Impact of cancer on outcomes following breakthrough ischaemic stroke on oral anticoagulants for atrial fibrillation: insights from the ASPERA-R study
Matteo Foschi, Federico De Santis, Francesca Gabriele, Lucio D’Anna, Andrea Zini, Matteo Paolucci, Stefano Forlivesi, Ludovica Migliaccio, Maria Maddalena Viola, Angelo Cascio Rizzo, Maria Sessa, Ghil Schwarz, Rachele Tortorella, Soma Banerjee, Gaurav Desai, Muhammad Jaffar

TL;DR
This study shows that cancer, especially active or blood-related cancers, significantly worsens outcomes after a stroke in patients on blood thinners for heart rhythm issues.
Contribution
The study identifies cancer as a major risk factor for poor outcomes after stroke on anticoagulants, with distinct risks for active and remission cancer.
Findings
Cancer patients had a 2.56-fold higher risk of new stroke or TIA within 90 days compared to non-cancer patients.
Active cancer increased the risk of new stroke or TIA by over 4-fold and bleeding by nearly 3-fold.
Haematological cancers posed higher risks for both stroke and bleeding than solid tumors.
Abstract
Breakthrough ischaemic stroke during oral anticoagulation (OAC) for atrial fibrillation (AF) represents a major therapeutic challenge, especially in patients with cancer, who face competing risks of thrombosis and bleeding. This study investigated the impact of cancer on 90-day outcomes after ischaemic stroke on OAC. We analysed patients with AF who experienced ischaemic stroke while on continuous OAC enrolled in the international retrospective ASPERA-R study, comprising 35 stroke centres across 9 countries. Inverse probability weighting was applied to adjust for baseline imbalances, and weighted Cox, ordinal logistic and generalised linear models were used to estimate adjusted 90-day risks for the primary (ischaemic stroke or TIA), secondary (mRS shift, vascular/all-cause death) and safety (moderate-to-severe bleeding, ICH, 24-h haemorrhagic transformation) outcomes. Among 1649…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
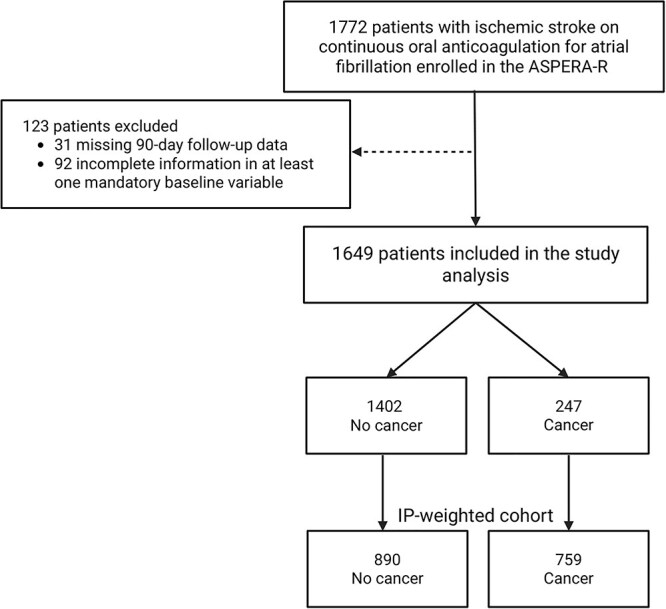 Figure 1
Figure 1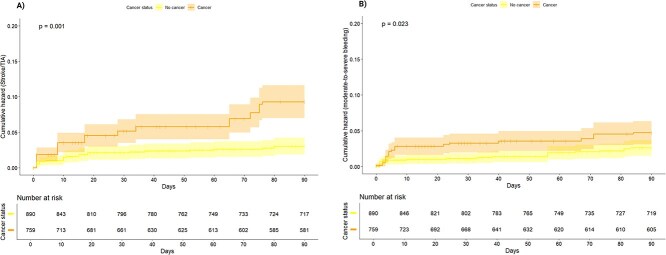 Figure 2
Figure 2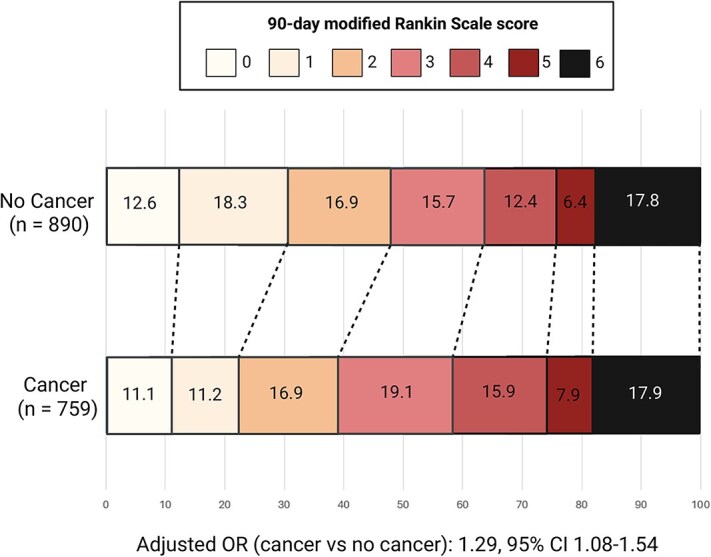 Figure 3
Figure 3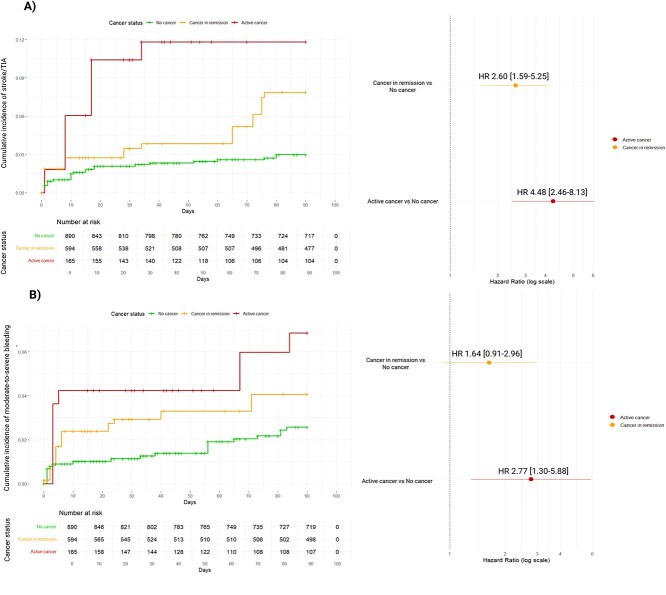 Figure 4
Figure 4|
|
|
|
|
| |
|---|---|---|---|---|---|
|
| |||||
|
| 78.0 ± 10.7 | 79.4 ± 7.9 | 77.7 ± 10.9 | 0.263 |
|
|
| 789 (47.8) | 129 (52.2) | 660 (47.1) | 0.103 | 0.024 |
|
| 0.437 |
| |||
|
| 1,303 (79.0) | 213 (86.2) | 1,090 (77.7) | ||
|
| 113 (6.9) | 23 (9.3) | 90 (6.4) | ||
|
| 24 (1.5) | 1 (0.4) | 23 (1.6) | ||
|
| 9 (0.5) | 1 (0.4) | 8 (0.6) | ||
|
| 200 (12.1) | 9 (3.6) | 191 (13.6) | ||
|
| |||||
|
| 0.012 | 0.036 | |||
|
| 374 (22.7) | 55 (22.3) | 319 (22.8) | ||
|
| 1,275 (77.3) | 192 (77.7) | 1,083 (77.2) | ||
|
| 0.053 | 0.074 | |||
|
| 469/1,275 (36.8) | 71/192 (37.0) | 398/1,083 (36.7) | ||
|
| 428/1,275 (33.6) | 57/192 (29.7) | 371/1,083 (34.3) | ||
|
| 251/1,275 (19.7) | 43/192 (22.4) | 208/1,083 (19.2) | ||
|
| 127/1,275 (10.0) | 21/192 (10.9) | 106/1,083 (9.8) | ||
|
| 0.208 | 0.098 | |||
|
| 653/1,275 (51.2) | 111/192 (57.8) | 542/1,083 (50.0) | ||
|
| 471/1,275 (36.9) | 68/192 (35.4) | 403/1,083 (37.2) | ||
|
| 151/1,275 (11.9) | 13/192 (6.8) | 138/1,083 (12.8) | ||
|
| 1.39 ± 0.54 | 1.40 ± 0.56 | 1.37 ± 0.45 | 0.051 | 0.032 |
|
| 0.030 | 0.080 | |||
|
| 205/374 (54.8) | 29/55 (52.7) | 176/319 (55.2) | ||
|
| 156/374 (41.7) | 26/55 (47.3) | 130/319 (40.8) | ||
|
| 13/374 (3.5) | 0/55 (0.0) | 13/319 (4.0) | ||
|
| 281/1,275 (22.0) | 53/192 (27.6) | 228/1,083 (21.1) | 0.153 | 0.081 |
|
| |||||
|
| 67/281 (23.9) | 11/53 (20.8) | 56/228 (24.6) | 0.065 | 0.004 |
|
| 197/281 (70.1) | 39/53 (73.6) | 158/228 (69.3) | ||
|
| 17/281 (6.0) | 3/53 (5.6) | 14/228 (6.1) | ||
|
| |||||
|
| 1,596 (96.8) | 240 (97.2) | 1,356 (96.7) | 0.026 | 0.003 |
|
| 0.018 | 0.043 | |||
|
| 1,504/1,596 (94.2) | 228/240 (95.0) | 1276/1,356 (94.1) | ||
|
| 42/1,596 (2.6) | 4/240 (1.7) | 38/13,563 (2.8) | ||
|
| 50/1,596 (3.1) | 8/240 (3.3) | 42/1,356 (3.1) | ||
|
| 11 (5–18) | 11 (5–18) | 10 (5–17) | 0.105 | 0.069 |
|
| 0.217 |
| |||
|
| 814 (49.4) | 105 (42.5) | 709 (50.6) | ||
|
| 369 (22.4) | 58 (23.5) | 311 (22.2) | ||
|
| 223 (13.5) | 41 (16.6) | 182 (13.0) | ||
|
| 179 (10.9) | 32 (14.2) | 144 (10.3) | ||
|
| 59 (3.6) | 8 (3.2) | 51 (3.6) | ||
|
| 5 (0.3) | 0 (0.0) | 5 (0.4) | ||
|
| 240 (14.6) | 23 (9.3) | 217 (15.4) | 0.186 | 0.097 |
|
| 139 (8.4) | 18 (7.3) | 121 (8.6) | 0.050 | 0.027 |
|
| 732 (44.4) | 110 (44.5) | 622 (44.4) | 0.003 | 0.019 |
|
| |||||
|
| 1,338 (81.1) | 200 (81.0) | 1,138 (81.2) | 0.003 | 0.026 |
|
| 845 (51.2) | 120 (48.6) | 725 (51.7) | 0.063 | 0.062 |
|
| 443 (26.9) | 49 (19.8) | 394 (28.1) | 0.194 | 0.011 |
|
| 154 (9.3) | 20 (8.1) | 134 (9.6) | 0.051 | 0.058 |
|
| 410 (24.9) | 60 (24.3) | 350 (25.0) | 0.016 | 0.050 |
|
| 27 (1.6) | 6 (2.4) | 21 (1.5) | 0.067 | 0.067 |
|
| 366 (22.2) | 57 (23.1) | 309 (22.0) | 0.025 | 0.088 |
|
| 277 (16.8) | 41 (16.6) | 236 (16.8) | 0.006 | 0.052 |
|
| 268 (16.3) | 48 (19.4) | 220 (15.7) | 0.098 | 0.018 |
|
| 7 (0.4) | 1 (0.4) | 6 (0.4) | 0.004 | 0.001 |
|
| 80 (4.9) | 16 (6.5) | 64 (4.6) | 0.084 | 0.024 |
|
| 94 (5.7) | 15 (6.1) | 79 (5.6) | 0.019 | 0.031 |
|
| 81 (4.9) | 19 (7.7) | 62 (4.4) | 0.137 | 0.006 |
|
| 0.378 |
| |||
|
| 335 (20.3) | 53 (21.5) | 282 (20.1) | ||
|
| 200 (12.1) | 9 (3.6) | 191 (13.6) | ||
|
| 76 (4.6) | 9 (3.6) | 67 (4.8) | ||
|
| 847 (51.4) | 148 (59.9) | 699 (49.9) | ||
|
| 191 (11.6) | 28 (11.3) | 163 (11.6) | ||
|
| 1,310 (79.4) | 194 (78.5) | 1,116 (79.6) | 0.026 | 0.092 |
|
| 742 (45.0) | 111 (44.9) | 631 (45.0) | 0.001 | 0.001 |
|
| 397 (24.1) | 44 (17.8) | 353 (25.2) | 0.180 | 0.015 |
|
| 131 (7.9) | 18 (7.3) | 113 (8.1) | 0.029 | 0.039 |
|
| |||||
|
| 0.164 |
| |||
|
| 179 (10.9) | 25 (10.1) | 179 (12.8) | ||
|
| 463 (28.1) | 62 (25.1) | 463 (33.0) | ||
|
| 201 (12.2) | 23 (9.3) | 201 (14.3) | ||
|
| 283 (17.2) | 42 (17.0) | 283 (27.2) | ||
|
| 112 (6.8) | 18 (7.9) | 112 (8.0) | ||
|
| 179 (10.9) | 27 (7.3) | 179 (12.8) | ||
|
| 59 (3.6) | 16 (5.3) | 59 (4.2) | ||
|
| 36 (2.2) | 11 (4.5) | 36 (2.6) | ||
|
| 19 (1.2) | 3 (1.2) | 19 (1.6) | ||
|
| 8 (0.5) | 0 (0.0) | 8 (0.6) | ||
|
| 110 (6.7) | 20 (8.1) | 110 (7.8) | ||
|
| 8.1 ± 9.1 | 8.6 ± 9.9 | 8.0 ± 8.9 | 0.057 | 0.031 |
|
| 151/1,350 (11.2) | 30/201 (11.5) | 121/1,149 | 0.059 | 0.043 |
|
| 1,346 (81.7) | 208 (84.2) | 1,138 (81.2) | 0.080 | 0.096 |
|
| 1,064 (64.5) | 161 (65.2) | 903 (64.4) | 0.007 | 0.018 |
|
| 387 (23.5) | 43 (17.4) | 344 (24.5) | 0.195 | 0.037 |
|
| 250 (15.2) | 38 (15.4) | 212 (15.2) | 0.001 | 0.018 |
|
|
| ||||||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
| |
|
| |||||||
|
| 20 (8.1) | 37 (2.6) | 62 (8.2) | 25 (2.8) | Adjusted hazard ratio | 2.56 [1.59–4.13] |
|
|
| |||||||
|
| Adjusted odds ratio | 1.29 [1.08–1.54] |
| ||||
|
| 13 (5.3) | 172 (12.3) | 84 (11.1) | 112 (12.6) | |||
|
| 33 (13.4) | 251 (17.9) | 85 (11.2) | 163 (18.3) | |||
|
| 36 (14.6) | 205 (14.6) | 128 (16.9) | 150 (16.9) | |||
|
| 48 (19.4) | 221 (15.8) | 145 (19.1) | 140 (15.7) | |||
|
| 42 (17.0) | 178 (12.7) | 121 (15.9) | 110 (12.4) | |||
|
| 19 (7.7) | 97 (6.9) | 60 (7.9) | 57 (6.4) | |||
|
| 56 (22.7) | 278 (19.8) | 136 (17.9) | 158 (17.8) | |||
|
| 56 (22.7) | 278 (19.8) | 136 (17.9) | 158 (17.8) | Adjusted hazard ratio | 0.98 [0.78–1.24] | .883 |
|
| 31 (12.6) | 184 (13.1) | 82 (10.8) | 101 (11.3) | Adjusted hazard ratio | 0.94 [0.70–1.26] | .677 |
|
| |||||||
|
| 16 (6.5) | 39 (2.8) | 33 (4.3) | 21 (2.4) | Adjusted hazard ratio | 1.82 [1.05–3.14] |
|
|
| 7 (2.8) | 22 (1.6) | 16 (2.1) | 11 (1.2) | Adjusted hazard ratio | 1.66 [0.77–3.58] | .194 |
|
| 35 (14.2) | 252 (18.0) | 125 (16.5) | 158 (17.8) | Adjusted risk difference (%) | 0.2 [−3.8 to 4.2] | .931 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Acute Ischemic Stroke Management · Venous Thromboembolism Diagnosis and Management
Introduction
Over the past decades, major advances in atrial fibrillation (AF) management have substantially improved stroke prevention. Oral anticoagulation (OAC), particularly with the advent of direct oral anticoagulants (DOACs), represents the cornerstone of secondary prevention, significantly reducing ischaemic stroke risk.^1,2^ However, a subset of patients still experiences breakthrough ischaemic strokes despite adequate OAC, remaining at high risk of recurrence. A recent patient-level meta-analysis estimated this residual annual risk at 1.5%–2.5%.^3^ These individuals constitute a distinct and particularly vulnerable phenotype, facing an increased risk of both recurrent ischaemic events and major bleeding, underscoring the need for tailored preventive strategies.^4,5^
In patients with ischaemic stroke, concomitant cancer introduces a therapeutic paradox in which tumour-driven hypercoagulability, endothelial injury and treatment-related haemostatic alterations^6–8^ simultaneously promote thrombosis and predispose to bleeding. In AF patients receiving OAC, this hypercoagulable state may counteract anticoagulant efficacy, increasing the likelihood of breakthrough ischaemia, while cancer and its treatments further heighten bleeding risk.^9,10^ Despite these challenges, breakthrough ischaemic strokes during OAC remain poorly investigated in patients with cancer. Clarifying their characteristics and clinical outcomes is crucial to guide evidence-based management and optimise secondary prevention in this complex population.
Hence, we aimed to assess the impact of cancer on outcomes following breakthrough ischaemic stroke in AF patients on continuous OAC therapy.
Patients and methods
Data availability
The dataset supporting this study will be made available upon reasonable request to the corresponding author.
Study design
ASPERA is a large multicentre observational study coordinated by the University of L’Aquila, comprising a retrospective (ASPERA-R) and a prospective (ASPERA-P) arm. This analysis reports data from ASPERA-R, including 35 stroke centres across 9 European and North African countries (Appendix S1). The ASPERA-P arm is ongoing. The study followed STROBE reporting guidelines.^11^
Study population
ASPERA-R consecutively enrolled adults (≥18 years) with AF who experienced a breakthrough ischaemic stroke while on continuous OAC between February 2020 and February 2025. All hospital admissions and emergency evaluations during this period were screened. Stroke diagnosis followed WHO criteria and was confirmed by NCCT or MRI. Continuous OAC use was confirmed based on prescription records and corroborated by patient or caregiver report of uninterrupted treatment during the 7 days prior to the index event, with documented last intake within 48 h of stroke onset.
Data collection and definitions
Clinical data were retrieved from hospital records and standardised follow-up visits, supplemented by direct contact when needed. Only patients with complete 90-day follow-up and no missing mandatory baseline variables were included. The full list of both mandatory and optional baseline variables is provided in Appendix S2. Data were entered via a standardised REDCap case report form and centrally validated through weekly quality checks. The final dataset was locked on 1 September 2025.
Patients were classified as with or without cancer. Those with cancer were further categorised as active or in remission. Active cancer was defined using binary clinical information available in the registry (yes/no): (1) diagnosis within 6 months before or during the index hospitalisation; (2) receipt of cancer-directed therapy (radiotherapy, chemotherapy, hormonal therapy or surgery) within 6 months or (3) recurrence or metastasis within 6 months. Cancer in remission referred to a prior malignancy not fulfilling active cancer criteria. Importantly, the ASPERA-R registry did not collect detailed oncological data such as cancer stage (eg, tumour–node–metastasis [TNM] classification), specific treatment regimens, treatment timing/intensity or extent of metastatic disease. Cancer status was determined by the treating physician; no systematic screening for occult malignancies was performed.
Study outcomes
The primary outcome was the 90-day risk of new ischaemic stroke or TIA. Secondary outcomes included the 90-day ordinal shift in mRS score; 90-day incidence all-cause and vascular death (any death attributable to cardiovascular or cerebrovascular causes, including fatal ischaemic or haemorrhagic stroke, sudden cardiac death, myocardial infarction or other vascular events). Safety outcomes included 90-day moderate-to-severe bleeding, ICH and 24-h haemorrhagic transformation (HT). Bleeding severity was categorised according to the Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Artery (GUSTO) trial classification.^12^ Specifically, moderate-to-severe bleeding was defined as any haemorrhagic event ranging from those requiring blood transfusion to life-threatening or fatal bleeding, including ICH or bleeding necessitating surgical intervention, fluid replacement or inotropic support. Haemorrhagic transformation was defined according to the Heidelberg Bleeding Classification system.^13^
Statistical analysis
Categorical variables were expressed as counts (percentages) and continuous variables as means (SD) or medians (IQR). To minimise baseline imbalances between groups, inverse probability weighting (IPW) based on propensity scores was applied using logistic regression including prespecified variables (age, sex, ethnicity, enrolling centre, vascular risk factors, AF type, baseline NIHSS and mRS scores, concomitant large-artery atherosclerosis and reperfusion therapies). Stabilised weights were used to limit extreme values, and covariate balance was verified through standardised mean differences (SMDs) and visual inspection of score covariate balance graphs. Primary and secondary analyses were performed in the weighted cohort, with further adjustment for residual imbalances. The primary outcome was evaluated with weighted Cox regression models, providing adjusted hazard ratios (aHRs) and 95% CIs. Secondary outcomes were analysed with ordinal logistic regression for 90-day mRS and weighted Cox models for mortality. Safety endpoints (24-h haemorrhagic transformation, 90-day bleeding and ICH) were assessed using generalised linear or Cox models. Death was treated as a competing risk for recurrent ischaemic events, with cumulative incidences compared by Gray’s test and Fine–Gray regression. Proportional hazards assumptions were checked via Schoenfeld residuals, and Kaplan–Meier curves illustrated time-to-event outcomes. All eligible patients were included without formal sample size estimation. Analyses were conducted in R (v4.4.1), with 2-sided P < .05 considered significant.
Results
A total of 1649 patients were included, of whom 247 (15.0%) had cancer (mean age 78.0 ± 10.7 years). The ASPERA-R flowchart with excluded cases is shown in Figure 1. Among cancer patients, 87/247 (35.2%) had active cancer and 160/247 (64.8%) cancer in remission. Cancer sites were gastrointestinal 48/247 (19.4%), lung 20/247 (8.1%), genitourinary 64/247 (25.9%), breast 47/247 (19.0%), haematological 30/247 (12.2%), skin 15/247 (6.1%) and other 23/247 (9.3%). Metastatic disease was present in 29/247 (11.7%), involving lymph nodes in 7/29 (24.1%), bone 5/29 (17.2%), liver 5/29 (17.2%), lung 5/29 (17.2%) and multiple sites 3/29 (10.3%). No patient had a primary or secondary tumour of the central nervous system. Unweighted characteristics are summarised in Table 1.
Study flow-chart of the ASPERA-R study. Abbreviations: IP = inverse probability.
Inverse probability weighting
After IPW, the weighted cohort (pseudopopulation) comprised 759 patients with cancer and 890 without. No missing data were present for propensity score variables. Balance diagnostics indicated adequate matching, with an SMD of 0.19 (<0.25) and a variance ratio of 1.01 (0.5–2.0).^14^ Visual inspection and covariate-balance plots confirmed the good overlap (Figures S1 and S2). Weighted baseline characteristics showed SMD < 0.10 across most variables (Table 1).
Primary outcome
In the unweighted cohort, 90-day ischaemic stroke or TIA occurred in 20 (8.1%) cancer and 37 (2.6%) non-cancer patients. After weighting and adjustment, the 90-day risk remained significantly higher in cancer (8.2% vs 2.8%; aHR 2.56; 95% CI, 1.59–4.13; P < .001) (Table 2; Figure 2A). In competing-risk analysis, the cumulative incidence differed by cancer status (Gray’s test χ^2^ = 23.6; P < .001), and Fine–Gray regression confirmed higher subdistribution hazard (SHR 2.97; 95% CI, 1.87–4.72; P < .001). Death as competing event was not different (P = .379) (Figure S3).
Kaplan–Meier cumulative estimates of (A) 90-day new ischaemic stroke or TIA and (B) 90-day moderate-to-severe bleeding by cancer status in the weighted cohort. p: log-rank test P-value. Dashed areas indicate 95% CIs.
Secondary outcomes
As shown in Table 2, patients with cancer had a significantly higher 90-day disability burden compared to those without cancer (adjusted odds ratio 1.29; 95% CI, 1.08–1.54; P = .005) (Figure 3), while 90-day all-cause and vascular mortality did not differ between groups.
90-day mRS ordinal shift in the weighted cohort.
Safety outcomes
Moderate-to-severe bleeding occurred in 16 (6.5%) cancer and 39 (2.8%) non-cancer patients in the unweighted cohort. In the weighted analysis, cancer remained associated with higher 90-day bleeding risk (4.3% vs 2.4%; aHR 1.82; 95% CI, 1.05–3.14; P = .033) (Table 2; Figure 2B). Among cancer patients, 8/15 (53.3%) bleeding events were extracranial and 7/15 (46.7%) intracranial, with no differences vs non-cancer. The 24-h haemorrhagic transformation risk was similar (Table 2).
Active cancer and cancer in remission versus no cancer
Compared with non-cancer, patients with active cancer had higher 90-day risks of ischaemic stroke/TIA (HR 4.48; 95% CI, 2.46–8.13; P < .001) and bleeding (HR 2.77; 95% CI, 1.30–5.88; P = .008). Those with cancer in remission had elevated ischaemic risk (HR 2.60; 95% CI, 1.59–5.25; P = .001) but similar bleeding risk (HR 1.64; 95% CI, 0.91–2.96; P = .103) (Table S1; Figure 4).
Kaplan–Meier cumulative estimates of (A) 90-day new ischaemic stroke or TIA and (B) 90-day moderate-to-severe bleeding in patients with active cancer, cancer in remission vs no cancer in the weighted cohort. Panels on the right indicate the HR (95% CIs) for 90-day new ischaemic stroke or TIA (A) and moderate-to-severe bleeding in respect to patients without cancer. Abbreviation: HR = hazard ratio.
Haematological versus solid malignancies
In the weighted cohort, haematological cancers carried a higher 90-day risk of ischaemic recurrence (HR 3.06; 95% CI, 1.69–5.54; P = .001) and bleeding (HR 3.47; 95% CI, 1.57–7.70; P = .006) compared with solid tumours (Table S2; Figure S4).
Discussion
In this multicentre cohort of patients with AF who experienced ischaemic stroke during continuous OAC, cancer was associated with a higher 90-day risk of recurrent ischaemic stroke or TIA, worse functional outcome and increased moderate-to-severe bleeding compared with patients without cancer. Patients with active cancer exhibited over a 4-fold higher risk of ischaemic recurrence and nearly 3-fold higher risk of moderate-to-severe bleeding, whereas those in remission showed an elevated risk of recurrent cerebral ischaemia only. Haematological malignancies were associated with markedly higher risks of both ischaemic and haemorrhagic events compared with solid tumours. Overall, these findings identify cancer as a key modifier of prognosis in AF patients with breakthrough stroke on OAC, underscoring the need for tailored secondary prevention strategies to balance competing ischaemic and bleeding risks.
The higher 90-day risk of recurrent ischaemic stroke or TIA among patients with cancer compared with those without suggests that malignancy amplifies thromboembolic burden despite OAC. This is biologically plausible, as cancer-related prothrombotic mechanisms, tumour-derived factors, anticancer therapies, platelet activation and coagulation cascade upregulation, promote thrombogenesis.^6–8^ Endothelial injury further enhances platelet adhesion via von Willebrand factor release, while many anticancer drugs alter CYP3A4 and P-glycoprotein activity, reducing DOAC exposure and efficacy.^9^ These mechanisms may attenuate OAC protection and explain recurrent ischaemic events.^8^ In our cohort, 89.1% resumed anticoagulation after stroke, without differences by cancer status. Although causality cannot be inferred, these findings suggest cancer may contribute both to index and recurrent strokes, reinforcing the need for integrated prevention strategies addressing cancer-related hypercoagulability.
Evidence on secondary prevention after breakthrough ischaemic stroke in cancer patients on OAC is scarce. Available data, mostly from embolic stroke of unknown source (ESUS) populations, indicate comparable recurrence rates between anticoagulants and antiplatelets. A retrospective study of 263 patients with active cancer showed no difference in thromboembolic recurrence between the 2 treatments.^15^ Similarly, the ARCADIA post hoc analysis (137 ESUS patients with prior cancer) and the NAVIGATE ESUS subanalysis reported similar efficacy between apixaban or rivaroxaban and aspirin.^16,17^ In our cohort, even patients with prior (remitted) cancer had a higher recurrence risk than non-cancer patients, though lower than those with active malignancy. This gradient suggests that the prothrombotic state may persist beyond active disease, warranting long-term vigilance and optimisation of preventive therapy.
Regarding safety outcomes, active cancer patients had an approximately 3-fold higher 90-day risk of moderate-to-severe bleeding, mostly extracranial, mainly driven by patients with haematological malignancies, who showed the highest risk for both moderate-to-severe bleeding and ischaemic recurrence. This pattern aligns with previous evidence^18^ and likely reflects the profound haemostatic dysregulation characteristic of haematological cancers, including coagulopathy, thrombocytopenia and, in severe cases, evolution towards disseminated intravascular coagulation.^19–21^ Furthermore, haematological cancer therapies may amplify both venous and arterial thromboembolic risk or accelerate atherosclerotic processes,^19–21^ creating a particularly unfavourable balance between ischaemic and haemorrhagic complications in anticoagulated patients.^22,23^ In contrast, solid tumours may contribute to bleeding risk through both local and systemic mechanisms: tumour invasion and neovascularisation generate fragile vasculature, while systemic coagulopathy, treatment-related thrombocytopenia and endothelial dysfunction impair haemostasis.^24^ In anticoagulated patients, these alterations, together with drug–drug interactions and fluctuating renal or hepatic function, can modify anticoagulant metabolism, narrowing the therapeutic window and further predisposing to bleeding.^22,23^
The main strength of this study lies in the rigorous data verification and systematic quality checks of the ASPERA-R database, its large sample size and the use of advanced statistical methods providing robust outcome estimates. However, several limitations must be acknowledged. First, despite IPW adjustment, residual confounding cannot be excluded given the observational design. Second, the retrospective nature may have introduced selection or measurement bias and precludes causal inference; some cases managed outside the stroke unit or with alternative discharge diagnoses may have been missed. Third, DOAC plasma levels were available for only ~ 20% of patients, limiting assessment of treatment exposure; estimates based on clinical data may have led to misclassification, and time on therapeutic INR was unavailable for VKA users. Fourth, resumption of OAC after the index stroke was incomplete: among those who did not restart anticoagulation (10.9%), most died during the index hospitalisation or had severe in-hospital bleeding, and in a minority no clear clinical reason was identifiable. This may have influenced both thromboembolic and bleeding outcomes and represents an additional potential source of residual confounding. Fifth, 6.9% of patients with incomplete data were excluded, although attrition appeared nondifferential, selection bias remains possible. Sixth, although receipt of cancer-directed therapy and the presence of recurrence or metastasis were collected in binary form to classify active cancer, detailed information on cancer stage, specific therapeutic regimens and extent of metastatic disease was not available, limiting assessment of how these features may influence OAC exposure and outcomes. This is relevant because bleeding risk (elevated in cancers such as melanoma or renal cell carcinoma) and thromboembolic risk (notably increased in advanced lung or pancreatic cancer) vary substantially by tumour type.^8,24^ Furthermore, assessing the effect of specific cancer subtypes on ischaemic recurrence is inherently challenging, as this would require very large sample sizes to support adequately powered subgroup analyses. Lastly, advanced disease, chemotherapy-related cytopenias, frailty and cachexia, key modifiers of thrombotic and haemorrhagic risk, were not systematically captured and may have attenuated, though not reversed, the observed associations. In addition, as this study is a predefined secondary analysis of the ASPERA-R registry, which was designed to capture major cardiovascular effectiveness outcomes and bleeding, systematic data on venous thromboembolism were not collected, thereby preventing a reliable risk assessment despite it may influence antithrombotic management in patients with cancer. Moreover, undiagnosed cancers in the no-cancer group cannot be ruled out, as systematic screening was not performed. Similarly, limited data on metastatic disease precluded reliable assessment of its impact. Finally, since ~ 60% of patients were enrolled in Italy and most were non-Hispanic White, generalisability to other populations may be limited.
In conclusion, cancer significantly alters the prognosis of patients experiencing ischaemic stroke despite OAC, increasing short-term risks of both recurrent ischaemia and major bleeding, particularly in those with active or haematological malignancies. These results emphasise the delicate interplay between hypercoagulability, treatment-related haemostatic changes and anticoagulant safety, underscoring the need for refined risk assessment and individualised management. Future prospective studies should clarify the mechanisms underlying anticoagulation failure in cancer and define evidence-based strategies for secondary prevention to support precision antithrombotic therapy and improve outcomes in this high-risk population.
Supplementary Material
aakag015_SUPPLEMENTAL_ASPERA_CANCER_final
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. 2021;52:e 364-e 467. 10.1161/STR.000000000000037534024117 · doi ↗ · pubmed ↗
- 2Dawson J, Béjot Y, Christensen LM, et al. European Stroke Organisation (ESO) guideline on pharmacological interventions for long-term secondary prevention after ischaemic stroke or transient ischaemic attack. Eur Stroke J. 2022;7:I-XLI. 10.1177/23969873221100032 PMC 944632436082250 · doi ↗ · pubmed ↗
- 3Johnson LS, Benz AP, Shoamanesh A, et al. Residual stroke risk among patients with atrial fibrillation prescribed oral anticoagulants: a patient-level meta-analysis from COMBINE AF. J Am Heart Assoc. 2024;13:e 034758. 10.1161/JAHA.123.03475839190578 PMC 11646504 · doi ↗ · pubmed ↗
- 4D’Anna L, Filippidis FT, Harvey K, et al. Ischemic stroke in oral anticoagulated patients with atrial fibrillation. Acta Neurol Scand. 2022;145:288-296. 10.1111/ane.1355234766621 · doi ↗ · pubmed ↗
- 5Sakamoto Y, Okubo S, Nito C, et al. The relationship between stroke severity and prior direct oral anticoagulant therapy in patients with acute ischaemic stroke and non-valvular atrial fibrillation. Eur J Neurol. 2017;24:1399-1406. 10.1111/ene.1340528799181 · doi ↗ · pubmed ↗
- 6Kawano T, Mackman N. Cancer patients and ischemic stroke. Thromb Res. 2024;237:155-162. 10.1016/j.thromres.2024.03.01938603819 · doi ↗ · pubmed ↗
- 7Dardiotis E, Aloizou AM, Markoula S, et al. Cancer-associated stroke: pathophysiology, detection and management (review). Int J Oncol. 2019;54:779-796. 10.3892/ijo.2019.466930628661 PMC 6365034 · doi ↗ · pubmed ↗
- 8Heo JH, Yun J, Kim KH, et al. Cancer-associated stroke: thrombosis mechanism, diagnosis, outcome, and therapeutic strategies. J Stroke. 2024;26:164-178. 10.5853/jos.2023.0327938836266 PMC 11164583 · doi ↗ · pubmed ↗