Impact of anaemia severity on functional outcome in patients with cerebral venous thrombosis: a DOAC-CVT substudy
Nada M Sobih, Jelle Vellema, Anita van de Munckhof, Mayte Sanchez van Kammen, Xunming Ji, Ido van den Wijngaard, Jeremy Molad, Marialuisa Zedde, Y Muralidhar Reddy, Mohammad Wasay, Antonio Arauz, Mirjam Heldner, Nesrin Ergin, Miguel A Barboza, Diana Aguiar de Sousa

TL;DR
This study found that moderate to severe anemia at admission predicts worse recovery in patients with cerebral venous thrombosis.
Contribution
The study is the first to show that anemia severity correlates with poor outcomes in cerebral venous thrombosis patients.
Findings
Anaemia was associated with poor functional outcome (mRS 3–6) in CVT patients.
Moderate to severe anaemia had a stronger association with poor outcomes than mild anaemia.
Anaemia was not significantly linked to mortality in CVT patients.
Abstract
Anaemia is an established risk factor for poor outcome in intracerebral haemorrhage and ischaemic stroke. We examined whether anaemia predicts poor outcome in cerebral venous thrombosis (CVT). We used data of the DOAC-CVT study, which was an international, prospective observational cohort study in adult patients with CVT that ran from January 2021 to January 2024. Anaemia at admission was defined according to World Health Organization criteria. Poor outcome was defined as modified Rankin Scale (mRS) 3–6 at 6-months. Binary logistic regression, adjusted for age, recent delivery/puerperium, income country, cancer and intracranial haemorrhage, was applied. Of 619 patients in DOAC-CVT, 583 patients were included, of whom 157 (27%) had anaemia. Compared to patients without anaemia, patients with anaemia were slightly younger (median age 40 vs. 42 years), more often female (76% vs. 59%),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
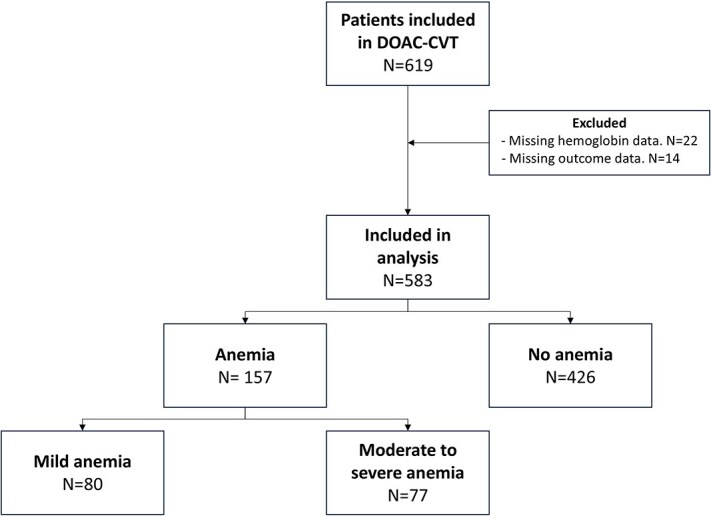 Figure 1
Figure 1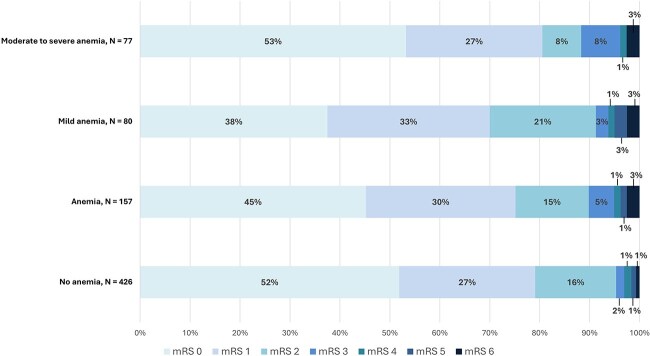 Figure 2
Figure 2|
|
|
| |
|---|---|---|---|
|
| |||
| Age, median (IQR), years | 42 (29–53) | 40 (27–48) | .011 |
| Female sex | 250/426 (58.7) | 120/157 (76.4) | <.001 |
| Country of inclusion’s income group | |||
| High-income country | 264/332 (79.5) | 68/332 (20.5) | <.001 |
| Middle-income country | 162/251 (64.5) | 89/251 (35.5) | |
| Risk factors | |||
| Oral contraceptives | 116/250 (46.4) | 35/120 (29.2) | .243 |
| Recent delivery, puerperium | 11/250 (4.4) | 9/120 (7.5) | .217 |
| Other prothrombotic medication | 28/426 (6.6) | 6/157 (3.8) | .238 |
| Head or neck infection | 29/426 (6.8) | 17/157 (10.8) | .120 |
| CNS infection | 5/426 (1.2) | 4/157 (2.5) | .260 |
| Cancer | 8/426 (1.9) | 7/157 (4.5) | .135 |
| Autoimmune disease | 18/426 (4.2) | 16/157 (10.2) | .009 |
| Known APS or presence of antiphospholipid antibodies at baseline | 36/426 (8.5) | 12/157 (7.6) | .866 |
| Previous VTE | 33/426 (7.7) | 8/157 (5.1) | .283 |
| Previous major bleeding | 6/426 (1.4) | 7/157 (4.5) | .050 |
| No risk factor identified | 155/426 (36.4) | 33/157 (21.0) | <.001 |
| Pre-morbid mRS 3–6 | 12/426 (2.8) | 10/157 (6.4) | .043 |
|
| |||
| Time from symptom onset to diagnosis, median (IQR), days | 4 (1–11) | 3 (1–10.75) | .577 |
| Headache | 383/426 (89.9) | 140/157 (89.2) | .878 |
| Focal neurologic deficits | 153/426 (35.9) | 84/157 (53.5) | <.001 |
| Seizure | 117/426 (27.5) | 46/157 (29.3) | .678 |
| GCS, median (IQR) | 15 (15–15) | 15 (13–15) | <.001 |
| Coma | 10/426 (2.3) | 8/157 (5.1) | .106 |
|
| |||
| Location thrombosis | |||
| Superior sagittal sinus | 214/426 (50.2) | 67/157 (42.7) | .113 |
| Straight sinus | 70/426 (16.4) | 19/157 (12.1) | .243 |
| Deep venous system | 31/426 (7.3) | 10/157 (6.4) | .722 |
| Cortical vein | 98/426 (23.0) | 32/157 (20.4) | .505 |
| Number of thrombosed sinuses, median (IQR) | 3 (2–4) | 3 (2–4) | .340 |
| Non-haemorrhagic lesion | 94/426 (22.1) | 43/157 (27.4) | .187 |
| Intracranial haemorrhage | 134/426 (31.5) | 76/157 (48.4) | <.001 |
|
| |||
| White blood cell, 109/L | 9.0 (7.0–11.2) | 9.7 (7.0–13.0) | .125 |
| Platelet count, 109/L | 254.5 (209.8–311.2) | 302.0 (231.3–399.5) | <.001 |
| C-reactive protein, mg/L | 5.81 (2.00–16.70) | 9.21 (3.00–41.10) | .002 |
| Renal function (eGFR) mL/min/1.73 m2 | 94.0 (81.0–112.0) | 100.0 (85.5–120.1) | .057 |
| Creatinine (mg/dL) | 1.17 (0.80–1.20) | 0.85 (0.61–0.85) | <.001 |
|
| |||
| Lead-in parenteral anticoagulants | 394/426 (92.5) | 146/157 (93.0) | .862 |
| Endovascular treatment | 21/426 (4.9) | 7/157 (4.5) | .834 |
| Decompressive neurosurgery | 4/426 (0.9) | 8/157 (5.1) | .004 |
| Intensive care unit admission | 67/426 (15.7) | 37/157 (23.6) | .038 |
|
|
|
| ||
|---|---|---|---|---|
|
|
| |||
|
| 20/426 (4.7%) | 16/157 (10.2%) | 2.30 (1.16–4.57) | 2.20 (1.01–4.81) |
|
| 3/426 (0.7%) | 4/157 (2.5%) | 3.67 (0.82–16.66) | 3.54 (0.68–18.31) |
|
|
|
| ||
|---|---|---|---|---|
|
|
| |||
|
| ||||
| Mild anaemia | 73/547 (13.3%) | 7/36 (19.4%) | 1.95 (0.80–4.77) | 1.64 (0.60–4.55) |
| Moderate–severe anaemia | 68/547 (12.4%) | 9/36 (25.0%) | 2.69 (1.17–6.15) | 2.88 (1.14–7.38) |
- —Netherlands Thrombosis Foundation10.13039/501100012028
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebral Venous Sinus Thrombosis · Vascular Malformations Diagnosis and Treatment · Venous Thromboembolism Diagnosis and Management
Introduction
Cerebral venous thrombosis (CVT) is an uncommon cerebrovascular disease, affecting approximately 1–2 per 100 000 individuals annually.^1^ Although the prognosis of CVT is favourable in many patients, a minority experiences persistent functional impairment or fatal outcomes.^2^ Several clinical variables that predict poor outcome have been previously identified in patients with CVT, including intracranial haemorrhage, thrombosis of the deep venous system, decreased consciousness, older age, coma and cancer.^3–6^
Anaemia is present in 7%–27% of patients with CVT at diagnosis and has previously been identified as an independent risk factor for disease occurrence.^2,7,8^ More recently, anaemia has also been recognized as a predictor of poor outcome in other cerebrovascular diseases, such as ischaemic and haemorrhagic stroke.^9–11^ The impact of anaemia on clinical outcomes is thought to be related to impaired oxygen delivery, heightened inflammatory responses, altered blood viscosity and decreased physiological reserve.^12–17^ Similar pathophysiological mechanisms might underlie an association between anaemia and poor outcomes in CVT.
To date, only 2 studies have investigated the relationship between anaemia and outcomes after CVT.^18,19^ In both studies, anaemia was associated with worse clinical outcomes, with the strongest associations seen in patients with moderate to severe anaemia. Both studies were predominantly retrospective in nature and had limited sample size. The aim of the current study was to investigate whether anaemia at baseline is associated with poor functional outcomes in patients with CVT, using data from a large international prospective cohort study.
Patients and methods
Study design and population
We performed a post hoc analysis of the DOAC-CVT study. DOACT-CVT was a prospective, international, observational cohort designed to investigate the effectiveness and safety of direct oral anticoagulants (DOACs) compared to vitamin K antagonists (VKAs) in adult patients with CVT. The study protocol and primary results of the study have been published.^20,21^ The study was conducted in 65 hospitals, across 23 countries on 5 continents. Patients could be included if they were 18 years or older, if CVT was radiologically confirmed, and if oral anticoagulant therapy (either DOAC or VKA) had been started within 30 days of diagnosis. Exclusion criteria were the use of anticoagulation before CVT diagnosis, pregnancy or breast feeding and a contraindication to DOACs.^21^ For this substudy, we additionally excluded patients for whom baseline haemoglobin or follow-up data on functional recovery were missing. Detailed baseline data were collected and patients were followed up at 3 and 6 months after diagnosis. All data were entered in an electronic data capture system (Castor EDC). All participants or their immediate family members provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines, and was approved by relevant ethics committees and regulatory authorities in each participating country.
Haemoglobin assessment, anaemia classification and outcomes
Haemoglobin concentration was measured at hospital admission as part of routine clinical care. Values were converted to millimoles per litre (mmol/L) when necessary. Anaemia was defined according to World Health Organization criteria as a haemoglobin level of <8.1 mmol/L (<13.0 g/dL) in men and <7.5 mmol/L (<12.0 g/dL) in women. For subgroup analyses, anaemia severity was classified as mild (6.8–8.0 mmol/L [11–12.9 g/dL] in men; 6.8–7.4 mmol/L [11–11.9 g/dL] in women) or moderate to severe (<6.8 mmol/L [<11 g/dL] for both men and women).^22^
The primary outcome was poor functional outcome at 6-months follow-up, assessed using the modified Rankin Scale (mRS). A score of 0 on the mRS indicates no symptoms; 1, no significant disability; 2, slight disability; 3, moderate disability; 4, moderately severe disability; 5, severe disability requiring constant care; and 6, death.^23^ Outcomes were dichotomized into favourable (mRS 0–2) and unfavourable (mRS 3–6).
Statistical analysis
Baseline characteristics were compared between anaemic and non-anaemic patients. Categorical variables are reported as frequencies (%) and compared using Chi-squared or Fisher’s exact test, as appropriate. Continuous variables are presented as means with standard deviation or median (interquartile range, IQR), depending on distribution, and were compared using t-tests or Mann–Whitney U tests.
To assess the relationship between anaemia and unfavourable outcome, three binary logistic regression models were used: The first model assessed the impact of anaemia as a dichotomous variable (anaemic vs. non-anaemic) on the likelihood of an unfavourable outcome (mRS 3–6). The second model investigated the association between haemoglobin levels as a continuous variable and unfavourable outcomes (mRS 3–6). The third model examined the impact of anaemia as a dichotomous variable on the 6-month mortality rate.
For further analysis, two multivariate ordinal regression models were conducted to evaluate the impact of anaemia across the entire spectrum of mRS scores (0–6). Two separate models were used assessing haemoglobin as a continuous variable and anaemia status as a categorical variable (anaemic vs. non-anaemic).
We conducted two sensitivity analyses. In the first, patients with cancer were excluded. Cancer was defined as active malignancy requiring treatment or cancer diagnosed within 6 months prior to the CVT event. In the second sensitivity analysis, to account for baseline functional status, patients with a premorbid mRS score greater than 2 were excluded. In addition, subgroup analyses were conducted according to anaemia severity (mild and moderate to severe), gender and clinical subgroups typically associated with anaemia, including young women of reproductive age (18–50), older patients (>65 years) and patients with cancer or autoimmune diseases, using binary logistic regression.
All models were adjusted for age, recent delivery, country income level, intracranial haemorrhage and cancer. In the subgroup analyses, the variables cancer, recent delivery and age were omitted when they overlapped with the defining characteristic of the subgroup, such as in analyses of cancer patients, young women, men and older patients.^2,24^ Missing data were handled by complete-case analysis. Odds ratios (ORs) with corresponding 95% CIs were reported, and a 2-sided P-value <.05 was considered statistically significant. Analyses were performed using IBM SPSS Statistics version 24 (IBM Corp., Armonk, NY, USA).
Results
Between January 2021 and January 2024, 619 patients with CVT were enrolled in the DOAC-CVT study. Of these, 36 patients were excluded because of missing baseline haemoglobin levels (22) or follow-up data (14), leaving 583 patients for analysis. Of these, 157 (26.9%) had anaemia at baseline and 426 (73.1%) did not. Among those with anaemia, 80 patients (13.7%) had mild anaemia and 77 patients (13.2%) had moderate to severe anaemia (Figure 1). In total, 332 patients (57.1%) were from high-income countries and 251 patients (43.1%) were from middle-income countries.
Flowchart of patient inclusion. This figure illustrates the inclusion and exclusion process for the study cohort. It further categorizes patients into anaemic and non-anaemic groups, with anaemia severity further stratified into mild and moderate to severe categories. Abbreviation: CVT = cerebral venous thrombosis.
Median haemoglobin level was 6.8 mmol/L (IQR 5.5–7.3) in the anaemic group and 8.8 mmol/L (IQR 8.3–9.5) in the non-anaemic group. Anaemic patients were younger (median age 40 vs. 42 years, P = .01), more often female (76.4% vs. 58.7%, P < .01), and more frequently from middle-income countries (35.5% vs. 20.5%; P < .001). Cancer (4.5% vs. 1.9%, P = .14) and auto-immune disease (10.2 vs 4.2%, P < .01) were more prevalent in patients with anaemia. Anaemic patients presented more frequently with focal neurological deficits (53.5% vs. 35.9%, P < .01), lower Glasgow Coma Scale scores (median: 14 [IQR: 13–15] vs. 15 [IQR: 15–15], P < .01), and intracranial haemorrhage (48.4% vs. 31.5%, P < .01; Table 1).
After 6-months follow-up, 547 patients (93.8%) had a favourable functional outcome (mRS 0–2) and 36 patients (6.2%) a unfavourable outcome (mRS 3–6). Both unfavourable functional outcome (10.2% vs. 4.7%, P = .01) and mortality (2.5% vs. 0.7%, P = .07) were more common among patients with anaemia than those without anaemia (Figure 2). After adjustment, the presence of anaemia was associated with an increased risk of unfavourable functional outcome (mRS 3–6; aOR: 2.20, 95% CI, 1.01–4.81; Table 2). When anaemia was modelled as a continuous variable, lower haemoglobin levels were also associated with unfavourable outcomes (aOR per one mmol/L increase in haemoglobin: 0.75, 95% CI, 0.61–0.93). Ordinal regression analysis indicated that anaemia was statistically non-significant associated with a shift toward worse functional outcomes across the full mRS spectrum (aOR: 1.43, 95% CI, 0.99–2.05). This finding was consistent when haemoglobin was analysed as continuous variable (aOR per one mmol/L increase in haemoglobin: 0.92; 95% CI, 0.83–1.02). In addition, mortality was nominally higher among anaemic patients but this difference was not statistically significant (aOR: 3.54, 95% CI, 0.68–18.31; Table 2).
Stacked distribution of modified Rankin scale outcomes at 6 months across anaemia categories. This figure illustrates the stacked bar chart of mRS scores at 6-moths follow-up for each anaemia category (no anaemia, anaemia, mild anaemia, moderate-to-severe anaemia). For each mRS score, the corresponding percentage is indicated within the bars. Notably, no patients in the moderate to severe anaemia group had a mRS score of 5. Abbreviation: mRS = modified Rankin scale.
The prevalence of unfavourable functional outcome at 6-months increased with anaemia severity and was 4.7% in patients without anaemia, 8.8% in those with mild anaemia and 11.7% in those with moderate to severe anaemia (Figure 2). Moderate to severe anaemia was associated with mRS 3–6 (aOR: 2.88, 95% CI, 1.14–7.38; P = .03), whereas mild anaemia was not (aOR: 1.64, 95% CI, 0.60–4.55; P = .35; Table 3). The presence of anaemia, irrespective of severity, showed a statistically significant association with unfavourable functional outcome (mRS 3–6) in women (aOR: 3.61, 95% CI, 1.04–8.82; P = .03) but not in men (aOR: 2.13; 95% CI, 0.54–8.30; P = .28). In the subgroups of patients with cancer or autoimmune disease (aOR: 1.16; 95% CI, 0.19–7.07; P = .88), and older patients (aOR: 1.09; 95% CI, 0.23–5.19; P = .91), anaemia showed no significant association with unfavourable functional outcome. Among young women, the presence of anaemia was associated with a statistically non-significant trend toward unfavourable functional outcomes (aOR 4.28; 95% CI, 0.95–19.18; P = .06).
In a sensitivity analysis excluding patients with cancer (n = 15), anaemia remained associated with unfavourable outcome (aOR: 2.34; 95% CI, 1.02–5.39; P = .045). In the sensitivity analysis excluding patients with a premorbid mRS score higher than 2 (n = 22) and with haemoglobin modelled as continuous variable, the association with unfavourable outcome remained significant (aOR per one mmol/L increase in haemoglobin: 0.76, 95% CI, 0.60–0.97). When modelled as a dichotomous variable, anaemia was associated with higher odds of unfavourable functional outcome (aOR 1.86; 95% CI, 0.75–4.62), though this association was no longer statistically significant.
Discussion
In this post hoc analysis of the DOAC-CVT study, anaemia was present at baseline in approximately one in four patients with CVT. The presence of anaemia was independently associated with poor functional outcome (mRS 3–6) at follow-up. The strongest prognostic effect was present in moderate to severe anaemia.
The rate of anaemia is consistent with previous studies, which reported rates ranging from 22% to 27%.^7,25^ The strength of association between the dichotomized anaemia and poor outcome (aOR 2.2) is also in line with findings from Silvis et al. and Kai Liu et al. (aORs 2.4 and 3.0, respectively) (14, 15). In contrast, mortality rates varied substantially. We observed a 6-month mortality of 3% among anaemic patients, compared to 11% and 27% in the studies by Silvis and Kai Liu. Several factors may explain this discrepancy in mortality. In the study by Silvis et al., both coma and cancer were more prevalent (11% and 17%, respectively) than in the current study (5% and 5%), both of which are established predictors of mortality in CVT. In the study by Kai Liu et al., the rate of coma was also considerably higher than in our study. This difference in clinical severity may be explained by the fact that some of the more severe cases were not included in DOAC-CVT because of early death (ie, prior to start of oral anticoagulation) or because patients were not started on oral anticoagulation within 30 days, for instance because of cancer or difficulty swallowing.
The majority of patients with anaemia were from middle-income countries, likely reflecting the higher prevalence of anaemia in these regions due to nutritional, socioeconomic and public health factors.^26^ Notably, after adjusting for country income level, anaemia remained independently associated with poorer functional outcomes. This suggests that, while country’s income status may influence the incidence of CVT with concomitant anaemia, it does not fully explain the observed association between anaemia and worse CVT outcomes.
The impact of anaemia on functional outcome followed a severity gradient, with moderate to severe anaemia exhibiting a stronger relation than in mild anaemia. This supports the hypothesis that cerebral oxygen delivery becomes critically impaired below a hemodynamic threshold, whereas mild anaemia may be offset by compensatory mechanisms such as increased cardiac output and oxygen extraction.^27^
The effect of anaemia appeared to be more pronounced in women, although this could be due to a reduced statistical power among men. Silvis et al. reported an increased risk in both sexes but did not explore potential sex-specific modifiers.^18^ In related conditions such as acute ischaemic stroke, the association between worse outcomes and female sex appears to be partly attributable to lower haemoglobin levels in women.^28^ Stratification by clinical subgroups typically associated with anaemia showed no significant association with poorer outcomes among patients with cancer, autoimmune disease or older age, whereas a non-significant trend towards worse outcomes was observed in young women. These findings should be interpreted with caution, as small sample sizes likely limited statistical power despite considerable numerical differences in the cancer/autoimmune disease and older patient groups. Furthermore, interpreting outcomes of patients with cancer or autoimmune disease is challenging, as this subgroup includes highly heterogeneous conditions with widely varying prognoses. Further studies are therefore warranted to determine whether anaemia exerts sex-specific effects and whether its impact is significant in patients with cancer or autoimmune disease, as well as to elucidate the mechanisms underlying these potential differences.
Although several biological mechanisms have been proposed through which anaemia may exacerbate neurological injury—such as impaired cerebral oxygen delivery, disrupted autoregulation, endothelial dysfunction and increased inflammation—our observational design precludes determination of their causal involvement.^12–17^ Alternatively, anaemia may reflect underlying frailty or chronic disease, including systemic inflammation, malnutrition, occult malignancy or other comorbid conditions, and thus function as a biological marker rather than a direct mediator of unfavourable outcome. The higher proportion of severe clinical features among CVT patients with anaemia, such as intracerebral haemorrhage, focal neurological deficits, decompressive surgery and ICU admission, could support this hypothesis. However, these features could also be downstream consequences of anaemia itself. In this context, the coexistence of CVT and anaemia may represent a “second-hit,” where anaemia, by impairing oxygen transport and exacerbating cerebral vulnerability, predisposes patients to more severe neurological injury. This, in turn, may lead to worse outcomes, such as intracerebral haemorrhage and neurological deficits, and a greater need for intensive interventions.
It is unknown whether correcting anaemia improves the outcome of patients with CVT. A recent randomized controlled trial did demonstrate that, among patients with acute brain injury and anaemia, a liberal red blood cell transfusion threshold was associated with improved clinical outcomes compared to a restrictive transfusion strategy.^29^ However, extrapolation to CVT is not straightforward. The pathophysiological profile of CVT, characterized by venous congestion and potentially elevated intracranial pressure, may increase patients’ susceptibility to transfusion-related complications, including hyperviscosity and thrombotic propagation.^30^ Nevertheless, the more pronounced association between moderate to severe anaemia and poor functional outcome may suggest that this subgroup could benefit from targeted correction strategies, and this should be investigated in future studies.
Our study has several limitations. Although the DOAC-CVT study was prospectively designed, anaemia was not a predefined primary outcome, limiting causal inferences. Still the rate of missing data of haemoglobin levels was low (4%). However, additional details, including cause of anaemia and additional laboratory values such as MCV, and data on anaemia interventions were not collected. Second, although we adjusted for several potential confounders, residual confounding cannot be excluded, either due to baseline imbalances or unmeasured variables that may partly explain the observed association between anaemia and poor outcomes. Third, the absence of patients included from low-income countries, where anaemia is generally more common, and the exclusion of pregnant women limit generalizability of the findings to these populations. Fourth, we did not have information on the underlying causes of anaemia, and therefore were unable to perform stratified analyses by anaemia type. Fifth, we lacked information on longitudinal changes in haemoglobin levels or on anaemia correction during follow-up, both of which may have influenced clinical outcome. Sixth, because cancer is not systematically screened for in patients with CVT, underreporting of malignancy is possible. Finally, the described population does not represent the entire spectrum of CVT patients, as it is limited to those who progressed to oral anticoagulation, potentially resulting in the preferential inclusion of less severe cases.
In conclusion, we found that anaemia is associated with poor functional outcome in patients with CVT. The association was more pronounced in patients with moderate to severe anaemia. Further studies are needed to determine whether correcting anaemia at baseline improves the outcome of patients with CVT.
Supplementary Material
aakag006_Supplemental_material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kim J, Martinez C, Sirotkin I. Cerebral venous thrombosis. Fed Pract. 2017;34:33-37PMC 637044030766287 · pubmed ↗
- 2Ferro JM, Canhao P, Stam J, et al. Prognosis of cerebral vein and dural sinus thrombosis: results of the international study on cerebral vein and Dural sinus thrombosis (ISCVT). Stroke. 2004;35:664-670. 10.1161/01.STR.0000117571.76197.2614976332 · doi ↗ · pubmed ↗
- 3Duman T, Uluduz D, Midi I, et al. A Multicenter study of 1144 patients with cerebral venous thrombosis: the VENOST study. J Stroke Cerebrovasc Dis. 2017;26:1848-1857. 10.1016/j.jstrokecerebrovasdis.2017.04.02028583818 · doi ↗ · pubmed ↗
- 4Korathanakhun P, Sathirapanya P, Geater SL, et al. Predictors of hospital outcome in patients with cerebral venous thrombosis. J Stroke Cerebrovasc Dis. 2014;23:2725-2729. 10.1016/j.jstrokecerebrovasdis.2014.06.02025307433 · doi ↗ · pubmed ↗
- 5Salottolo K, Wagner J, Frei DF, et al. Epidemiology, endovascular treatment, and prognosis of cerebral venous thrombosis: US Center study of 152 patients. J Am Heart Assoc. 2017;6:6. 10.1161/JAHA.117.005480 PMC 566917128611097 · doi ↗ · pubmed ↗
- 6Klein P, Shu L, Nguyen TN, et al. Outcome prediction in cerebral venous thrombosis: the IN-R Ev ASC score. J Stroke. 2022;24:404-416. 10.5853/jos.2022.0160636221944 PMC 9561213 · doi ↗ · pubmed ↗
- 7Coutinho JM, Zuurbier SM, Gaartman AE, et al. Association between anemia and cerebral venous thrombosis: case-control study. Stroke. 2015;46:2735-2740. 10.1161/STROKEAHA.115.00984326272383 · doi ↗ · pubmed ↗
- 8Cardenas-Cruz AF, Ricaurte-Fajardo A, Andrade S, et al. Clinical characterization and predictors of poor outcome in patients with cerebral venous thrombosis: experience from a Latin American cohort. J Stroke Cerebrovasc Dis. 2025;34:108471. 10.1016/j.jstrokecerebrovasdis.2025.10847141093053 · doi ↗ · pubmed ↗