel positional changes associated with this approach have not been well characterized. From January 2020 to December 2024, 13 patients who underwent computed tomography (CT)-guided biopsy in the prone position with imaging spanning L2-L5 were retrospectively analyzed. Patient factors, including age, sex, body mass index, history of abdominal surgery, and malignancy, were recorded. Supine and prone CT scans obtained within one month were used to measure the distances from the posterior vertebral line to the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
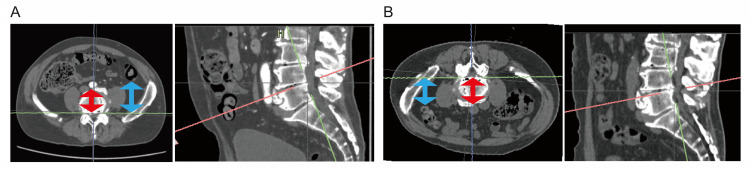 Figure 1
Figure 1| Mean±SD | |
| Age | 60.2±18.2 |
| Sex (male/female) | 8/5 |
| Body mass index | 20.8±2.2 |
| Malignancy (present/absent) | 11/2 |
| Abdominal operation (present/absent) | 6/7 |
| Levels | DBV prone | DBV supine | ΔDBV | DAV prone | DAV supine | ΔDAV |
| L2/3 | 30.9±24.3 | 31.5±34.7 | -0.6±18.6 | 44.9±9.0 | 45.3±8.6 | -0.4±3.1 |
| L3/4 | 23.0±21.5 | 26.5±30.4 | -3.5±15.7 | 45.1±7.6 | 47.1±8.4 | -1.9±6.0 |
| L4/5 | 20.4±18.4 | 25.5±19.5 | -5.1±8.2 | 44.5±7.7 | 44.2±9.1 | 0.3±3.3 |
| Factors | R2 | Standard β | P-value | |
| ΔDBV in L3/4 | Abdominal operation | 0.61 | 0.61 | 0.04* |
| Female | 0.66 | 0.03* | ||
| ΔDBV in L4/5 | Abdominal operation | 0.67 | 0.64 | 0.01* |
| Malignancy | 0.62 | 0.01* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Cervical and Thoracic Myelopathy · Spinal Fractures and Fixation Techniques
Introduction
Lumbar interbody fusion can be performed using several surgical approaches, each with distinct anatomical corridors, indications, and risk profiles. Posterior lumbar interbody fusion (PLIF) is performed through a midline posterior approach, allowing bilateral access to the disc space after retraction of the dural sac and nerve roots; although it provides direct decompression, it is associated with greater neural manipulation. Transforaminal lumbar interbody fusion (TLIF) is a modification of PLIF that uses a unilateral posterior approach through the intervertebral foramen, reducing dural retraction while maintaining the ability to achieve circumferential fusion. Anterior lumbar interbody fusion (ALIF) accesses the disc space through an anterior retroperitoneal or transperitoneal approach, enabling the placement of large interbody cages and the restoration of disc height and lumbar lordosis, but with potential risks to major vascular and visceral structures. Lumbar lateral interbody fusion (LLIF) is a well-established surgical approach for the management of lumbar degenerative disorders, providing substantial deformity correction and effective indirect decompression [1-3]. Since it was introduced in 2006, the number of LLIF surgeries has rapidly increased [1,4,5].
In LLIF, lateral cage insertion is performed with the patient in a lateral decubitus position, followed by repositioning to the prone position for pedicle screw placement from the posterior side. However, one major drawback is the time required for repositioning. To address this issue, single-position LLIF was developed. Since 2020, the prone transpsoas approach has been explored as a form of single-position LLIF [6-8].
Some studies have reported that LLIF in the prone position achieves a greater lumbar lordosis than LLIF performed in the lateral decubitus position [9,10]. However, few studies have evaluated how abdominal organs are displaced in the prone position relative to standard supine preoperative imaging. Therefore, this study aimed to investigate positional changes of the intestines and major blood vessels between the supine and prone positions, in order to provide clinically relevant information for planning and safely performing prone transpsoas spinal procedures.
Materials and methods
Between January 2020 and December 2024, we identified 43 patients who underwent prone-position computed tomography (CT)-guided biopsy at Kyoto University Hospital, located in Kyoto, Japan.Of these patients, we selected 13 whose scans included the lumbar spine from L2 to L5. Patient background data, including age, sex, body mass index (BMI), prior abdominal surgery, and history of cancer, were evaluated as factors that could potentially affect abdominal organ displacement.
We measured distance from the posterior vertebral line to the bowel (distance of the bowel to the posterior vertebral line (DBV)) and distance to the abdominal aorta (distance of the abdominal aorta to the posterior vertebral line (DAV)) from CT scans obtained in both supine and prone positions taken within one month (Figure 1). The changes in each measurement (ΔDBV=DBV prone-DBV supine; ΔDAV=DAV prone-DAV supine) were assessed at the intervertebral disc levels from L2/3 to L4/5.
CT images of the lumbar spine in supine and prone positions(A) Left: CT image perpendicular to the L4/5 intervertebral disc space in supine position. Right: Sagittal reconstruction image. Blue arrows indicate the distance of the bowel at the left side to the posterior vertebral line. Red arrows indicate the distance of the abdominal aorta to the posterior vertebral line. (B) Left: CT image perpendicular to the L4/5 intervertebral disc space in prone position. Right: Sagittal reconstruction image. Blue arrows indicate the distance of the bowel at the left side to the posterior vertebral line. Red arrows indicate the distance of the abdominal aorta to the posterior vertebral line.CT: computed tomography
The CT scans were acquired using multidetector scanners. Image processing was performed using Aquarius Net Viewer (TeraRecon, Durham, North Carolina, United States). Prone CT imaging was obtained with bolsters placed under the chest, with both arms positioned forward and the hips extended. Measurements were performed three times on separate occasions by two surgeons (T.S. and H.I.), who were not blinded to patient position. The final value for each parameter was calculated as the mean of these measurements. Interobserver reliability, assessed using the intraclass correlation coefficient (ICC (2,1)), was 0.98 for DBV and 0.84 for DAV. Intraobserver reliability, assessed using ICC (1,3), was 0.98 for DBV and 0.90 for DAV. All ICC analyses were performed using Microsoft Excel (Version 2021; Microsoft, Redmond, Washington, United States). Stepwise multiple regression analyses were conducted using JMP Pro (Version 13.0; SAS Institute Inc., Cary, North Carolina, United States). All candidate variables entered into the regression model included age, sex, BMI, history of abdominal surgery, and history of malignancy. Stepwise selection was performed using a p-value threshold of 0.20, with both forward and backward variable entry and removal allowed and variable combinations evaluated according to this criterion. Multicollinearity was assessed by examining variance inflation factors, and no clinically relevant multicollinearity was identified among the included variables. Statistical significance was set at p<0.05.
This study was approved by the Kyoto University Graduate School of Medicine, Faculty of Medicine, and Hospital Medical Ethics Committee (approval number: R5161) and was conducted in compliance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective design of the study.
Results
The study included 13 patients (eight males and five females) with a mean age of 60.2 years. The average BMI was 20.8. Six patients had a history of abdominal surgery, and 11 had a history of cancer (Table 1).
DBV in the prone position was measured to be 30.9 mm at L2/3, 23.0 mm at L3/4, and 20.4 mm at L4/5. DBV in the supine position was measured to be 31.5 mm at L2/3, 26.5 mm at L3/4, and 25.5 mm at L4/5. DAV in the prone position was measured to be 44.9 mm at L2/3, 45.1 mm at L3/4, and 44.5 mm at L4/5. DAV in the supine position was measured to be 45.3 mm at L2/3, 47.1 mm at L3/4, and 44.2 mm at L4/5.
ΔDBV was -0.6 mm at L2/3, -3.5 mm at L3/4, and -5.1 mm at L4/5. ΔDAV was -0.4 mm at L2/3, -1.9 mm at L3/4, and 0.3 mm at L4/5 (Table 2).
ΔDBV showed negative values at all levels, indicating posterior displacement of the bowel in the prone position. In contrast, ΔDAV showed minimal change across all levels. Independent significant contributors for ΔDBV at L3/4 were identified as history of abdominal surgeries and being female. Independent significant contributors for ΔDBV at L4/5 were identified as history of cancer and abdominal surgeries (Table 3).
Table 3: Factors affecting ΔDBV in L3/4 and L4/5 identified using multiple regression analysis: p<0.05ΔDBV: the difference between the distance of the bowel to the posterior vertebral lines in prone and supine positions*
Discussion
This study investigated bowel and vascular displacement in the prone position, particularly the differences across lumbar intervertebral levels. The results demonstrated that at all lumbar intervertebral disc levels, the bowel tended to shift posteriorly in the prone position. This observation was contrary to our expectations and the previous report [11]. This unexpected finding suggested that prone positioning may not uniformly promote anterior bowel displacement across all lumbar levels, raising concerns about the generalizability of surgical planning based on assumptions at a single level.
Another significant finding was that the positioning of the major abdominal vessels, such as the aorta, remained relatively stable across different body positions, which corresponded to the previous report [12]. This implies that vascular displacement is minimal and might not be significant in altering the surgical access routes during prone transplant procedures.
Multivariate analysis identified three key patient-related factors that were associated with reduced bowel mobility: female sex, history of cancer, and abdominal surgery. Male patients may experience elevated intra-abdominal pressure that cannot be sufficiently relieved in the prone position, thereby promoting posterior bowel movements. Although previous studies by Kim et al. [13] have reported no significant associations between BMI and movement of abdominal organs, these studies focused on solid organs such as the liver and kidneys rather than the more mobile intestinal tract. Thus, the current study highlights the importance of specifically examining bowel behavior, which may respond differently to positional and pressure changes, in order to mitigate the risk of bowel injury during surgery, which has been reported to have a mortality rate of 13% [14].
Additionally, a prior history of cancer, especially in patients who undergo abdominal radiotherapy or surgical interventions, may affect the flexibility and positioning of the abdominal organs. Radiation-induced fibrosis or postoperative adhesions can anchor portions of the bowel, restricting natural displacement during postural changes. This is supported by the findings of Ganeshan et al., who emphasize the lasting effects of cancer therapies on organ mobility and spatial anatomy [15].
This study has several limitations. First, the small sample size and highly selected cohort of oncologic patients undergoing CT-guided biopsy reduced the statistical power and generalizability of our findings. Second, the absence of a four‑point support system may have had a larger effect on organ position than anticipated, potentially contributing to the observed posterior displacement. Third, variations in the positioning of the bowels and blood vessels due to differences in the respiratory cycle and the fact that prone and supine CT scans were performed on different days were not taken into account.
Conclusions
Although the prone transpsoas approach may offer advantages in lumbar spinal surgery, surgeons should exercise caution, particularly in patients with a history of cancer or abdominal surgery. These populations may have altered intra-abdominal dynamics, which increases the risk of bowel injury. Preoperative imaging in both the supine and prone positions may be considered in selected high-risk patients to optimize surgical planning and safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Extreme Lateral Interbody Fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion Spine J Ozgur BM Aryan HE Pimenta L Taylor WR 435443620061682505210.1016/j.spinee.2005.08.012 · doi ↗ · pubmed ↗
- 2Indirect decompression via oblique lateral interbody fusion for severe degenerative lumbar spinal stenosis: a comparative study with direct decompression transforaminal/posterior lumbar interbody fusion Spine J Shimizu T Fujibayashi S Otsuki B Murata K Matsuda S 9639712120213354012410.1016/j.spinee.2021.01.025 · doi ↗ · pubmed ↗
- 3Indirect decompression through oblique lateral interbody fusion for revision surgery after lumbar decompression World Neurosurg Shimizu T Fujibayashi S Otsuki B Murata K Matsuda S 099141202010.1016/j.wneu.2020.05.15132454196 · doi ↗ · pubmed ↗
- 4Trends in single-level lumbar fusions over the past decade using a national database World Neurosurg Lambrechts MJ Siegel N Heard JC 09167202210.1016/j.wneu.2022.07.09235963610 · doi ↗ · pubmed ↗
- 5Longitudinal trends of patient demographics and morbidity of different approaches in lumbar interbody fusion: an analysis using the American College of Surgeons National Surgical Quality Improvement Program database World Neurosurg Oezel L Okano I Hughes AP 093164202210.1016/j.wneu.2022.04.06735472646 · doi ↗ · pubmed ↗
- 6Single-position prone lateral approach: cadaveric feasibility study and early clinical experience Neurosurg Focus Godzik J Ohiorhenuan IE Xu DS 049202010.3171/2020.6.FOCUS 2035932871564 · doi ↗ · pubmed ↗
- 7Prone lateral lumbar interbody fusion: case report and technical note World Neurosurg Martirosyan NL Uribe JS Randolph BM Buchanan RI 17017714420203289661810.1016/j.wneu.2020.08.172 · doi ↗ · pubmed ↗
- 8The prone transpsoas technique: preliminary radiographic results of a multicenter experience Eur Spine J Pimenta L Amaral R Taylor W 1081133020213247234610.1007/s 00586-020-06471-y · doi ↗ · pubmed ↗